Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Drug discovery wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Prescription costs wikipedia , lookup
Drug interaction wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Theralizumab wikipedia , lookup
Pharmacognosy wikipedia , lookup
Neuropharmacology wikipedia , lookup
Atypical antipsychotic wikipedia , lookup
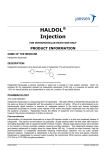
MEDICINE I Adverse Side Effects in Horses Following the Administration of Fluphenazine Decanoate John D. Baird, BVSc, PhD*; and George A. Maylin, DVM, MS, PhD Adverse behavioral side effects may occur in some horses after the intramuscular administration of fluphenazine decanoate. In severe cases, these side effects are difficult to manage and may be life-threatening to the horse, stable personnel, and treating veterinarians. The drug is not approved for use in the horse, and testing for fluphenazine is now conducted by various regulatory organizations involved in racing and equestrian competitions. Authors’ addresses: Department of Clinical Studies, Ontario Veterinary College, University of Guelph, Guelph, ON Canada N1G 2W1 (Baird); and Equine Drug Testing and Research Program, New York Drug Testing and Research Program Morrisville State College, 777 Warren Road, Ithaca, NY 14850 (Maylin); e-mail: jbaird@ovc. uoguelph.ca. *Corresponding author. © 2011 AAEP. 1. Introduction Fluphenazine is a trifluoromethyl phenothiazine derivative (Fig. 1). The systematic International Union of Pure and Applied Chemistry (IUPAC) name of fluphenazine is 2-[4-[3-[2-(trifluoromethyl) phenothiazin-10-yl]propyl]-piperazin-1-yl]ethanol and it has the following structural formula. 2. Clinical Pharmacology Fluphenazine is a highly potent antipsychotic drug that has been used in human medicine in the maintenance treatment of schizophrenia and other forms of psychotic illness since the 1960s.1–3 Long-acting intramuscular depot formulations of fluphenazine, such as fluphenazine decanoate and fluphenazine enanthate, were developed for use in human patients, who cannot be relied on to take oral antipsychotic drugs.1,2,4 The fluphenazine decanoate ester markedly prolongs the duration of action. Fluphenazine decanoate is formulated as a sesame oilbased intramuscular (IM) depot injection and is more commonly used clinically than fluphenazine enanthate. In humans, the most common dosage of fluphenazine decanoate is 25 mg (range, 12.5 to 50 mg), with patients injected once every 2 weeks (range, 1 to 4 weeks).1,5,6 After the IM injection of fluphenazine decanoate, the drug gradually diffuses from the oily vehicle into the surrounding lymph nodes and tissues. Once the drug enters the tissue, it is rapidly hydrolyzed by ubiquitous esterases, and the parent compound (fluphenazine) is released. The hydrolysis of fluphenazine decanoate has been shown to be slow at the IM injection sites, probably because the oil protects the ester from exposure to esterases. Hydrolysis of fluphenazine decanoate has also been shown to occur in a variety of tissues including the lymphatic system and blood.1 Antipsychotic drugs are highly lipophilic, highly membrane-bound or protein-bound, and accumulate in the brain, lung, and other tissues with a high blood supply. It is virtually impossible (and usually not necessary) to remove antipsychotic agents by dialy- NOTES AAEP PROCEEDINGS Ⲑ Vol. 57 Ⲑ 2011 57 MEDICINE I Fig. 1. Chemical structure of fluphenazine. sis.5 Studies in laboratory rats showed that fluphenazine is 10-fold to 27-fold higher in brain regions than is plasma.7 Fluphenazine may also enter the fetal circulation and breast milk.5 After a single injection of fluphenazine decanoate in humans, an early high peak of the drug occurs during the first day and then declines, with a halflife ranging from 6.8 to 9.6 days. After multiple injections of fluphenazine decanoate, however, the mean apparent half-life increases to 14.3 days.8 The individual response to treatment with antipsychotics is highly variable in humans.6,9 Patients must be monitored closely to find a dose that is both safe and effective.6 Humans treated with 25 mg fluphenazine decanoate require 3 months to reach a steady-state plasma level.6 Substantial evidence exists that there is also a sex difference in antipsychotic dosing, in that women require lower doses given at longer intervals.10 Antipsychotic agents are also referred to as neuroleptics and are categorized as either typical (also known as first generation) or atypical (also known as second generation).11 Fluphenazine is classified as a typical antipsychotic, which refers to the fact that when used in clinically effective dosages, they typically induce extrapyramidal side effects (EPS) and symptoms.12 Typical antipsychotics have also been referred to as classic,9 traditional,13,14 or conventional antipsychotics.12,15 The typical antipsychotics are associated with adverse side effects in humans that can affect every system of the body.16 3. Mode of Action The primary site of action for all antipsychotics is the dopamine D2 receptor.17 Dopamine transmission has been found to play an important role in four major pathways: nigrostriatal, mesolimbic, tuberoinfundibular, and mesocortical. The nigrostriatal circuit, originating from A8 and A9 groups of dopamine cells, is well known from the impact of deficiencies. When these deficiencies occur naturally in the substantia nigra, Parkinson disease often develops with concomitant movement disorders, rigidity, and so forth, and when they occur as con58 2011 Ⲑ Vol. 57 Ⲑ AAEP PROCEEDINGS sequence of medications, the symptoms may be labeled as extrapyramidal symptoms.15 Neurolepticinduced movement disorders or EPS are commonly encountered in humans after treatment with the typical antipsychotics.2,12 The signs of EPS include Parkinsonism (i.e., tremor, rigidity), bradykinesia (abnormal slowness of movement), akinesia (difficulty in initiating and maintaining movement), dystonia (i.e., abrupt onset, sometimes bizarre muscular spasms affecting mainly the musculature of the head and neck), and akathisia (inner restlessness, compulsion to move).12,16,18 Typical antipsychotics, such as fluphenazine, have a higher affinity for dopamine D2 receptors than dopamine and as a consequence more frequently elicit Parkinsonism than the newer atypical antipsychotics that bind more loosely to the dopamine D2 receptors.14,17 The incidence of acute EPS associated with antipsychotics varies; however, most medical researchers agree that neuroleptic-induced EPS occurs in 50% to 75% of patients who take typical antipsychotics.12,16 Most typical antipsychotics have a narrow therapeutic index, which means that the separation between the dose that produces efficacy and the one that produces EPS and other adverse effects is narrow.12 Dopamine D2 receptor antagonists, such as fluphenazine, have also been shown to cause hyperprolactinemia.19 Hyperprolactinemia is commonly observed in women administered therapeutic doses of typical antipsychotics resulting in amenorrhea, gynecomastia, galactorrhea, and infertility.15,16,19,20 Studies in humans taking long-term antipsychotic medications have also shown that they are at high risk of developing reduced bone mineral density as a consequence of hyperprolactinemia-induced hypogonadism.19,20 4. Fluphenazine in Horses Long-acting depot preparations of fluphenazine, such as fluphenazine decanoate and fluphenazine enanthate, have been administered off-label to horses for a long-lasting sedative effect21,22 and as an anxiolytic and behavior modifier for horses in training and competition.21–24 It also been used in horses undergoing stall rest after surgery,25 in managing the behavior of young horses,24 and for the treatment of fescue toxicosis in pregnant mares.26 There are also anecdotal reports of its use for agalactia, head-shaking, and shivers. Dowling (2004) stated that “before prescribing any drug for problem behavior in horses, the clinician should have (1) a reasonable diagnosis; (2) an appreciation for the mechanism of action of the drug; (3) a clear understanding of the potential side effects; (4) an understanding of how the drug will specifically alter the problem behavior; and (5) an understanding of the potential for abuse (unethical use).22 MEDICINE I 5. Reports of Adverse Reactions in Horses Extrapyramidal side effects after the intramuscular administration of fluphenazine decanoate, as reported in humans,5 have also been reported in the horse.21,23–25 The doses of fluphenazine decanoate administered to those horses that have shown EPS have ranged from 25 mg25 to 50 mg21,23 to 125 mg.23 Extrapyramidal signs are usually observed between 24 and 36 hours after fluphenazine decanoate administration.21,23,25 A case has been reported in which EPS signs were noticed 14 hours after the intramuscular administration of 37.5 mg of fluphenazine enanthate24; another report described signs that developed 72 hours after the administration of 50 mg fluphenazine decanoate.23 It is surprising that such severe and dramatic EPS occur in horses (body weight, 400 to 450 kg) after the administration of amounts of fluphenazine decanoate that are within the standard dose of 25 to 50 mg administered to adult humans (body weight, approximately 70 kg).1,23,24,27,28 Given this large body weight difference, it would appear that the horse may be very susceptible to adverse side effects of fluphenazine decanoate.23,24 It has been proposed that horses might be more susceptible to fluphenazine-induced EPS because they may have a more extensive extrapyramidal system than that in humans.25 To the author’s knowledge, there are no published studies on the pharmacokinetics of fluphenazine decanoate in the horse. 6. Clinical Signs Horses exhibiting extrapyramidal signs can be extremely dangerous to humans.22–25,29 The violent behavior of these horses presents considerable diagnostic and therapeutic challenges. The clinical signs result from a dopamine-acetylcholine imbalance in the extrapyramidal motor system. The signs of EPS in horses are characterized by episodes of severe depression and somnolence and the adoption of abnormal postures with intervals of extremely frantic, repetitive, compulsive, manic movements.21,24,29,30 They may be reluctant to move forward, and when they do, some have a hypermetric gait.23,24,29 Muscle fasciculation has been noted.23–25 When placed in a stall, they appear agitated and restless and may compulsively circle the stall.21,23–25,29,31 Episodes of repetitive and rhythmic neck flexion and head-tossing may occur.23–25,29 Horses may show a rhythmic side-toside swaying of the head and neck23,25 (Fig. 2). Affected horses adopt abnormal postures and often stand with their forelimbs extended forward and may flex their head and neck ventrally and look backward between their forelimbs.21 Horses affected with EPS may have intermittent episodes of pawing that may become more frantic and violent.21,23–25 These pawing episodes may last for up to 1 to 2 minutes (Fig. 3). Horses have also been reported to strike24,25 and rear.25 Profuse sweating may occur as a result of this abnormal Fig. 2. Horse exhibiting abnormal posture and swinging of head and neck after fluphenazine decanoate administration. behavior.21,23,24 Horses may become laterally recumbent21,25,31 and may paddle while recumbent.25 There are reports of seizures,21 jaw champing,25 and flank biting.23 Abnormal neurological signs have been observed in neonatal foals nursing dams that have been administered fluphenazine decanoate. Fluphenazine has been detected in the dam’s milk and serum of the dam and her foal. 7. Diagnosis Determination of serum or plasma fluphenazine concentrations can only be performed by a small number of equine analytical laboratories in North America and throughout the world. Unfortunately results are usually available after a minimum of 2–3 weeks. This is not of great value when a veterinarian is confronted with a case of a horse exhibiting extrapyramidal signs due to fluphenazine. However, determination of fluphenazine in serum or plasma is the “gold standard” and retrospectively is of value in Fig. 3. Horse exhibiting frantic pawing after fluphenazine decanoate administration. AAEP PROCEEDINGS Ⲑ Vol. 57 Ⲑ 2011 59 MEDICINE I confirming the diagnosis. For most veterinarians, the history of fluphenazine administration within the last 72 hours, as well as clinical signs of restlessness, agitation, bizarre behavior, violent and frantic pawing, and abnormal movements of the head and neck, are supportive of a diagnosis of EPS. There have been wide variations in serum fluphenazine concentrations in horses with EPS.23–25 In severe EPS, fluphenazine concentrations as high as 20.3 ng/mL24 and 39 ng/mL23 have been recorded, but there are also cases with marked signs with values of 3 to 4 ng/mL.23,25 Wide and highly fluctuating variations in serum or plasma fluphenazine concentrations have also been observed in humans.6 Plasma fluphenazine concentrations in the range of 0.25 to 0.80 ng/mL have been considered to be probably adequate for maintenance therapy.6 As a result of the highly lipophilic nature of fluphenazine, the tissue levels may be more important than plasma or serum fluphenazine values. The author is not aware of any studies on tissue levels after fluphenazine decanoate administration to the horse. 8. Differential Diagnoses Differential diagnoses should include any disease producing cerebrocortical dysfunction.28 The primary diagnostic rule-outs for fluphenazine-induced EPS in a horse include rabies, equine herpes virus (EHV)-1 myeloencephalopathy, equine protozoal myeloencephalitis (EPM), Eastern equine encephalitis (EEE), Western equine encephalitis (WEE), West Nile virus (WNV), and fumonisin toxicity (i.e., equine leukoencephalomalacia).23,25,28 Because many of the horses appear restless, agitated, with constant walking and episodes of pawing, colic may also be a diagnostic possibility. In the western United States, nigropallidal encephalomalacia from the chronic ingestion of yellow star thistle (Centaurea solstitialis) or Russian knapweed (Centaurea repens) may also be considered as a possible diagnosis.24,30 However, many of these diseases may not be considered primary rule-outs when the vaccination history and seasonal, environmental, and geographic conditions are taken into account. If the severe signs exhibited by some horses are not recognized as being secondary to antipsychotic administration, it may lead to inappropriate euthanasia.29 9. Treatment Horses with EPS are often refractory to conventional tranquilizers such as xylazine, acepromazine, or romifidine or they may result in a variable and transient effect.23–25,31 An intravenous catheter should be placed whenever possible to allow easy venous access for repeated sedation and fluid administration. The principal treatment of fluphenazine-induced EPS is based on the cholinergic-dopaminergic transmitter model.23–25,32 In the extrapyramidal system, especially in the basal ganglia, acetylcholine is an excitatory transmitter, whereas dopamine is an 60 2011 Ⲑ Vol. 57 Ⲑ AAEP PROCEEDINGS inhibitory transmitter. Under normal conditions, the cholinergic-dopaminergic system maintains physiologic balance, resulting in coordinated neuromuscular activity.32 After the administration of fluphenazine, blockage of the dopamine D2 receptors occurs, especially in the nigrostriatal system. The acetylcholine neurotransmitters become dominant and overactive after the sudden withdrawal of dopaminergic inhibition, leading to an acute extrapyramidal reaction.17 Centrally acting anticholinergic drugs that restore an appropriate dopamine-acetylcholine balance, such as benztropine and diphenhydramine hydrochloride, may be used to treat the extrapyramidal signs. Both drugs have been used in the treatment of fluphenazine-induced EPS in the horse.21,22–25,29,31 Diphenhydramine hydrochloride (0.67 to 1.0 mg/kg IV) administered as a bolus or over 20 minutes is the most widely used drug in the treatment of EPS in the horse.23–25,31 If there is no response, a second dose after an interval of approximately 15 minutes should be given.23,24 If there is still no response, benztropine mesylate (0.018 mg/kg IV q 12 h or 0.04 mg/kg PO q 12 h) should be given.23 Benztropine mesylate is a synthetic compound containing the tropine portion of atropine and the benzohydryl portion of diphenhydramine.32 Theoretically, benztropine mesylate should have stronger antiparkinsonic and anticholinergic effects than diphenhydramine.5,32 Benztropine mesylate has both anticholinergic and antihistaminic effects.32 In horses, it has been recommended that treatment with benztropine mesylate (0.035 mg/kg PO q 12 h) should be continued for 7 to 10 days to prevent a recurrence. In humans, a more rapid response has been observed with antipsychotic-induced dystonic reactions after treatment with benztropine mesylate than with diphenhydramine.13,16,32 In some horses with EPS, neither diphenhydramine hydrochloride23,25 or benztropine mesylate is effective.23 In these refractory cases, supportive hypnotic therapy may be necessary. Intravenous pentobarbital and phenobarbital has been found to be useful in managing the maniacal behavior of these horses.21,23,25,31 The ability to provide longterm sedation and control of fluphenazine-induced central nervous system excitement without inducing recumbency or anesthesia has been shown to be very beneficial in managing these severe cases.21 Intravenous boluses or continuous-rate infusion of sodium pentobarbital (2.6 to 5.5 mg/kg IV) have been given to provide rapid sedation.21,23 In some horses, continuous-rate infusion of phenobarbital after a loading dose of 12 mg/kg administered in 1 L over 20 to 30 minutes21,25 and oral phenobarbital (10.6 mg/kg) has been used to manage these cases.25 While receiving barbiturates, horses with EPS need close monitoring for a period of 5 to 10 days, and, ideally, serum phenobarbital levels should be monitored to maintain the recommended therapeutic MEDICINE I range of 20 to 40 g/mL.25 With improvement of the horse’s mental status and behavior, the administration of phenobarbital may be gradually reduced.23,25 Intravenous chloral hydrate may be used in place of barbiturates.31 Balanced electrolyte solutions, such as lactated Ringer’s solution, should be given IV during hospitalization to provide renal diuresis.21,23,25 Observation of a response to anticholinergic treatments (diphenhydramine, benztropine mesylate) for EPS may place the viral encephalitides lower on the differential diagnostic list. 10. Prognosis The prognosis for the recovery of affected horses tends to be good, and recovery is typically complete.28 The prognosis may depend on the dosage, route of administration, frequency of administration, and interval(s) between doses. Considerable difficulty may be involved in the treatment of these horses. Transportation to a referral hospital is recommended, but that may be difficult and hazardous.23,25 There are reports of horses being euthanized because of the severity of the behavioral abnormalities and the lack of response to conventional tranquilizers and anticholinergics (diphenhydramine, benztropine mesylate).23 There are no reports of the long-term continuation of EPS in the horse, as reported in humans.12,16,25 11. Testing for Fluphenazine In 1997, a highly sensitive and specific high-performance liquid chromatographic method with coulometric detection was developed for the simultaneous assay of fluphenazine and its metabolites in plasma. The lower limit of quantification and detection of fluphenazine and its metabolites in equine plasma is 0.1 ng/mL.1 The United States Equestrian Federation (USEF) classifies fluphenazine as a forbidden substance and warns that it is possible that long-acting forms of fluphenazine or its metabolites may remain detectable in blood for long periods of time. For this reason, a 90-day withdrawal time is recommended to avoid inadvertent positive findings. Detection depends on the formulation of the drug, dose or doses administered, frequency of administration, route of administration, weight of the horse or pony, and health condition of the animal. Fluphenazine testing was instituted by the USEF in 2003, and up until 2010 there have been 48 positive tests in competition horses under the USEF jurisdiction. The penalties imposed for a positive fluphenazine test have ranged from $3000 to $6000 as well as suspension from competing or taking any part whatsoever in recognized competitions as an exhibitor, participant, or spectator for periods of 3 to 6 months. Any trophies, prizes, ribbons, and monies won by these horses must also be returned. From November 1, 2003, the New York Racing and Wagering Board commenced post-race testing for fluphenazine and reserpine. The New York Racing and Wagering Board Rules of Racing that pertain to these drugs for Thoroughbreds is Rule 4043.7 and for Harness horses is Rule 4120.11. These rules state: “(a) Notwithstanding any inconsistent provision of this part, a finding by the laboratory that the drug reserpine or the drug fluphenazine was present in the sample taken from a horse shall result in the disqualification of the horse from the race and from any share of the purse in the race; and (b) The trainer of a horse which has been the subject of a finding by the laboratory that the drug reserpine or the drug fluphenazine was present in the sample taken from that horse shall not be subject to application of trainer’s responsibility based solely upon the finding by the laboratory that the drug reserpine or the drug fluphenazine was present in the sample.” The Fédération Equestre Internationale classifies fluphenazine as a prohibited substance, which means a substance that has been deemed by the Fédération Equestre Internationale to have no common legitimate use in equine medicine and/or have a high potential for abuse. Positive drug tests have been reported. Equine veterinarians who are involved in prepurchase examinations may now request drug screening tests that include detection of fluphenazine. References 1. Luo J-P, Hubbard JW, Midha KK. Sensitive method for the simultaneous measurement of fluphenazine decanoate and fluphenazine in plasma by high-performance liquid chromatography with coulometric detection. J Chromatogr B 1997; 688:303–308. 2. Altamura AC, Sassella F, Santini A, et al. Intramuscular preparations of antipsychotics: uses and relevance in clinical practice. Drugs 2003;63:493–512. 3. Preskorn SH. CNS Drug Development, part I: the early period of CNS drugs. J Psychiatr Pract 2010;16:334 –339. 4. Miller RS, Peterson GM, McLean S, et al. Monitoring plasma levels of fluphenazine during chronic therapy with fluphenazine decanoate. J Clin Pharm Ther 1995;20:55– 62. 5. Baldessarini RJ, Tarazi FI. Drugs and the treatment of psychiatric disorders Psychosis and mania. In: Hardman JG, Limbird LE, ed. Goodman & Gilman’s The Pharmacological Basis of Therapeutics. 10th edition. New York: McGrawHill, 2001:485–520. 6. Marder SR, Aravagiri M, Wirshing WC, et al. Fluphenazine plasma level monitoring for patients receiving fluphenazine decanoate. Schizophrenia Res 2002;53:25–30. 7. Aravagiri M, Marder SR, Yuwiler A, et al. Distribution of fluphenazine and its metabolites in brain regions and other tissues of the rat. Neuropsychopharmacology 1995;13:235– 247. 8. Jann MW, Ereshefsky L, Saklad SR. Clinical pharmacokinetics of the depot antipsychotics. Clin Pharmacokinet 1985;10:315–333. 9. Farde L, Wiesel F-A, Halldin C, et al. Central D2-dopamine receptor occupancy in schizophrenic patients treated with antipsychotic drugs. Arch Gen Psychiatry 1988;45:71–76. 10. Seeman MV. Gender differences in the prescribing of antipsychotic drugs. Am J Psychiatry 2004;161:1324 –1333. 11. Leucht S, Corves C, Arbter D, et al. Second-generation versus first-generation antipsychotic drugs for schizophrenia: a meta-analysis. Lancet 2009;373:37– 41. AAEP PROCEEDINGS Ⲑ Vol. 57 Ⲑ 2011 61 MEDICINE I 12. Collaborative Working Group on Clinical Trial Evaluations. Assessment of EPS and tardive dyskinesia in clinical trials. J Clin Psychiatry 1998;59(Suppl 12):23–27. 13. Cortese L, Pourcher-Bouchard E, Williams R. Assessment and management of antipsychotic-induced adverse events. Can J Psychiatry 1998;43(Suppl 1):15S–20S. 14. Seeman P. Atypical antipsychotics: mechanism of action. Can J Psychiatry 2002;47:29 – 40. 15. Goodnick PJ, Rodriguez L, Santana O. Antipsychotics: impact on prolactin levels. Expert Opin Pharmacother 2002; 3:1381–1391. 16. Arana GW. An overview of side effects caused by typical antipsychotics. J Clin Psychiatry 2000;61(Suppl 8):5–11. 17. Seeman P. Dopamine D2 receptors as treatment targets in schizophrenia. Clin Schizophr Relat Psychoses 2010;4:56 –73. 18. Carpenter WT Jr, Buchanan RW, Kirkpatrick B, et al. Comparative effectiveness of fluphenazine decanoate injections every 2 weeks versus every 6 weeks. Am J Psychiatry 1999; 156:412– 418. 19. Haddad PM, Wieck A. Antipsychotic-induced hyperprolactinaemia: mechanisms, clinical features and management. Drugs 2004;64:2291–2314. 20. Meaney AM, Smith S, Howes OD, et al. Effects of long-term prolactin-raising antipsychotic medication on bone mineral density in patients with schizophrenia. Br J Psychiatry 2004;184:503–508. 21. Kauffman VG, Soma L, Divers TJ, et al. Extrapyramidal side effects caused by fluphenazine decanoate in a horse. J Am Vet Med Assoc 1989;195:1128 –1130. 22. Dowling PM. Drugs acting on the neurological system and behavior modification. In: Bertone JJ, Horspool LJI, eds. 62 2011 Ⲑ Vol. 57 Ⲑ AAEP PROCEEDINGS 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. Equine Clinical Pharmacology. Edinburgh: Saunders, 2004: 145–154. Baird JD, Arroyo LG, Vengust M, et al. Adverse extrapyramidal effects in four horses given fluphenazine decanoate. J Am Vet Med Assoc 2006;229:104 –110. Brewer BD, Hines MT, Stewart JT, et al. Fluphenazine induced parkinson-like syndrome in a horse. Equine Vet J 1990;22:136 –137. Brashier M. Fluphenazine-induced extrapyramidal side effects in a horse. Vet Clin North Am Equine Pract 2006;22: e37– e45. Bennett-Wimbush K, Loch WE. A preliminary study of the efficacy of fluphenazine as a treatment for fescue toxicosis in gravid pony mares. J Equine Vet Sci 1998;18:169 –174. Adams CE, Fenton MKP, Quraishi S, et al. Systematic meta-review of depot antipsychotic drugs for people with schizophrenia. Br J Psychiatry 2001;179:290 –299. Brashier M. Fluphenazine toxicosis. In: Robinson NE, Sprayberry KA, eds. Current Therapy in Equine Medicine. 6th edition. St. Louis: Saunders Elsevier, 2009:19 –20. Vivrette S. Drugs acting on the reproductive system. In: Bertone JJ, Horspool LJI, eds. Equine Clinical Pharmacology. Edinburgh: Saunders, 2004:177–191. Mayhew IGJ. Toxic diseases. In: Mayhew IGJ, ed. Large Animal Neurology. 2nd edition. Ames: Wiley-Blackwell, 2009:321–359. Divers TJ. Specific acute drug reactions and recommended treatments. In: Orsini JA, Divers TJ, eds. Equine Emergencies: Treatment and Procedures. 3rd edition. St. Louis: Saunders Elsevier, 787–794. Lee A-S. Treatment of drug-induced dystonic reactions. JACEP 1979;8:453– 457.