Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Journal of Pedialric Psychology. Vol. 21, No. 2. 1996, pp. 153-173
Conceptual and Methodologic Issues in Quantifying
Perceptual Accuracy in Childhood Asthma1
Gregory K. Fritz2 and Albert Yeung
Brown University/Rhode Island Hospital
Marianne Z. Wamboldt
University of Colorado!National Jewish Center for Immunology and Respiratory Medicine
Anthony Spirito and Elizabeth L. McQuaid
Brown University/Rhode Island Hospital
Robert Klein
University of Texas Health Science Center at Tyler
Ronald Seifer
Brown University/Bradley Hospital
Received September 16, 1994, accepted June I, 1995
Delineated methodologic issues in the study of symptom perception in childhood
asthma. A review of past and recent psychophysiological and clinical studies of
both adults and children presents the methodologic and analytic approaches that
have been applied to quantify perceptual accuracy. Peak expiratory flow rate,
forced expiratory volume in the first second, and force expiratory flow can serve
as objective measures of asthma. A visual analog scale, a numerical guess, and a
categorical description as subjective measures all have clear strengths and weaknesses. Correlational analysis of subjective-objective data, arithmetic differences between subjective guess and objective value, and an error grid categori'This work was supported by the National Heart, Lung, and Blood Institute Grant RO1-HL45I57,
Gregory K. Fritz. Principal Investigator.
AII correspondence should be sent to Gregory K. Fntz, Child and Family Psychiatry, Rhode Island
Hospital, 593 Eddy Street, Providence, Rhode Island 02903.
153
2
0146-8693/96/W00-01J3J09 50/0 O 1996 Plenum Publiihing Corpomion
154
Fritz et al.
zation can each be applied to calculate an accuracy index on an individual
subject. Illustrative examples reveal that the same data lead to different indices
depending on the method chosen. Empirical research is needed to standardize
various methodologic approaches. Given the increasing prevalence, severity,
and morbidity of pediatric asthma, the study of symptom perception may be a
critical component in our understanding of asthma management, and will likely
lead to useful clinical interventions.
KEY WORDS: symptom perception; asthma; perceptual accuracy.
Asthma is not only the most common chronic illness of childhood, but despite
considerable improvement in the many aspects of asthma treatment, the prevalence, severity, and mortality related to this illness are on the rise. The prevalence of asthma in American children 18 years or younger increased nearly 40%
from 1981 to 1988—an increase that translates into approximately 2.7 million
children (Taylor & Newacheck, 1992; Weitzman, Gortmaker, Sobol, & Perrin,
1992). Furthermore, from 1980 to 1987, the asthma mortality rate increased 42%
in children under age 20, with the highest increase in poor, urban, minority
children (Evans, 1992; Weiss, Gergen, & Crain, 1992; Weiss & Wagener, 1990).
In addition to the risk of death, there is a high risk of morbidity from pediatric
asthma. Asthma accounts for 30% of pediatric hospitalizations (Gortmaker &
Sappenfield, 1984), for approximately one third of school absences (Weitzman, Klerman, Lamb, Menary, & Alpert, 1982), and for numerous other psychosocial complications including reduced participation in sports and extracurricular
activities (Nocon, 1991).
Psychiatrists and psychologists have studied psychosomatic aspects of bronchial asthma for decades. Specific emotional conflicts (French & Alexander,
1941); separation issues (Purcell et al., 1969), temperament (Kim, Ferrara, &
Chess, 1980), family systems (Minuchin et al., 1975), personality (Glasberg,
Bromberg, Stein, & Luparello, 1969), and psychopathology (Tietz, Kahlstrom,
& Cardiff, 1975) have all been explored over the years as causal or contributory
factors in asthma. It has been established that children with asthma and psychological problems have asthma that is more difficult to control. They require more
concurrent antiasthma medication, especially corticosteroids (Fritz & Overholser, 1989), require a greater number of emergency room visits (Dirks et al.,
1977), hospitalizations (Baron et al., 1986; Fritz & Overholser, 1989), and
longer hospitalizations (Strunk, Mrazek, Fuhrmann, & LaBrecque, 1985), exhibit poorer compliance with oral theophylline (Christiaanse, Lavigne, & Lemer,
1989), and more frequently die of asthma (Kravis, 1987; Sears & Rea, 1987;
Strunk, 1987). The early clinical work in this area that tried to establish an
asthmatic personality type (Sperling, 1968) has been largely discounted, and
there is now solid evidence documenting the heterogeneity of personality styles
Perceptual Accuracy in Childhood Asthma
155
and psychosocial difficulties found in patients with asthma (Kinsman, Dirks, &
Jones, 1982; Mrazek, 1988). Yet despite general understanding that psychosocial
problems are associated with more morbidity and mortality, few studies have
been able to demonstrate which specific psychological processes are most critical
in influencing asthma outcome, or in documenting that a psychological intervention could ameliorate or prevent morbidity and mortality (Gustafsson, Kjellman,
& Cederbald, 1986; Liebman, Minuchin, & Baker, 1974).
Perhaps more than any other illness, asthma necessitates a working partnership between physician, patient, and family for optimal treatment to take place.
The episodic nature of asthma and the potential for rapid symptom progression
has led to increased emphasis on self-management approaches, including national efforts by the National Heart, Lung and Blood Institute and the National
Institute for Allergy and Infectious Diseases (Mellins, 1989; Parker, Mellins, &
Sogu, 1989). Proper self-management leads to timely treatment and reduces the
risk of iatrogenic problems and medication side effects. Some reports describe
noncompliance or delay in seeking emergency care as major "avoidable" factors
linked to the increase in asthma deaths (Kravis, 1987; Kravis & Kolski, 1985;
Sears, 1988; Sears & Rea, 1987; Strunk et al., 1985). This finding makes selfmanagement efforts especially salient.
The purpose of this review is to examine, from a conceptual perspective,
one key component of the self-management process: accurate perception of
asthma symptoms. We start by reviewing psychological and physiological factors
hypothesized to affect perceptual accuracy in asthma and review the scant empirical data on this topic. Having reviewed what is known, we (a) propose a
definition of perceptual accuracy in asthma; (b) examine existing objective and
subjective assessment approaches that have been utilized in both clinical practice
and the research literature; and (c) discuss pros and cons of different indices of
perceptual accuracy that may be used by clinicians and researchers when working with asthma patients. We conclude with a discussion of the clinical and
research implications of symptom perception for asthma management.
PSYCHOLOGICAL AND PHYSIOLOGIC FACTORS AFFECTING
PERCEPTUAL ACCURACY
Inaccurate perception of asthma symptoms, which may occur for a variety
of reasons, may be one common mechanism whereby a variety of psychosocial
problems lead to out-of-control, or even fatal, asthma. The accurate perception
of changes in respiratory function and consequent appropriate initiation of selfmanagement is a complex skill. First, there must be a perceptual capability to
detect airway changes. This capability requires intact proprioceptive neurons in
the lungs and respiratory muscles, and unimpaired neuronal pathways to the
156
Fritz ct al.
brain. Second, the person must be motivated and able to pay attention to these
inputs. Third, the individual must accurately distinguish which perceptions correspond to changes in respiratory function due to bronchoconstriction versus
which perceptions are due to changes in anxiety levels, emotional distress, pain,
or other illness. Finally, the person must have the cognitive skills, knowledge,
and the motivation to initiate an appropriate sequence of self-care assessments
and treatments.
The ability to focus attention on respiratory changes may vary between
person as well as within persons, although empirical studies of relevant factors
are scarce. For example, it seems plausible that children with ADHD may have
more difficulty than other children. The severity of their current psychological
symptoms may interfere with attention. Likewise, concurrent stressors and resultant anxiety or dysphoria may either distract attention from respiratory sensations
or lead to enhanced focus and hypersensitivity to them. In chronic pain patients,
for example, the threshold for detecting and complaining of pain is lowered when
there is concurrent depression (Roy, Thomas, & Matas, 1984).
The ability to distinguish physical sensations from emotional states is likely
dependent on a number of factors, including familial teaching or modeling,
cultural input, and genetic predisposition. Developmentally, younger children
often complain of somatic symptoms when they feel distressed for emotional
reasons (Campo & Fritsch, 1994), in part because they have not yet learned to
sort out the different states. This ability requires a family culture (Fabrega, 1990)
that helps teach children to distinguish between physical and psychological distress, as well as to express it. Patients with somatization disorders appear to have
a different neuropsychologic makeup that includes a lower threshold for experiencing bodily sensations coupled with a difficulty expressing emotional states
which has been termed "alexithymia" (Barsky, Goodson, Lane, & Cleary, 1988).
Certain psychological factors, such as depression or anxiety, may affect an
individual's motivation to intervene when symptoms are perceived. Abnormalities in the autonomic nervous system may be synergistic in depression and
asthma (Miller, 1987). Anxiety has been documented to interfere with accurate
labeling of symptoms as well as motivation to initiate appropriate action. Kinsman and associates (Dirks & Kinsman, 1981; Dirks, Schraa, Bron, & Kinsman,
1980) have shown that adult asthmatics who are high or low on a "panic-fear"
dimension have more hospitalizations than those who score in the moderate
range. In this work, low anxiety was hypothesized to lead to delay in seeking
treatment; high anxiety levels were associated with poor discernment between
respiratory and anxiety-related symptoms, leading to overutilization of treatment. This work was partially replicated in children (Baron et al., 1986). Others
have reported an association between poor perception of respiratory sensation
and a defensive style of repression (Steiner, Higgs, & Fritz, 1987).
There is a pertinent and substantial body of basic research in which well-
Perceptual Accuracy in Childhood Asthma
157
established methods of psychophysics (the study of the relationship between a
physical stimulus and the sensation of it) have been adapted to assess sensory
thresholds in respiration. Although this research to date has only involved adults
and has not been related to clinical problems or settings, the findings have some
relevance for the study of perceptual accuracy. In a typical study, added resistive
loads of varying magnitude are applied with a breathing apparatus for one or
several breaths, separated by "unloaded" breaths. The sensory threshold is defined as the smallest added resistance that can consistently be detected.
Individual adult subjects have been found to differ in their threshold for
detecting the added load; children have not been studied. Passive respiration is
associated with less accurate resistance detection than active respiration, indicating that active contraction of the respiratory muscles is essential in the detection
of resistance (Killian, Mahutte, & Campbell, 1980). Research has also shown
consistent findings whether the change in resistance occurs in the bronchial tree
or at the mouth (Zechman & Wiley, 1986), suggesting that the perceptual process
involves receptors in extrathoracic and intrathoracic airways plus muscles of the
chest. In other experiments, airway anesthesia has not been found to alter load
detection thresholds (Chaudhary & Burki, 1980).
In studies that have examined the effect of age on respiratory sensation,
older adults seem less able to perceive added respiratory loads than younger
adults (Akiyama, Nishimura, Kobayashi, Yamamoto, & Miyamoto, 1993; Tack,
Altose, & Chemiack, 1981). Variability in resistive load detection threshold is
rather small from one assessment to the next in a given adult. Variability is much
larger among adults. In one study, normal adults showed only 7% within-subject
variation but 230% variation in threshold level between subjects (Killian, Mahutte, & Campbell, 1981).
Despite the promising results in some of the basic research and the logical
appeal of the relevance of perceptual accuracy to clinical management of asthma,
few studies have been conducted with actual patients. Rubinfeld and Pain (1976),
using a methacholine challenge, found that 15% of adult asthmatics were unable
to sense even marked airway obstruction. Burki, Mitchell, Chaudhary, and Zechman (1978) found adult patients to vary markedly in their ability to detect added
resistive loads. Ergood, Epstein, Ackerman, and Fireman (1985) found no differences between adult asthmatics' and nonasthmatics' perception of respiratory
function at rest or after moderate exercise. In the only study to date that deals
with pediatric asthma patients, Sly, Landau, and Weymouth (1985) found no
relationship between actual forced expiratory volume in the first second (FEV,)
and subjective ratings of FEV, in a group of children with asthma before or after
an educational program. However, this study was compromised by its reliance on
a single measure of subjective/objective correspondence obtained only twice,
before and after the intervention.
More recently, there have been three studies suggesting that impaired symp-
158
Fritz et at.
torn perception may be a salient factor in predicting asthma outcome. Kikuchi,
Okabe, and Tamura (1994) have demonstrated that the lack of perception of
dyspnea is associated with near-fatal attacks of asthma in adults. Similarly,
disregard of asthma symptoms is a factor that differentiated between children
who eventually died from their asthma and those with equally severe asthma who
did not die (Strunk et al., 1985; Zach & Karner, 1989).
Although this line of work is promising, it has been limited thus far by small
samples and imprecise measurements of perceptual accuracy of respiratory symptoms. Before more work can be done to elucidate the numerous processes involved
in the development and maintenance of symptom perception, a standardized and
sensitive means of assessing respiratory sensation must be developed.
Definition of Perceptual Accuracy
We propose that a useful definition of perceptual accuracy is the degree to
which subjective assessment of asthma symptomatology/severity corresponds
with an objectively measured rating of severity. This definition implies an individual pattern that is determined from multiple observations of the correspondence between subjective and objective measurement. It also requires an objective change in respiratory status. Thus, an extremely accurate person is one who
can subjectively distinguish small changes in physiologic function. Symptom
perception accuracy is conceived to have both state-dependent and stable characteristics. Clinical experience (but as yet no empirical evidence) suggests that
there is some stability in perceptual accuracy at least over a several week period;
stability over longer periods (e.g., year-to-year) is unknown. Changes in this
ability over development (e.g., from latency age to adolescence) have not been
studied. Accuracy may also vary with situational changes such as the severity of
an asthma episode, the setting (outdoors vs. doctor's office), or the level of
psychological stress. The number and frequency of ratings needed to determine
an individual's level of accuracy have yet to be determined by clinical study, but
both symptomatic and symptom-free periods should be included.
Objective Measurement of Respiratory Status
Pulmonary physiologists have developed numerous indices and ratios that
use volume, pressure, and flow measurements to describe function at various
points in the respiratory cycle. In pediatric practice the number of frequently
utilized indices is much smaller, but a single, validated "gold standard" does not
exist. By far the most commonly used objective measure is the peak expiratory
flow rate (PEFR). This National Institute of Health (Mellins, 1989) "Guidelines
for the Diagnosis and Management of Asthma" has recommended regular mon-
Perceptual Accuracy in Childhood Asthma
159
itoring of PEFR. The major reason for the ubiquity of PEFR is ease and economy of measurement; PEFR is easily assessed with an inexpensive, hand-held
peak flow meter. No other pulmonary function test approaches the technological
simplicity of PEFR. Predicted normal values are available based on height,
gender, and ethnicity, but individually determined baseline normal values are
preferable for clinical use. Most children quickly leam their typical normal
range. Disadvantages of using PEFR as the objective measure of asthma include the fact that it is highly effort-dependent and that there may be considerable variability between different brands of hand-held meters (Eichenhom,
Beauchamp, Harper, & Ward, 1982). Further, recent data suggest that because
PEFR measures predominantly large airway function, a subgroup of children
whose asthma involves primarily peripheral airways may not be monitored
appropriately with PEFR (Klein, Fritz, Yeung, McQuaid, & Mansell, in
press).
A reasonable alternative to PEFR is the FEV,. This test is somewhat less
effort-dependent than PEFR and may provide a more "complete" picture of lung
function. Currently, FEV, is obtained only through full spirometry requiring
more sophisticated and expensive equipment, careful monitoring, and physician
interpretation. These factors limit the usefulness of FEV, in the clinical assessment of perceptual accuracy for they preclude easy self-monitoring.
The forced expiratory flow in the midportion of a breath (FEF^.-^) primarily measures small airway function and is much less effort-dependent than PEFR.
Like FEV,, it can only be measured with spirometry equipment. FEF^,-^ is an
especially important index of asthma severity in the subgroup of children whose
acute asthma episodes are characterized by peripheral airway compromise.
Subjective Assessment of Respiratory Symptoms
One of the most straightforward approaches to subjective quantification of
symptoms is to ask patients to predict, based on their present asthma symptoms,
what their objective pulmonary function test result would be at that moment.
This is a reasonable approach to subjective assessment because PEFR monitoring
is increasingly common among patients with asthma and the PEFR values are
readily understood by both patients and physicians. Many asthma patients now
monitor PEFR at home and are familiar with their personal range in readings.
Thus, they have sufficient practice and feedback to help shape subjective assessments. For research purposes, the subjective and objective assessments are expressed in the same units, making analyses easily understood.
There are several potential disadvantages to subjective prediction of PEFR
values. First, PEFR may not be a sensitive enough measure of pulmonary function for some children. Klein et al. (in press) found a significant number of
160
Fritz et al.
children (17%) had normal PEFR values even when they were clinically symptomatic. FEF 23 _ 75 was a more sensitive objective index of pulmonary functioning for this subgroup of asthmatic children. A second disadvantage of the PEFR
prediction approach stems from the observation that many developmentally
younger children think of illness in categorical terms—"healthy," "sick," "not
too good," and so forth. To express their status in continuous numbers may be a
cognitive challenge for young children. Finally, whether PEFR or F E F ^ v s is
used as the objective index, there can be a recency effect to the prediction
process. That is, some patients—especially younger, cognitively concrete
children—may tend to guess the same value as they did on the last occasion.
This effect can lead to an artifactually accurate (or inaccurate) guess that does not
reflect an actual assessment of physiologic state.
A second approach to subjective assessment is the use of a visual analog
scale (VAS). With a VAS, a patient picks a rating from a 100-mm line that may or
may not have verbal or pictorial anchors. For example, one end of the line might
be the rating "terrible asthma" and the other end, "no symptoms"; the patient
marks the line somewhere in-between. In another type of VAS, pictorial anchors
are used. One such instrument, the Brown Asthma Visual Analog Scale (Fritz,
Spirito, Yeung, Klein & Freedman, 1994) was developed for children with
asthma. In this scale, both verbal anchors and cartoon depictions are used to help
orient a child to the use of the scale.
The advantage of a VAS is that it requires summation of symptoms and a
judgment, which means that it is more global. The "gut feeling" reflected in such
a global assessment may very well be the real basis for subsequent action or
inaction in asthma self-management. Because it is continuous, one can look for
small changes in symptomatology detected by the patient. One disadvantage of a
VAS is that it requires the ability to use a combination of verbal or pictorial
anchors and a proportional spatial relationship between anchors, making the
approach clearly inappropriate for developmentally immature children with preoperational cognitive abilities. Further, patients develop response sets; for example, they may consistently rank extremes. Others do not use the extremes of the
scales but, instead, develop a response set that truncates the use of potential
values. In these cases, the advantages of the VAS are minimal unless the patient
is reeducated to the use of the scale.
A third approach to subjective assessment is categorical description. In this
type of approach, a simple scale may be used. For example, five verbal descriptors might represent choices to describe asthma symptomatology (e.g., none, a
little, some, pretty bad, or awfully bad—the worst). Such categorical descriptors
have an advantage because they are commonly used in everyday life. Descriptors
may be more understandable than a VAS and the wording can be changed and
defined by the investigator to ensure proper understanding of the terminology by
a particular population. Although categorical scales commonly employ verbal
Perceptual Accuracy in Childhood Asthma
161
descriptors, they can also use pictorial descriptors for young children, such as the
FACES scale used by children to quantify pain (McGrath, 1987). The disadvantage to the categorical approach is the limited variability; it discourages attempts
at distinguishing subtle differences in symptomatology. In addition, categories
may not have the same meaning across patients. There may also be intraindividual variation in rating tendencies that are more problematic when using a
scale with a small number of points.
A fourth approach to assessing symptomatology is to ask the patient what
treatment is indicated by symptomatology. In other words, the symptoms are
categorized on the basis of the extent of treatment needed: inhaler versus nebulized medications versus urgent visit to the physician. The advantage to such a
rating system is that it is clinically relevant and easily understood by patients who
are knowledgeable in self-management techniques. A major disadvantage to
such an approach is that it confounds treatment knowledge and judgment, and
perception of illness. A child who perceives pulmonary changes adequately but
lacks self-management knowledge would be incorrectly classified regarding perceptual ability using this approach. In addition, utilizing treatment categories
means this method has the same problems as other categorical approaches.
Finally, treatment plans can vary between one physician and another, making it
hard to compare across practices or in research populations.
DEVELOPMENTAL CONSIDERATIONS IN OBJECTIVE
AND SUBJECTIVE ASSESSMENT
In clinical practice, the treating physician relies on a symptom report from
the child with asthma and/or the parent regarding pulmonary functioning and
then provides guidelines regarding when and how to manage acute symptoms
according to the overall treatment plan. For the youngest children, this approach
relies almost entirely on the parent's ability to notice symptomatic changes in the
child's presentation. However, this process likely lays the groundwork for the
development of children's own symptom perception, for children are thought to
acquire concepts of health and health skills through repeated opportunities for
practice of these behaviors in the home (Tinsley, 1992).
As children approach school age and begin to have responsibility for monitoring their symptoms, their own ability to attend to changes in respiratory status
and initiate appropriate treatment becomes increasingly important. Recent research demonstrates that with increasing illness knowledge and developmental
progress, school-aged children begin to rely more on internal physiologic cues as
signs of health difficulty (Hergenrather & Rabinowitz, 1991). Experienced physicians find that children as young as 6 years old can reliably use a hand-held
peak flow meter if provided with appropriate instruction and parental monitoring
162
Fritz ct al.
of the procedure (Clark, Evans, & Mellins, 1992). As children progress towards
adolescence, they begin to take more responsibility not only for identifying
symptoms but for self-management. Thus the developmental progression from
the preschooler's total reliance on parental care of their asthma, to the schoolaged child's active participation in symptom identification, to the adolescent's
central position in asthma self-management means that the role and importance
of symptom perception may vary with developmental stage.
The child's age and overall cognitive level should serve as a guide for
choosing the appropriate subjective measurement of current symptomatology.
Some children arc more familiar with either verbal or pictorial categories; others
may be able to effectively use graphs or number lines for a more fine-grained
assessment of symptom state. We have observed that younger children (7 years
and below) are more comfortable using categories. Graphical representation
using a visual analog scale with pictorial anchors is likely the optimal choice for
this younger group (Fritz et al., 1994). Children 8 years and older can often guess
their own peak flows and give a more precise description of how their current
state compares to previous exacerbations. However, there appear to be significant differences in this ability, which may be related to experience, psychological
and/or family factors. Future research is needed to determine more precisely how
these factors change over time and interact with critical developmental transitions.
INDICES OF PERCEPTUAL ACCURACY
Selection of appropriate objective and subjective variables and their measurement at a number of points are essential steps in determining the perceptual
accuracy of a particular patient. The method by which these data are analyzed or
summarized is also an important factor in the determination. Several approaches
are conceptually possible, but they do not necessarily lead to the same classification of perceptual accuracy when applied to an individual patient's data. The
almost total lack of published research studies unfortunately means that previous
work on the utility of a particular approach cannot be cited. Our own work to
date provides the basis for the three approaches which are described briefly; data
from five illustrative cases are then analyzed with each approach. The five cases
were selected because they represent the full range of perceptual ability and their
data sets have different characteristics.
Correlational
If a sufficient number of trials are available, a child's subjective and objective ratings at each point may be statistically correlated; the correlation coeffi-
Perceptual Accuracy in Childhood Asthma
163
cient can be used as an indication of the magnitude of perceptual accuracy for the
given child. The advantages of this correlational approach include the creation of
an index of association that depends little on specific scale properties. Subject
variables (e.g., VAS or "guess" of predicted PFT value) can be standardized and
combined, creating a more stable subjective index to correlate with objective
measurement. This fact may explain why correlation coefficients have been the
most commonly used statistical index in quantifying the accuracy of subjective
perception in asthma research (Fritz, Klein, & Overholser, 1990).
Despite the appeal of such an approach, it is subject to the same limitations
of most correlational methods; a sufficient number of observations are needed for
a valid index, and the correlation is likely to be low if there is insufficient
variability on indices measured. In the latter case, poor perceptual accuracy
could be confused with statistical artifact. Further, low correlations are likely to
contain no information regarding the type of perceptual error, overestimation of
symptoms is indistinguishable from underestimation even though the medical
consequences are very different. Table I summarizes these issues and the overall
variability of correlational analyses of 30 subjective (either VAS ratings or
guesses of PEFR) and objective (PEFR, FEV,, or FEF25_7J) assessments for five
different children with asthma (selected for illustrative purposes). For example,
Subject 2 had VAS ratings that were very restricted, and the correlations with
pulmonary function were poor. Subject 5, in contrast, had a similar mean VAS
rating but more variability (larger SD); the correlation with pulmonary function
was better. Statistical significance testing was done to illustrate the magnitude of
the subjective-objective association reflected in the coefficients obtained.
Arithmetic Differences
When the same specific measurement scales are used for objective and
subjective ratings, the actual value obtained on the objective measure may be
subtracted from the patient's guess that immediately preceded it according to the
formula
Guessed Value - Actual Value
Predicted Value
,..
,._
x 100 = difference.
The Predicted Values in the formula above may be obtained from normative
tables (e.g., Polgar & Romadhaf, 1971). Since normal PFT values depend on the
size of the child, this adjustment to the raw difference score is done to approximately standardize the magnitude of the difference. These difference scores are
then summed over all observations. The mean difference score summarizes the
subject's average guessing error; using the absolute value of the differences
avoids the artifact of errors in opposite directions canceling each other out.
58.7
12.7
5.6
3. F/15
4
.13
-.03
.21
.50'41'
PEFR
(r)h
VAS and
h
.25
.29
40'
.11
93.1
88.3
67.7
75.7
.02
-.12
1.7
70.0
-.06
7.6
4.2
7.7
9.8
SD
Guess
M
(r)
FEF-,,_
,
h 7
VAS and
-.07
-.07
-.16
(r)
FEV,
VAS and
.29
-.06
-.13
-.11
.48'
FbrK
(r)"
Guess and
.46'
.37'
.21
-.21
-.23
{r)
FEV,
h
Guess and
.46'
.38'-
-.10
.30
-.36
{r)
FEF,,_
,
h 7
Guess and
"VAS = visual analog scale rating (mm); PEFR = peak expiratory flow rate; FEV, » forced expiratory volume in the first second; FEF Z ! U 7 , = forced expiratory flow
in the midportion of the breath; Guess = subjective guess of PEFR (in % of expected PEFR).
h
r == correlation coefficient.
• / ' < .05
5. M/12
7.1
16.8
3.3
2.6
12.9
2.7
4.6
1 M/13
2. M/IO
F/IO
50
M
subject
(scx/ugc)
VAS
Table I. Five Illustrative Subjects Demonstrating Variability of Correlations Between Subjective and Objective Data"
165
Perceptual Accuracy In Childhood Asthma
Unlike correlational analysis, an advantage of calculating the arithmetic
differences is that the direction of inaccuracy can be meaningfully indicated. To
depict the magnitude of imprecision in either direction, the sum of overestimations (subjective PFT guess > objective PFT measure) and the sum of underestimations (subjective PFT guess < objective PFT measure) are calculated.
These indices can be interpreted individually or summarized in a ratio:
X overestimation
= Over/Under Ratio
2 underestimation
Because this method relies on mean differences, it is impossible to distinguish between a pattern of multiple small errors or a few large errors. The same
mean value could result from either pattern, and a nonrepresentative outlier can
have an unduly large impact on the final index. This approach is also cumbersome to apply when the subjective and objective variables are not in the same
units. Finally, the arithmetic summary does not deal with the clinical relevance of
the data, as differences of similar magnitude are weighted equally no matter what
the child's clinical status at the time of the measurement.
Table II details the arithmetic summaries of the five illustrative patients'
PEFR data compared to the corresponding guess. Results from correlational
analyses may not agree with results from arithmetic differences approach. In our
selected cases this discrepancy is most obvious regarding Subject 1 who is
categorized as highly accurate with the arithmetic summary and inaccurate using
the correlation coefficients.
Table II. Arithmetic Summary of Subjective Ratings of PEFR
and Objective PEFR Data for Five Illustrative Subjects
Subject
(sex/age)
1.
2.
3.
4.
5.
M/13
M/10
F/15
F/10
M/12
Mean
difference"
(%)
Mean
difTerence"
(absolute
value)
(%)
2 overestimation''
1.8
6.2
-11.6
-0.5
1.5
2.9
11.9
12.2
2.1
6.2
70
272
9
39
115
Over/under ratio
2 overestimation
2 underestimation'' 2 underestimation
16
86
356
54
72
4.4
3.2
0.03
0.72
1.6
/ PEFR Guess - PEFR actual
1 x 100%.
PEFR predicted
/
'Summation of overestimation (subjective PEFR > objective PEFR); numbers adjusted for 30
observations.
•Summation of underestimation (subjective PEFR < objective PEFR); numbers adjusted for 30
observations
"Difference
166
Fritz et al.
Error Grid Analysis
Cox et al. (1985), working with adult patients with diabetes, developed a
graphic system in which a subjective estimate of blood sugar is plotted against
the corresponding actual blood sugar level and then categorized on clinical
grounds. This creative approach may be modified for asthma; the resulting grid
takes the arithmetic summary described above a step further because the grid is
grounded on clinical specifications. The categories on the grid consider the
actual pulmonary status (indicated by the objective measure) and the implications
of decisions for self-management that would be based on the subjective estimate.
Although the grid system could be applied to any pulmonary function variable,
the present status of PEFR makes it the clear choice to use in the development of
the error grid analytic approach. The subjective/objective data for all the observations of a single subject are plotted on a grid.
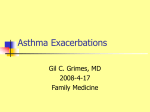
As shown in Figure 1, the grid is divided into several areas. The diagonal is
the line of identity, reflecting perfect subject-objective agreement. The vertical
line at 80% of the child's best value (Self Best) is an arbitrary point at which
PEFR can be considered to reflect clinically significant compromise (N.I.H.,
1991). Zone A (Accurate) includes points for which the subjective estimate is
within ±10% of the actual PEFR. Zones B.O. (Benign Overestimation) and
B.U. (Benign Underestimation) include inaccuracies that have benign consequences in self-management. Zone B.O. includes clinically uncompromised
points in which the subject overestimated PEFR; no intervention is needed or
undertaken. Zone B.U. includes points where a compromised PEFR is exaggerated in the estimate; needed intervention would be vigorously pursued. Zone D
(Dangerous) includes overestimates of clinically compromised PEFR; it is considered dangerous because the need for self-management interventions would be
overlooked. Zone E (Erroneous) reflects the potential for overtreatment since it
includes points at which a normal-range PEFR is perceived as compromised.
The error grid analysis provides a comprehensive display of the degree of
accuracy in a child's subjective estimate, the extent and direction of inaccuracy,
and the clinical risk (or lack thereof) potentially resulting from the specific
inaccuracy. The approach allows the use of Area A alone to reflect overall accuracy. Alternatively, the grid can be used to generate a complete profile of
accurate guesses, overestimations, and underestimations.
The main disadvantage of the error grid analysis stems from the arbitrary
nature of the threshold for PFT abnormality. There is no empirical evidence for
choosing 10%, 20%, or any other decrease from an individual's normal baseline
level of pulmonary functioning as indicative of an asthma episode. Further, it is
essential in using the error grid approach to have an individualized baseline (the
child's persona] best PFT value obtained when completely asymptomatic and
exerting maximal effort) to use in standardizing the objective observations. Pub-
167
Perceptual Accuracy in Childhood Asthma
Estimated PEFR
% predicted
y = 0.9i
Actual PEFR
% predicted
80%
Fig. 1. Grid analysis in the accuracy of PEFR perception. Area A: Accurate area; Subject estimated
PEFRs accurately. Area D: Dangerous area; Subject overestimated PEFRs while having low PEFRs.
Area E: Erroneous area; Subject underestimated PEFRs while having normal PEFRs. Area B.O.:
Benign overestimation area; Subject overestimated PEFRs while having normal PEFRs. Area B.U :
Benign underestimation area; Subject underestimated PEFRs while having low PEFRs.
lished tables only approximate normal values for a given child due to individual
anatomic and functional variation.
Table III summarizes the data for the five illustrative subjects analyzed with
the error grid approach, as indicated by the percentages of their guesses falling in
Zone A. Similar to the findings with the arithmetic approach, Subjects 1 and 4
are the most accurate. Relatively few points fall in the clinically dangerous zone,
with Subjects 1 and 3 having no such observations. The "over/under ratio" is
Table III. Summary of the Error Grid Analysis Results for Five Illustrative Subjects"
Subject
(sex/age)
I.
2.
3.
4.
5.
M/13
M/10
F/15
F/IO
M/12
Zone A
(Accurate)
(%)
Zone D
(Dangerous)
(%)
Zone E
(Erroneous)
(%)
Over/under ratio
_ Zone D + Zone B. O.
Zone E + Zone B. U.
90
51
53
79
58
9.5
11.0
0
10.0
24.0
0
11
9.5
3.5
0
1.0
1.3
48
3
•5
"Zones A, D, E, B.O., and B.U. are described in Figure 1 legend.
A/(D + E)
ratio
9.5
23
LI
6.1
1.5
168
Fritz ct al.
similar to the one obtained in the arithmetic approach, as both reflect a subject's
tendency to err in a consistent direction. Two of five (Subjects 1 and 2) demonstrate degrees of overestimation of pulmonary function more frequently than
underestimation; the other three do not demonstrate a pattern.
CLINICAL IMPLICATIONS
The majority of children with asthma require some objective measurement
of pulmonary function to optimize self-management. Despite some of its drawbacks, PEFR is still the most widely accepted and easily accessible measure.
Hand-held computerized spirometers are now more readily available (e.g., from
Pulmonary Data Service, Louisville, CO), making possible the clinical use of
less effort-dependent indices such as FEV,, orFEF25_75, in the future. Clinicians
can contract with patients and their families to keep a diary of medication usage,
subjective symptom ratings, and the corresponding pulmonary function data.
This undertaking serves to provide useful baseline data while it educates and
structures the family in asthma management.
Although PEFR measurements once or twice daily are commonly recommended by pediatricians, compliance may be a problem—especially when added
to an already complicated regimen of several medications, allergen avoidance,
nasal washes, exercise monitoring, and so forth. For children with documented
poor perceptual accuracy, daily PEFR assessment will continue to be essential.
However, for children who have demonstrated high perceptual accuracy, PEFR
monitoring may be needed only to confirm detected changes. Not only may
compliance with PEFR monitoring be improved, but other aspects of the regimen
may not suffer due to compliance or conflict over how much time needs to be
devoted to asthma.
Demonstrated perceptual accuracy may help the parents and physician trust
the patient to be responsible, thus allowing many children additional independence and control over their asthma. Development of improved accuracy in
symptom perception can be used as an objective indicator of when the child is
ready to take the next step in asthma self-management. Empirical evidence of
their child's perceptual ability may reassure parents and thus prevent the developmental problems associated with overprotection.
Early and accurate perception of asthma symptoms, if linked to timely and
appropriate treatment, should reduce asthma morbidity. With an accepted standardized measurement of respiratory symptom perception, the importance of
accuracy as a predictor of outcome in asthma morbidity and mortality can be
tested. It cannot be assumed that more accuracy will always be associated with
less morbidity or mortality. As was shown to be the case with the panic-fear
construct of Kinsman et al. (1982) or compliance with medical treatments in
Perceptual Accuracy in Childhood Asthma
169
general (Asburn, 1981), it may be that there is an optimal window of accuracy.
Too little accuracy may indeed lead to more emergency room visits and hospitalizations, due to disregard of warning symptoms and delay initiating treatment.
On the other hand, too much sensitivity may extract a price in quality of life: It
may indicate too much focus on the illness and its treatment at the expense of
other areas of development. Consideration of the clinical implications of perceptual accuracy leads to several important questions for which there currently are
no answers: Can perceptual accuracy be enhanced with educational efforts or
motivational programs? Do family characteristics of dealing with physical symptoms affect perceptual accuracy for children with asthma? Will biofeedback
training improve a child's perceptual ability?
RESEARCH IMPLICATIONS
Accuracy of symptom perception is an important component of chronic
pediatric illness, and it is a realm in which the knowledge base of child psychologist and psychiatrists is especially relevant. Although the processes involved in
symptom perception have to date been almost completely ignored in empirical
research on children with asthma or other chronic illnesses, the potential is great
for an improved understanding of perceptual accuracy to enhance medical management. Areas in need of basic research include (a) determinants of perceptual
accuracy and risk factors for inaccuracy; (b) cognitive ability in relation to
perception; (c) the impact of affective state (anxiety or depression) on the perceptual process; (d) the possible role of psychological defenses such as repression
and denial in blunting perception of physical symptoms; and (e) longitudinal
changes across development in perceptual ability. As this review indicates, the
methodology for studying symptom perception in children and adolescents is
currently being developed. A number of choices about objective physiologic
measures, subjective assessment, and analytic approaches are summarized in
Table IV. Consideration of the practicalities involved in data collection, familiarity with children's responses, and clinical judgment are essential in making the
choice. Research comparing the various approaches to quantify perceptual accuracy is needed to empirically determine which is most effective.
As regards subjective assessment, continued research in accuracy of symptom perception should lead to methods to enhance subjective data provided by
children. With the myriad alternatives in subjective assessment, objective assessment, and analytical method, each giving slightly different results, the picture
can at first seem perplexing. The complex picture can be unclouded if we
understand the different assumptions and limitations for each of the analyses:
Correlation analysis assumes a linear relationship between subjective and object
assessment; arithmetic differences may be biased by outliers; and error grid
Fritz et al.
170
TaWe IV. Summary of Methodologic Considerations in Studying Symptom Perception in Asthma
Strengths
Parameter
Objective pulmonary status
PEFR
FEV,
Easy, inexpensive, familiar
Less effort dependent than
PEFR
More complete respiratory
Weaknesses
Effort dependent
Variability in meters
Poor assessment of peripheral
airways
Laboratory measurement only
da La
Subjective estimate
PFT prediction
VAS
Categorical scale
Treatment indicated
Analytic approaches
Correlation
Arithmetic
Error grid
Least effort dependent
Most sensitive PFT—central
and peripheral airways
Laboratory measurement only
Readily understood from
home PEFR monitoring
Same units as objective
Continuous variable difficult
for those who think categorically
Recency effect
Response set
Global judgment obtained
Small changes registered
May be more realistic
Wording can be tailored to developmental level
Clinically relevant—reflects
self-management
Not dependent on absolute
scale properties
Can analyze multiple subjective and/or objective variables
Units irrelevant
Can show direction of error
No artifact with limited variability
Shows direction of error
No artifact with limited variability
Clinically relevant
Limited variability
Categories may not mean the
same to all individuals
Confounds symptom perception with illness knowledge
and judgment
Artifact possible when variability is limited
No directionality of error
Outliers affect the mean
Requires same units for subjective and objective data
Clinical threshold is arbitrary
Valid individual PFT baseline
is essential
Requires same units for subjective and objective data
analysis assigns subjective guesses arbitrarily into zones. With further studies to
refine the definition of the accurate zone and to validate various zones, the error
grid can potentially be a useful research and clinical tool for identifying high risk
asthma patients. Future research in perceptual accuracy should provide a critical
first step in reducing asthma morbidity through the identification of high-risk
patients and the enhancement of appropriate medical interventions.
Perceptual Accuracy in Childhood Asthma
171
REFERENCES
Akiyama, Y., Nishimura. M., Kobayashi. S., Yamamoto, M., & Miyamoto, K. (1993). Effects of
aging on respiratory load compensation and dyspnea sensation. American Review of Respiratory
Disease. 148. 1586-1591.
Asburn. L. (1981). Patient compliance with medication regimens. In S. LJdcomc (Eds.), Biobehavioral medicine Sydney: Cumberland College of Health Sciences.
Baron, C , Lamarre, A., Veilleux, P., Ducharme, C , Spier, S., & Lapierrc, J. G. (1986). Psychomaintenance of childhood asthma: A study of 34 children. Journal of Asthma. 23. 68-79.
Barsky, A. J., Goodson, J. D., Lane, R. S., & Cleary, P. D. (1988). The amplification of somatic
symptoms. Psychosomatic Medicine. 50, 510-519.
Burki. N. K., Mitchell, K., Chaudhary, B. A., & Zechman, F. W. (1978). The ability of asthmatics
to detect added resistive loads. American Review of Respiratory Disease. 117, 71-75.
Campo, J. V., & Fritsch, S. L. (1994). Somatization in children and adolescents. Journal of the
American Academy of Child and Adolescent Psychiatry. 33. 1223-1235.
Chaudhary, B. A., & Burki, N. K. (1980). The effects of anesthesia on detection of added inspiratory
elastic loads. American Review of Respiratory Disease, 122, 635-639.
Christiaanse, M. E., Lavigne, J. V., & Lemer, C. V. (1989). Psychosocial aspects of compliance in
children and adolescents with asthma. Developmental Behavioral Pediatrics, 10. 75-80.
Cox, D. J., Gonder-Frederick, L. A., Carter, W., Clark, W., Bennett-Johnson, S., Rosenbloom, A..
Bradley, C , & Moses, J. (1985). Symptoms and blood glucose levels in diabetics. Journal of the
American Medical Association. 253, 1558-1562.
Clark, N. M., Evans, B.. & Mellins, R. B. (1992). Patient use of peak flow monitoring. American
Review of Respiratory Disease. 145. 722-725.
Dirks, J. F., & Kinsman, R. A. (1981). Clinical prediction of medical rehospitalization: Psychological assessment with the battery of asthma illness behavior. Journal of Personality Assessment,
45. 608-613.
Dirks, J. F., Kinsman, R. A., Jones, F. F., Spector, S. L., Davidson, P. T , & Evans, N. W. (1977).
Panic-fear A personally dimension related to length of hospitalization in respiratory illness.
Journal of Asthma Research. 14, 6 1 - 7 1 .
Dirks, J. F., Schraa, J. C , Bron, E. L., & Kinsman, R. A. (1980). Psychomaintenance in asthma:
Hospitalization rates and financial impact. British Journal of Medical Psychology, 53. 349-354.
Eichenhom, M. S., Beauchamp, R. K., Harper, P. A., & Ward, J. C. (1982). An assessment of three
portable peak flow meters. Chest. 82. 306-309.
Ergood, J. S., Epstein, L. H., Ackerman, M., & Fireman, P. (1985). Perception of expiratory flow
by asthmatics and nonasthmatics during rest and exercise. Health Psychology. 4. 545-554.
Evans, I. R. (1992). Asthma among minority children: A growing problem. Chest. 101, 368S-371S.
Fabrega, A. (1990). The concept of somatization as a cultural and historical product of western
medicine. Psychosomatic Medicine, 52. 653-672.
French, T. M., & Alexander, F. (1941). Psychogenic factors in bronchial asthma (Psychosomatic
Medicine Monograph 4). Washington, DC: National Research Council.
Fritz, G. K., Klein, R. B., & Overholser, i. C. (1990). Accuracy of symptom perception in childh o o d a s t h m a . Journal of Developmental
Behavioral
Pediatrics,
II, 6 9 - 7 2 .
Fritz, G. K., & Overholser, J. C. (1989). Patterns of response to childhood asthma. Psychosomatic
Medicine, 51. 347-355.
Fritz, G. K., Spirito, A., Yeung, A., Klein, R., & Frcedman, E. (1994). A pictorial visual analog
scale for rating severity of childhood asthma episodes. Journal of Asthma. 31, 473-478.
Glasberg, H. M., Bromberg, P. M., Stein, M., & Luparcllo, T. J. (1969). A personality study of
asthmatic patients. Journal of Psychosomatic Research, 13, 197-207.
Gortmaker, S., & Sappenfield, W. (1984). Chronic childhood disorders: Prevalence and impact.
Pediatric Clinics of North America, 31, 3-18.
Gustafsson, P. A., Kjellman, M-I. M., & Cedebald, M. (1986). Family iherapy in treatment of
severe childhood asthma. Journal of Psychosomatic Research. 30. 369-374.
Hergenrather, J. R., & Rabinowitz, M. (1991). Age-related differences in the organization of children's knowledge of illness. Developmental Psychology, 27, 952-959.
172
Fritz et al.
Kikuchi, Y., Okabe. S.. & Tamura. G. (1994). Chemosensitivity and perception of dyspnea
in patients with a history of near fatal asthma. New England Journal of Medicine. 330. 13291334.
Killian, K. J.. Mahutte, C. K.. & Campbell. E. J. M.II980). Resistive-load detection during passive
ventilation. Clinical Science. 59. 493^495.
Killian. K. J.. Mahutte, C. K.. & Campbell. E. J. M. (1981). Magnitude of scaling of externally
added loads to breathing. Journal of Applied Respiratory Disease. 123. 12-15.
Kim. S. P.. Ferrara. A.. & Chess. S. (1980). Temperament of asthmatic children: A preliminary
study. Journal of Pediatrics. 97. 483r486.
Kinsman. R. A.. Dirks. J. F.. & Jones. N. F. (1982). Psychomaintenance of chronic physical illness.
In T. Millon & C. J. Green (Eds.), Handbook of clinical health psychology (pp. 435-465). New
York: Plenum Press.
Klein. R., Fritz, G. K., Yeung. A.. McQuaid. E. L.. & Mansell. A. (in press). Spirometric patterns
in childhood asthma: Peak flow compared to other indices.
Kravis, L. P. (1987). An analysis of Fifteen childhood asthma fatalities. Journal of Allergy and
Clinical Immunology. 80. 467-472.
Kravis. L. P.. & Kolski. G. B. (1985). Unexpected death in childhood asthma: A review of 13 deaths
in ambulatory patients. American Journal of Diseases in Childhood. 139. 558-563.
Liebman, R.. Minuchin. S..& Baker. L. (1974). The use of structural family therapy in the treatment
of intractable asthma. American Journal of Psychiatry, 131. 535-540.
McGrath. P. A. (1987). An assessment of children's pain: A review of behavioral, physiological and
direct scaling techniques. Pain. 31. 147-176.
Mellins, R. B. (1989). Asthma education: a national strategy. American Review of Respiratory
Disease. 140. 577-578.
Miller, B. D., (1987). Depression and asthma: A potentially lethal mixture. Journal of Allergy and
Clinical Immunology. 80. 481-486.
Minuchin. S.. Baker. L.. Rosman, B. L., Liebman, R., Milman. L.. & Todd. T. C. (1975). A
conceptual model of psychosomatic illness in children. Archives of General Psychiatry. 32.
1031-1038.
Mrazek, D. (1988). Asthma: Psychiatric considerations, evaluation and management. In E. Middleton, C. E. Reed. E. F. Ellis, N. F. Adkinson. & J. W. Yuninger (Eds). Allergy principles and
practice (pp. 1176-11%). Washington, DC: C. V. Mosby.
National Institutes of Health National Asthma Education Program (1991). Executive Summary:
Guidelines for the diagnosis and management of asthma. American Journal of Asthma and
Allergy for Pediatricians. 5. 5-56.
Nocon, A. (1991). Social and emotional impact of childhood asthma. Archives of Diseases in
Childhood. 66. 458-460.
Parker, S. R., Mellins, R. B.. & Sogu, D. D. (1989). NHLBI workshop summary: Asthma
education—a national strategy. American Review of Respiratory Disease. 140. 848-853.
Polgar, G., & Romadhat, V. (1971). Pulmonary functioning testing in children: Techniques and
standards. Philadelphia: W. B. Saunders.
Purcell, K., Brady, K., Chai, H., Muser, J., Molk. L.. Gordon. N.. & Means. J. (1969). The effect
on asthma in children of experimental separation from the family. Psychosomatic Medicine. 31.
144-164.
Roy, R.. Thomas, M., & Matas, M. (1984). Chronic pain and depression: A review. Comprehensive
Psychiatry. 25. 96-105.
Rubinfeld, A. R., & Pain, M. C. F. (1976). Perception of asthma. Lancet. I. 882-884.
Sears, M. R., & Rea, H. H. (1987). Patients at risk for dying of asthma: New Zealand experience.
Journal of Allergy and Clinical Immunology. 80, 477-481.
Sears, M. (1988). Fatal asthma: A perspective. Immunology and Allergy Proceedings. 9. 259.
Silverman, B. A., Mayer, D., Sabinsky, R., et al. (1987). Training perception of air flow obstruction
in asthmatics. Annals of Allergy. 59. 350-354.
Sly, P. D., Landau, L. L., & Wcymouth. R. (1985). Home recording of peak flow rates and
perception of asthma. American Journal of Diseases in Children, 139. 479-482.
Sperling, M. (1968). Asthma in children: An evaluation of concepts and therapies. Journal of the
American Academy of Child Psychiatry. 7. 44-58.
Perceptual Accuracy in Childhood Asthma
173
Steiner. H., Higgs, C , & Fritz, G. K. (1987). Defense style and the perception of asthma. Psychosomatic Medicine. 49. 34-44.
Strunk, R. C. (1987). Asthma deaths in childhood: Identification of patients at risk and intervention.
Journal of Allergy and Clinical Immunology. 80. 472-477.
Strunk, R., Mrazek, D., Fuhrmann, G.. & LaBrccque, J. (1985). Physiologic and psychological
characteristics associated with deaths due to asthma in childhood. Journal of the American
Medical Association. 254. 1193-1198.
Tack, M., Altose, M. D., & Chemiack, N. S. (1981). Effect of aging on respiratory sensations
produced by elastic loads. Journal of Applied Physiology: Respiratory Environmental and
Exercise Physiology. 50. 844-850.
Taylor, W. R., & Newacheck. P. W. (1992). Impact of childhood asthma on health. Pediatrics. 90.
657-662.
Tietz, W., Kahlstrom. E., & Cardiff, M. (1975). Relationship of psychopathology to death in
asthmatic adolescents. Journal of Asthma Research. 12. 199-206.
Tinsley, B. J. (1992). Multiple influences on the acquisition and socialization of children's health
attitudes and behavior. An integrative review. Child Development. 63. 1043-1069.
Weiss, K. B., Gergen, P. J., & Crain. E. F. (1992). Inner-city asthma. The epidemiology of an
emerging U.S. public health concern. Chest. 101. 362S-367S.
Weiss, K. B., & Wagener, D. K. (1990). Changing pattern of asthma mortality: Identifying target
populations at risk. Journal of the American Medical Association. 264, 1683-1687
Weitzman, M., Klerman, L. V., Lamb, G., Menary. J. & Alpert, J. J. (1982). School absence: a
problem for the pediatrician. Pediatrics, 69. 739-746.
Weitzman, M., Gortmaker, S. L., Sobol, A. M., & Perrin. J. M. (1992). Recent trends in the
prevalence and seventy of childhood asthma. Journal of the American Medical Association.
268. 2673-2677.
Zach, M. S., & Karner, U. (1989). Sudden death in asthma. Archives of Diseases in Children. 64.
1446-51.
Zechman, F. W., & Wiley, R. L. (1986). Afferent inputs to breathing: Respiratory sensation.. In A. P
Fishman (Ed.), Section J. The respiratory system. Handbook of physiology (Vol. 2) Bethesda,
MD: American Physiological Society.