Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
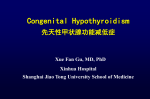
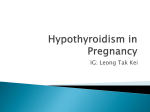
References 1Spencer CA, Takeuchi M and Kazarosyan M. Current status and performance goals for serum thyrotropin (TSH) assays. Clinical Chemistry 1996;42:141-145. 2Rawlins, ML, Roberts, WL Performance characteristics of six third-generation assays for thyroid stimulating hormone. 2004 Clin Chem 50:12 2338-2344. 3Evolution of TSH Assays: A Third Generation Viewpoint. Siemens monograph. 4The National Academy of Clinical Biochemistry: Laboratory Support for the Diagnosis and Monitoring of Thyroid Disease 2002. Laurence M. Demers, Ph.D., F.A.C.B. and Carole A. Spencer Ph.D., F.A.C.B. 5Wardle CA, Fraser WD and Squire CR. Pitfalls in the use of thyrotropin concentration as a first-line thyroid-function test. Lancet 2001;357:1013-4. 6Clinical dialysis Allen R. Nissenson, Richard N. Fine McGraw-Hill Professional, 2005, p 803-818. 7Handbook of dialysis, Volume 236 By John T. Daugirdas, Peter Gerard Blake, Todd S. Ing. Lippincott Williams & Wilkins, Dec 1, 2006. 8 Spectra data. 9 Tietz Textbook of Clinical Chemistry and Molecular Diagnostics, Eisevier, Inc., 4th edition, 2006, p 2062. 10 Henry’s Clinical Diagnosis and Management by Laboratory Methods, Saunders, 21st edition, 2007, p 341. Spectra Laboratories, Inc. 525 Sycamore Drive • Milpitas, CA 95035 • 800-433-3773 8 King Road • Rockleigh, NJ 07647 • 800-522-4662 www.spectra-labs.com Thyroid Stimulating Hormone, 3rd Generation © 2013 Fresenius Medical Care Holdings, Inc. All rights reserved. Spectra and the Spectra logo are trademarks of Fresenius Medical Care Holdings, Inc. or its affiliated companies. All other trademarks are the property of their respective owners. TSHBULLETIN Rev. 3/2013 DISTRIBUTION OF TSH and FT4 IN THE DIALYSIS POPULATION New Test: Thyroid Stimulating Hormone, 3rd Generation TSH 1 0.0 Spectra will no longer offer the current TSH assay because the new TSH3 assay provides the full testing range required for the determination of both hypothyroidism and hyperthyroidism. The American 0.1 Thyroid Association (ATA) currently suggests a third generation TSH as the most cost effective strategy to detect thyroid disease.4 Many clinicians pair 0.01 the TSH with FT4 to recognize euthyroid hyperor hypothyroxinemia. The latter is common in nephrotic syndrome.5 TSH can also be helpful in determining whether an elevated T4 is indicative of hyperthyroidism or is due to decreased proteinbinding site availability.4 The benefit of TSH3 is that, unlike 2nd generation TSH assays, TSH3 can measure levels below 0.020 mIU/L and can be used to distinguish the extremely low levels of TSH suppression of Graves’ disease from the less severely suppressed TSH of non-thyroid illnesses.4 Reference Range According to the ATA, >95% of the normal population will have a TSH level below 2.5 mIU/L with an average TSH level of approximately 1.5 mIU/L.4 Spectra has validated a TSH reference range of 0.300-3.000 mIU/L, which is also the range recommended by the American Association of Clinical Endocrinologists (AACE). The ESRD population includes about 20% of individuals with TSH of up to 20 mIU/L and a normal free T4 consistent with non-thyroidal illness. Persistant TSH values over 20 mIU/L usually indicitive of hypothyroid ESRD patients with true are hypothyroidism develop condition persistent values above 20 mIU/L. Although the average level of TSH in the general population is approximately 1.5 mIU/L, the mean TSH in the dialysis population is higher, with a significantly greater variation, compared to the general population. Free thyroid hormone can increase temporarily due to inflammation and following the administration of heparin due to the competition for the carrier proteins binding sites.10 20% of dialysis patients have TSH levels between 5-20 mIU/L and appear not to be related to thyroid disease DISTRIBUTION OF TSH and FT4 IN THE DIALYSIS POPULATION TSH and the Dialysis Patient The effects of uremia on dialysis patients are Reference Ranges sometimes indistinguishable from symptoms of Free T4: 0.89 - 1.76 ng/dL 6 TSH: 0.300-3.000 hypothyroidism. Peritoneal and hemodialysis do mIU/L not directly affect the thyroid hormone levels, but 0.5 1.0 in peritoneal 1.5 2.0 lead to 2.5 a loss of protein dialysis can a decrease in the total thyroxin levels.7 Dialysis patients may have decreased FT3 and FT4, and increased TSH levels and still be euthyroid.6 Abnormal thyroid results in dialysis patients are more commonly due to abnormal protein levels, malnutrition, or non-thyroid intercurrent illnesses than to actual thyroid dysfunction.6 Although decreases in thyroid hormones are generally associated with non-thyroid disease and malnutrition, dialysis patient decreases in FT3 are also due to decreased ability to convert FT4 to FT3 at the cellular level.9 1000 FT4 3.0 Persistant TSH values over 20 mIU/L are usually indicitive of hypothyroid condition 100 20% of dialysis patients have TSH levels between 5-20 mIU/L and appear not to be related to thyroid disease 10 Reference Ranges Free T4: 0.89 - 1.76 ng/dL TSH: 0.300-3.000 mIU/L TSH 1000 Spectra Laboratories is pleased to announce the addition of a new test, 3rd Generation Thyroid Stimulating Hormone (TSH3). This 3rd 100 TSH Generation TSH assay will replace the current assay. TSH3 provides a tenfold improvement in sensitivity over the previous method. In order to be designated a 3rd Generation TSH assay, a TSH 10 method must have a functional sensitivity below 1,2 a 0.020 mIU/L. The detectable limit of Spectra Laboratories’ new 3rd Generation TSH assay has a functional level validated to 0.008 mIU/L.3 1 0.0 0.5 1.0 1.5 2.0 2.5 FT4 3.0 DIALYSIS VS NON DIALYSIS THYROID HORMONES 9.00 8.64 8.00 7.00 FT4: FT3: 6.00 TSH: LITTLE DIFFERENCE DECREASED IN DIALYSIS POPULATION IMPAIRED CONVERSION OF FT4 TO FT3 DECREASED THYROID HORMONE INCREASES TSH 5.00 4.72 4.00 3.00 3.20 2.00 1.00 0.00 2.10 1.13 0.1 1.14 FT4 FT3 TSH NON DIALYSIS 1.13 3.20 4.72 DIALYSIS 1.14 2.10 8.64 0.01 These relatively mild decreases in FT3 and FT4 levels are not usually related to hypothyroidism but may, in part, contribute to the moderately increased TSH as compared to the normal population. Factors related to non-thyroid disease and the dialysis process result in 19-20% of dialysis patients having levels of TSH between 5 and 20 mIU/L.7,8 However, repeatedly decreased levels of FT4 and elevated TSH levels greater than 20 mIU/L may be indicative of true hypothyroidism.6,7 In addition, because of the prevalence of diabetes in the dialysis population, the incidence of primary hypothyroidism is increased (4%) in the ESRD population when compared to the normal population.6 DIALYSIS VS NON DIALYSIS THYROID HORMONES The new TSH3 assay provides the full testing range required for the determination of both hypothyroidism and hyperthyroidism. Reference Range: 0.300-3.000 mIU/L 9.00 Factors related to non-thyroid disease and the dialysis process result in 8.64 19-20% of dialysis patients having levels of TSH between 5 and 20 mIU/L.7,8 8.00 However, repeatedly decreased of FT4 and elevated TSH levels greater FT4: levels LITTLE DIFFERENCE 7.00 FT3: DECREASED IN DIALYSIS POPULATION 6,7 than 20 mIU/L may be indicative IMPAIRED of trueCONVERSION hypothyroidism. OF FT4 TO FT3 6.00 5.00 TSH: DECREASED THYROID HORMONE INCREASES TSH DISTRIBUTION OF TSH and FT4 IN THE DIALYSIS POPULATION New Test: Thyroid Stimulating Hormone, 3rd Generation TSH 0.0 Spectra will no longer offer the current TSH assay because the new TSH3 assay provides the full testing range required for the determination0.1of both hypothyroidism and hyperthyroidism. The American Thyroid Association (ATA) currently suggests a third generation TSH as the most cost effective strategy to detect thyroid disease.4 Many clinicians0.01 pair the TSH with FT4 to recognize euthyroid hyperor hypothyroxinemia. The latter is common in nephrotic syndrome.5 TSH can also be helpful in determining whether an elevated T4 is indicative of hyperthyroidism or is due to decreased proteinbinding site availability.4 The benefit of TSH3 is that, unlike 2nd generation TSH assays, TSH3 can measure levels below 0.020 mIU/L and can be used to distinguish the extremely low levels of TSH suppression of Graves’ disease from the less severely suppressed TSH of non-thyroid illnesses.4 Reference Range According to the ATA, >95% of the normal population will have a TSH level below 2.5 mIU/L with an average TSH level of approximately 1.5 mIU/L.4 Spectra has validated a TSH reference range of 0.300-3.000 mIU/L, which is also the range recommended by the American Association of Clinical Endocrinologists (AACE). The ESRD population includes about 20% of individuals with TSH of up to 20 mIU/L and a normal free T4 consistent with non-thyroidal illness. Persistant TSH values over 20 mIU/L usually indicitive of hypothyroid ESRD patients with true are hypothyroidism develop condition persistent values above 20 mIU/L. Although the average level of TSH in the general population is approximately 1.5 mIU/L, the mean TSH in the dialysis population is higher, with a significantly greater variation, compared to the general population. Free thyroid hormone can increase temporarily due to inflammation and following the administration of heparin due to the competition for the carrier proteins binding sites.10 20% of dialysis patients have TSH levels between 5-20 mIU/L and appear not to be related to thyroid disease DISTRIBUTION OF TSH and FT4 IN THE DIALYSIS POPULATION TSH and the Dialysis Patient The effects of uremia on dialysis patients are Reference Ranges sometimes indistinguishable from symptoms of Free T4: 0.89 - 1.76 ng/dL 6 TSH: 0.300-3.000 hypothyroidism. Peritoneal and hemodialysis do mIU/L not directly affect the thyroid hormone levels, but 0.5 1.0 in peritoneal 1.5 2.0 lead to 2.5 a loss of protein dialysis can a decrease in the total thyroxin levels.7 Dialysis patients may have decreased FT3 and FT4, and increased TSH levels and still be euthyroid.6 Abnormal thyroid results in dialysis patients are more commonly due to abnormal protein levels, malnutrition, or non-thyroid intercurrent illnesses than to actual thyroid dysfunction.6 Although decreases in thyroid hormones are generally associated with non-thyroid disease and malnutrition, dialysis patient decreases in FT3 are also due to decreased ability to convert FT4 to FT3 at the cellular level.9 1000 FT4 3.0 Persistant TSH values over 20 mIU/L are usually indicitive of hypothyroid condition 100 20% of dialysis patients have TSH levels between 5-20 mIU/L and appear not to be related to thyroid disease 10 Reference Ranges Free T4: 0.89 - 1.76 ng/dL TSH: 0.300-3.000 mIU/L TSH 1000 Spectra Laboratories is pleased to announce the addition of a new test, 3rd Generation Thyroid Stimulating Hormone (TSH3). This 3rd 100 Generation TSH assay will replace the current TSH (Highly Sensitive) assay. TSH3 provides a tenfold improvement in sensitivity over the previous method. In order to be designated a 3rd Generation 10 TSH assay, a TSH method must have a functional 1,2 sensitivity below a 0.020 mIU/L. The detectable limit of Spectra Laboratories’ new 3rd Generation TSH assay has a functional level validated to 0.008 1 mIU/L.3 1 0.0 0.5 1.0 1.5 2.0 2.5 FT4 3.0 DIALYSIS VS NON DIALYSIS THYROID HORMONES 9.00 8.64 8.00 7.00 FT4: FT3: 6.00 TSH: LITTLE DIFFERENCE DECREASED IN DIALYSIS POPULATION IMPARIED CONVERSION OF FT4 TO FT3 DECREASED THYROID HORMONE INCREASES TSH 5.00 4.72 4.00 3.00 3.20 2.00 1.00 0.00 2.10 1.13 0.1 1.14 FT4 FT3 TSH NON DIALYSIS 1.13 3.20 4.72 DIALYSIS 1.14 2.10 8.64 0.01 These relatively mild decreases in FT3 and FT4 levels are not usually related to hypothyroidism but may, in part, contribute to the moderately increased TSH as compared to the normal population. Factors related to non-thyroid disease and the dialysis process result in 19-20% of dialysis patients having levels of TSH between 5 and 20 mIU/L.7,8 However, repeatedly decreased levels of FT4 and elevated TSH levels greater than 20 mIU/L may be indicative of true hypothyroidism.6,7 In addition, because of the prevalence of diabetes in the dialysis population, the incidence of primary hypothyroidism is increased (4%) in the ESRD population when compared to the normal population.6 DIALYSIS VS NON DIALYSIS THYROID HORMONES The new TSH3 assay provides the full testing range required for the determination of both hypothyroidism and hyperthyroidism. Reference Range: 0.300-3.000 mIU/L 9.00 Factors related to non-thyroid disease and the dialysis process result in 8.64 19-20% of dialysis patients having levels of TSH between 5 and 20 mIU/L.7,8 8.00 However, repeatedly decreased of FT4 and elevated TSH levels greater FT4: levels LITTLE DIFFERENCE 7.00 FT3: DECREASED IN DIALYSIS POPULATION 6,7 than 20 mIU/L may be indicative IMPARIED of trueCONVERSION hypothyroidism. OF FT4 TO FT3 6.00 5.00 TSH: DECREASED THYROID HORMONE INCREASES TSH References 1Spencer CA, Takeuchi M and Kazarosyan M. Current status and performance goals for serum thyrotropin (TSH) assays. Clinical Chemistry 1996;42:141-145. 2Rawlins, ML, Roberts, WL Performance characteristics of six third-generation assays for thyroid stimulating hormone. 2004 Clin Chem 50:12 2338-2344. 3Evolution of TSH Assays: A Third Generation Viewpoint. Siemens monograph. 4The National Academy of Clinical Biochemistry: Laboratory Support for the Diagnosis and Monitoring of Thyroid Disease 2002. Laurence M. Demers, Ph.D., F.A.C.B. and Carole A. Spencer Ph.D., F.A.C.B. 5Wardle CA, Fraser WD and Squire CR. Pitfalls in the use of thyrotropin concentration as a first-line thyroid-function test. Lancet 2001;357:1013-4. 6Clinical dialysis Allen R. Nissenson, Richard N. Fine McGraw-Hill Professional, 2005, p 803-818. 7Handbook of dialysis, Volume 236 By John T. Daugirdas, Peter Gerard Blake, Todd S. Ing. Lippincott Williams & Wilkins, Dec 1, 2006. 8 Spectra data. 9 Tietz Textbook of Clinical Chemistry and Molecular Diagnostics, Eisevier, Inc., 4th edition, 2006, p 2062. 10 Henry’s Clinical Diagnosis and Management by Laboratory Methods, Saunders, 21st edition, 2007, p 341. Spectra Laboratories, Inc. 525 Sycamore Drive • Milpitas, CA 95035 • 800-433-3773 8 King Road • Rockleigh, NJ 07647 • 800-522-4662 www.spectra-labs.com Thyroid Stimulating Hormone, 3rd Generation © 2013 Fresenius Medical Care Holdings, Inc. All rights reserved. Spectra and the Spectra logo are trademarks of Fresenius Medical Care Holdings, Inc. or its affiliated companies. All other trademarks are the property of their respective owners. TSHBULLETIN Rev. 3/2013