Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
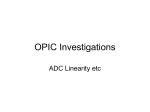
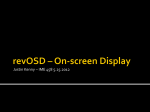
CME JOURNAL OF MAGNETIC RESONANCE IMAGING 000:000–000 (2012) Original Research Comparison of MRS and DWI in the Diagnosis of Prostate Cancer Based on Sextant Analysis Bo Li, MS,1 Wenchao Cai, BS,2 Dongjiao Lv, PhD,1 Xuemei Guo, PhD,2 Xiaoying Wang, PhD,2,3* Jue Zhang, PhD,1,3* and Jing Fang, PhD1,3 PROSTATE CANCER IS the fifth most common cancer in the world and the second most common in men (1). Numerous studies indicated approximately 65%–75% prostate cancer cases occur in the peripheral zone (2). Magnetic resonance (MR) imaging as a noninvasive tool plays an increasingly important role in the detection, localization and staging of prostate cancer (3). T2-weighted endorectal MR image can depict the prostate zonal anatomy and periprostatic structures with exquisite detail (4). MR spectroscopic (MRS) imaging has ability to provide chemical information about metabolites in normal and abnormal tissues. Elevation of choline (Cho) levels and reduction of citrate (Cit) have been observed in cancerous tissue relative to normal prostatic tissue (5). Diffusion-weighted imaging (DWI) can offer valuable information about the microstructure and pathophysiology of tissues based on the diffusion properties of the water molecules. Results of several studies suggested the apparent diffusion coefficient (ADC) values of cancerous peripheral zone (PZ) and transition zone tissues was lower than those of normal prostate tissue (6). Although both MRS and DWI can provide valuable information about prostate cancer (PCa), each of them plays a different role in detection. Kumar et al (7) studied both MRS and DWI and observed a positive correlation between metabolic ratio (Cit/(Cho þ Cr)) and ADC with estimated prostate-specific antigen (PSA). It was reported that the combination of MRS and DWI improved the detection of malignancy. Reinsberg et al (8) reported that specificity of the combination of DWI (ADC) and MRS (Cho/Cit) was significantly improved compared with DWI or MRS alone, without reduction in sensitivity for voxels containing 70% or more tumor tissue. Both studies used voxel-wise comparisons. In contrast, Mazaheri et al (5) used a region of interest (ROI)-based analysis and combined DWI and MRS with generalized estimating equations using a logistic regression model and reported that the combination of DWI and MRS was significantly more accurate than MRS alone and was also more accurate than DWI alone, although the latter difference was not significant. However, the results in these studies depend highly on the data registration between DWI and MRS; besides, there is no comparison of the utility of MRS and DWI in cancer diagnosis in the related studies. Purpose: To evaluate apparent diffusion coefficient (ADC) value, metabolic ratio ((Cho þ Cr)/Cit) and the combination of the two in identifying prostate malignant regions. Materials and Methods: Fifty-six consecutive patients with prostate biopsy results were retrospectively recruited in this study. Transrectal ultrasound-guided (TRUS) systemic prostate biopsies were used as a standard of reference. Mean ADC value and mean metabolic ratio (MMR) were calculated within each benign sextant region or malignant region. The efficiency of these two indices in prostate cancer (PCa) diagnosis is estimated in Fisher linear discriminant analysis (FLDA). The area under the receiver operating characteristic (ROC) curve was used to evaluate the distinguishing capacity of mean ADC, MMR, and the combination of the two in differentiating between noncancerous and cancerous cases. Results: There were significant differences for mean ADC value and MMR between malignant and benign regions. Weights of mean ADC value obtained by FLDA were much higher than those of MMR. In differentiating malignant regions, both ADC alone and combined ADC and metabolic ratio performed significantly better than MMR alone. However, accuracy improvements were not significant by using combined ADC and MMR than ADC alone. Conclusion: DWI is more efficient than MR spectroscopic (MRS) in the detection of PCa in this study. Combined ADC and MMR performed significantly better than MMR alone in distinguishing malignant from benign region in prostate peripheral zone. Key Words: prostate cancer; MR spectroscopic imaging; Diffusion weighted imaging; fisher linear discriminant analysis J. Magn. Reson. Imaging 2012;000:000–000. C 2012 Wiley Periodicals, Inc. V 1 College of Engineering, Peking University, Beijing, China, People’s Republic of China. 2 Department of Radiology, Peking University First Hospital, Beijing, China, People’s Republic of China. 3 Academy for Advanced Interdisciplinary Studies, Peking University, Beijing, China, People’s Republic of China. Contract grant sponsor: Fundamental Research Funds for the Central Universities. *Address reprint requests to: Jue Zhang, College of Engineering, Peking University, Yiheyuan Road No. 5, Beijing, 100871, China. E-mail: [email protected]; Xiaoying Wang, Department of Radiology, Peking University First Hospital, Xishiku Street No. 8, Xicheng District, Beijing, 100034, China. E-mail: [email protected] Received January 15, 2012; Accepted August 8, 2012. DOI 10.1002/jmri.23809 View this article online at wileyonlinelibrary.com. C 2012 Wiley Periodicals, Inc. V 1 2 In this study, we aim to (a) compare the utility of mean ADC and mean metabolic ratio ((Cho þ Cr)/Cit) by analyzing the weights of them in the detection of PCa using Fisher linear discriminant analysis (FLDA), and then (b) evaluate ADC value, metabolic ratio ((Cho þ Cr)/Cit) and the combination of the two by FLDA in identifying malignant regions. MATERIALS AND METHODS Database After institutional review board approval and written informed consent, fifty-six consecutive patients were retrospectively evaluated in this study from 2007– 2009. Inclusion criteria are: (a) The image data and clinical record of the patient were available; (b) Transrectal ultrasound-guided biopsy was performed within 6 months of MR examination, with pathological record of the cancerous and noncancerous areas in the prostate gland; (c) The patients had not received any treatments such as endocrine therapy, brachytherapy, radiotherapy, etc., before MRI. The Gleason score varied from 6 to 10 and 30 patients (54%) had a Gleason score of 7 or lower. The 23 patients (41%) (mean age, 66.2 6 9.3 years; range, 54–78 years) with benign prostate were all histopathologically confirmed. The histological diagnosis on the basis of tissue obtained by transrectal ultrasound-guided sextant biopsy was benign prostatic hyperplasia with or without chronic prostatitis or no histological abnormality, but no evidence of prostatic intraepithelial neoplasia. The serum PSA level ranged from 0.61 to 29.63 ng/mL with a mean value of 9.9 ng/mL. All 33 PCa patients (59%) (mean age, 68.2 6 9.8 years; range, 56–79 years) were also histopathologically diagnosed by ultrasound-guided sextant prostate biopsy. The serum PSA level ranged from 4.15 to 38.00 ng/mL with a mean value of 13.99 ng/mL. MR Imaging Thin-section, high-spatial-resolution transverse T2-WI MR images of the prostate and seminal vesicles were obtained on a 1.5 Tesla (T) whole-body MR scanner (SignaTM; GE Medical Systems, Milwaukee, WI). The patients were examined in supine position using a body coil for excitation and a pelvic phased-array coil (GE Medical Systems) for signal reception in combination with an expandable endorectal coil (Medrad, Pittsburgh, PA). A fast spin-echo sequence was applied with the following parameters: repetition time/echo time of 3800/139 ms; echo train length, 12–16; section thickness, 3 mm; intersection gap, 0 mm; field of view, 26 cm; matrix, 320 256; and four signal averages were acquired. Li et al. troscopy (PRESS) sequence, with high-bandwidth spectral-spatial 180 refocusing pulses, and with very selective outer voxel suppression pulses (9). A PRESS volume encompassing the prostate was graphically selected using the T2-weighted transverse images. This volume was selected to maximize coverage of prostate while minimizing the inclusion of periprostatic fat and rectal air. Dual-band spectral-spatial radiofrequency 180 pulses (10) and highly selective outer voxel saturation pulses (11) were combined to achieve water and lipid suppression. Additional voxel saturation bands were selectively placed around the selected region of interest to confine the shape of the rectangular PRESS volume to the shape of the prostate. Three-dimensional MR spectroscopic imaging data were acquired from the prostate with the following parameters: repetition time / echo time 1000/130 ms, field of view 11 cm and 16 8 8 phase encoding to yield spectra with a nominal resolution of 345 mm3 in approximately 17 min. The total MR acquisition time was typically approximately 50 min. All 3D MR spectroscopy data were transferred offline and processed on a workstation (Functool, GE Medical Systems) using specific commercially available software developed for 3D MR spectroscopy studies. The 3D MR spectroscopy data sets were apodized with a 2-Hz Lorentzian function, Fourier transformed in the time domain and three spatial domains. After frequency, phase, and baseline correction, the integral areas for the choline, creatine, and citrate resonances were calculated. Diffusion-Weighted Imaging Diffusion-weighted imaging (DWI) data were acquired by using single-shot diffusion-weighted echo-planar imaging with repetition time (TR) of 3500 ms, echo time (TE) of 56.7 [b ¼ 500 s/mm2, b ¼ 0 s/mm2] or 76.7 [b ¼ 800 s/mm2, b ¼ 0 s/mm2] ms, field of view 26 26 cm, matrix size 128 128, section thickness 6 mm, no intersection gap and four signal averages. Fisher Linear Discriminant Analysis (FLDA) FLDA was used to evaluate the weights of mean ADC value and mean metabolic ratio ((Cho þ Cre)/Cit) in the detection of prostate cancer. FLDA is a linear discriminative method to analyze the efficiency of each feature vector in a certain task by their weights in the discriminant. The weights reflect the utility of these two features in prostate cancer diagnosis. Given two classes with mean vectors M1, and M2, the goal of FLDA is to find the linear projection, x, which maximizes the contrast criterion J(x), the ratio of inter-cluster distance to intra-cluster variance represented as: J ðxÞ ¼ ðx 0 Sb xÞ=ðx 0 Sw xÞ Three-Dimensional 1H MR Spectroscopic Imaging Three-dimensional (3D) MR spectroscopic imaging was performed using the prostate spectroscopy and imaging examination (PROSE) sequence (GE Medical Systems), which is a water- and lipid-suppressed double-spin-echo point-resolved spatially localized spec- ½1 where Sw ¼ 2 X X k¼1 x2Ck ðx Mk Þðx Mk Þ0 ½2 MRS and DWI in the Diagnosis of Prostate Cancer 3 Figure 1. Box-and-whisker plots of mean ADC (b ¼ 500 s/mm2) (a), mean ADC (b ¼ 800 s/mm2) (b), and mean (Choline þ Creatine)/Citrate (c) in prostate cancer and benign prostate peripheral zone regions. and Sb ¼ ðM1 M2 ÞðM1 M2 Þ0 ½3 are intra-cluster variance and inter-cluster distance, respectively. When 1 x ¼ Sw ðM1 M2 Þ ½4 is satisfied, J(x) is maximized. Next, a new feature is obtained by combining individual features with the direction vector x: * D ¼ xT F ; ½5 * where F are feature vectors. Data Analysis The first criterion chosen for inclusion of an MRS voxel was that the signal-to-noise ratio (SNR) of the three main metabolites (Cho, Cit, and Cr) in each spectrum was greater than 3. The second criterion was that there was no lipid peak at 2.0 ppm influencing Cit peak. The third criterion was that at least 70% of the voxel was covered by peripheral zone. Tumor regions were defined as low-signal-intensity areas within peripheral zone in a sextant that was biopsy-positive on T2-weighted images and identified by a radiologist who had more than 5 years experience in interpreting prostate MRI. On the contrary, benign regions were defined as normal signal intensity areas within peripheral zone in a sextant that was biopsynegative on T2-weighted images. The identified regions on T2-weighted images were mapped on the MRS imaging grid and ADC map for voxel and region selection. For MRS, tumor region consisted of all voxels whose 60% were covered by tumor tissue on the basis of comparison of the grid with T2-weighted images within a sextant region. Corresponding regions were selected from ADC maps on the basis of T2weighted (b ¼ 0) images to minimize the partial volume effect, because of the one to one correspondence of the ADC voxels to the voxels of the T2-weighted images. Sextant regions containing tumor foci that were 0.1 cm3 or smaller or more than 50% invalid voxels were excluded to avoid the bias resulted from partial volume. The corresponding sextant regions in DWI were eliminated at the same time. Two hundred twentyeight (67%) sextant regions were involved in the analysis. Mean ADC value and mean metabolic ratio for malignant regions and benign sextant regions were calculated. Statistical Analysis T-tests were performed to evaluate the differences between groups of benign and malignant regions characterized by mean ADC, mean metabolic ratio ((Cho þ Cre)/Cit) and the combination of the two. Classification performance was evaluated by receiver operating characteristic (ROC) (12,13) analysis based on biopsy results. The area under the ROC curve (Az) was used as an index to evaluate the inherent distinguishing capacity of mean ADC, mean metabolic ratio, and the combination of the two in differentiating between noncancerous and cancerous cases. A 4 Li et al. Figure 2. A 72-year-old man with a current PSA level of 27.5 mg/mL and biopsy-proved cancer (Gleason score of 5 þ 4) in the right peripheral zone. a: The selected volume for spectroscopy (white box) is overlaid on the transverse T2-weighted (3800/139) image. And two areas in the volume are chosen for both comparisons of ADC and metabolic ratio. An area locates in the cancer right peripheral zone (1) and another one locates in the normal left peripheral zone (2). b: ADC color map obtained using b value of 800. ADC value in the cancer right peripheral zone (0.96 103 mm2/s) is lower than that in benign tissue in the left peripheral zone (1.73 103 mm2/s). c: MR spectrums obtained from the cancer right peripheral area (1 in a) shows elevated choline and reduced citrate, and its metabolic ratio ((Cho þ Cr)/Cit) is 4.14. d: MR spectrums obtained from the normal left peripheral zone (2 in a) shows a normal spectral pattern with high citrate and the absence of an elevated choline, and its metabolic ratio ((Cho þ Cr)/Cit) is 0.686. P value less than 0.05 was selected as the criterion of statistical significance. RESULTS In our study, according to the MRS inclusion criteria, we obtained 336 sextant regions and 1305 voxels. Among those voxels, (a) Eighty-seven voxels were excluded because they had a low SNR for all the three main metabolites (Cho, Cit, and Cr); (b) Two hundred fifty-three voxels were excluded because there were large lipid peaks interfered the interpretation of Cit peak; (c) Another 135 voxels were excluded because they contained too much urethra and periprostatic fatty tissue. Totally 475 voxels were nondiagnostic, then 830 voxels and 247 sextant regions were available for further analysis. Furthermore, 19 tumor sextant regions were excluded for data analysis because no voxels locating in those tumor region contained more than 60% tumor tissue. Finally, there were 228 sextant regions (146 benign and 82 malignant) included in the study. The median number of benign regions per patient was four (range, zero to six), and the median number of malignant regions per patient was four (range, zero to six). The mean ADC values with b values of 500 and 800 s/mm2 and mean (Cho þ Cre)/Cit are shown in Figure 1. The ADC values when b ¼ 800 were significantly different from those when b ¼ 500 for malignant regions and benign sextant regions (P ¼ 0.0028). Figure 2 shows a sample MR images with the corresponding 3D MRS imaging results and ADC maps obtained using b ¼ 800. The weights of mean ADC and mean metabolic ratio ((Cho þ Cre)/Cit) in the detection of prostate cancer MRS and DWI in the Diagnosis of Prostate Cancer 5 Table 1 FLDA Weights for Combining Diffusion-Weighted With Different b Values and MR Spectroscopic Imaging Measurements FLDA weight 2 b ¼ 500 (s/mm ) Mean ADC value Mean (ChoþCre)/Cit b ¼ 800 (s/mm2) Mean ADC value Mean (ChoþCre)/Cit 0.9388 0.0612 0.9374 0.0626 with different b values are shown in Table 1. The mean ADC value with b values of 500 s/mm2 for all patients for malignant regions in the PZ (mean 6 standard deviation (SD): 1.1441 6 0.4136 (103 mm2/s)) was significantly lower than that for benign regions in the PZ (1.8213 6 0.3365 (103 mm2/s)) (P < 0.001) (Table 2). Similarly, the mean ADC value with b values of 800s/mm2 for all patients for malignant regions in the PZ (1.0603 6 0.1362 (103 mm2/s)) was significantly lower than that for benign regions in the PZ (1.7053 6 0.3225 (103 mm2/s)) (P < 0.001) (Table 2). The mean (Cho þ Cre)/Cit ratios for all patients for malignant regions in the PZ (2.7062 6 2.1746) was significantly higher than that for benign regions in the PZ (1.1197 6 0.8146) (P < 0.01) (Table 2). Performance in differentiating malignant from benign regions in the PZ was evaluated by ROC analysis (Fig. 3). Mean metabolite ratio alone yielded an Az value of 0.778 (Table 3). No cutoff value of metabolite ratio could be chosen to achieve 70% for both sensitivity and specificity. A cutoff value of 0.81 resulted in a sensitivity of 56.1% and specificity of 88.4% (Table 4). In the case of b ¼ 500 s/mm2, mean ADC alone yielded an Az value of 0.892 (Table 3) and using a cutoff value of 1.49 103 mm2/s, cancer was detected with a sensitivity of 85.4% and specificity of 87% (Table 4). Mean ADC alone performed significantly more accurately than mean metabolite ratio alone (P < 0.01). The combination of metabolite ratio and ADC yielding an Az value of 0.895 was also more accurate than metabolite alone (P < 0.001), but there was no significant improvement compared with mean ADC alone (Fig. 3a). When b ¼ 800 s/mm2, mean ADC alone yielded an Az value of 0.897 (Table 3) and using a cutoff value of 1.26 103 mm2/s, cancer was detected with a sensitivity of 81.7% and specificity of 93.2% (Table 4). Mean ADC alone was significantly more accurate than mean metabolite ratio alone (P < 0.01). The combination of metabolite ratio and ADC yielded an Az value of 0.901, achieving significantly better discrimination of malignant from benign regions than metabolite alone (P<0.001) and was also slightly better than ADC alone, but the latter difference was not significant (Fig. 3b). In both cases, the sensitivity of the combination was significantly improved compared with metabolite ratio alone (P < 0.001) (Table 4). There was a slight improvement in specificity when b ¼ 800 s/mm2 (Table 4). DISCUSSION In this study, mean ADC with different b values and mean metabolic ratio ((Cho þ Cr)/Cit) for benign sextant regions and malignant regions within sextant regions were retrospectively calculated. Mean ADC values were lower and mean metabolic ratios ((Cho þ Cre)/Cit) were higher for malignant than for benign PZ regions. These changes were consistent with those reported in previous studies (5,7,8,14). All the patients in our study underwent the same MR protocol. Multi b values of 500 and 800 s/mm2, which are common selections in our usual scanning, were used to investigate whether diagnosis performance changes with different b-value. Although significant difference was found between ADC values from b ¼ 800 and b ¼ 500 for both malignant regions and benign sextant regions, there is no significant difference in either weight analysis or diagnosis performance between ADC values of two groups. Kitajima et al (15) reported that measuring ADC using a high b-value has little diagnostic advantage over using the standard b-value in discriminating malignant from normal prostate tissue. The clinical benefit of high-b-value DWI has also been discussed, although sacrificing the signal-to-noise ratio (16). Therefore, extending the analysis to include more and higher b values could better assess the effect of b-value in diagnosis and provide better MR protocol of DWI. FLDA is a linear discriminative method to analyze the efficiency of each feature vector in a certain task by their weights in the discriminant. There is a positive relation between weight and utility. The weights ranges from 0 to 1, larger weight suggesting more important role the corresponding feature plays in the task. A weight of 1 indicates that the corresponding feature is absolutely primary; on the contrary, a weight of 0 indicates a neglectable feature. To our knowledge, ours is the first study to use FLDA to analysis the weights of MRS and DWI in prostate cancer diagnosis. Mean ADC weights obtained by FLDA (0.9388 (b ¼ 500 s/mm2) and 0.9374(b ¼ 800 s/ mm2)) are much higher than those of mean metabolic ratios (0.0612 (b ¼ 500 s/mm2) and 0.0626 (b ¼ 800 s/mm2)), indicating that DWI is more efficient than MRS in the detection of PCa in the current study. More efficient functional MRI techniques are superior in prostate cancer screening and diagnosis and scan program could be optimized by the weights obtained by FLDA based on a larger patient population. Table 2 Statistical Results of ADC and Metabolite Ratio Measurement* 3 ADC (10 mm /s) b ¼ 500 (s/mm2) b ¼ 800 (s/mm2) (ChoþCre)/Cit Cancer region Benign region 1.144160.4136 (0.157–2.25) 1.060360.1362 (0.368–2.28) 2.706262.1746 (0.475–7.998) 1.821360.3365 (0.92–2.57) 1.705360.3225 (0.833–2.7) 1.119760.8146 (0.2010–4.385) 2 *Data are mean 6 SD (range). 6 Li et al. Figure 3. Receiver operating characteristic curves show performance of mean ADC alone, mean [(Choline þ Creatine)/Citrate] alone, and combination of the two to differentiate between cancer and benign regions in the case of (a) b ¼ 500 s/mm2 and (b) b ¼ 800 s/mm2. In our study, combined ADC and metabolic ratio ((Cho þ Cr)/Cit) by FLDA was evaluated in identifying malignant regions with sextant biopsy findings, as well as mean ADC alone and mean metabolic ratio ((Cho þ Cr)/Cit) alone. To avoid the registration problem between different scan techniques and better correspond to biopsy findings, the ADC values and metabolic ratios of all malignant voxels within a sextant region were averaged as new indicators. This is different from previous studies (5,8) where a voxel to voxel correspondence of tumor regions on ADC maps and MRS maps is needed, whereas the voxels on ADC maps cannot correspond exactly to the voxels on the MRS maps because of the discrepancy in voxel size and scan protocol. Combined ADC and metabolic ratio performed better than metabolic ratio and ADC alone. This result was consistent with previous results (5,8). However, accuracy improvements were not significant by using combined ADC and metabolic ratio than ADC alone. And ADC alone performed better than metabolic ratio alone for both b values. These results were consistent with (5), but contrary to the results of (8) that reported that MRS alone performed better than DWI alone. The deficiency of MRS in weight analysis and ROC analysis was presumably attributed to susceptible signal by lipid contamination and low spatial resolution. The spatial resolution of MRS is nearly tenfold lower than that of DWI. Additionally, MRS took much longer Table 3 Area Under Curve (Az) of Metabolite Ratio Alone, ADC Alone, and Combination of the Two in ROC Analysis b ¼ 500 (s/mm2) b ¼ 800 (s/mm2) Measurement Az* Az* (ChoþCre)/Cit ADC Combineda 0.77860.032 (0.715–0.841) 0.89260.025 (0.844–0.941) 0.89560.024 (0.848–0.942) 0.77860.032 (0.715–0.841) 0.89760.025 (0.849–0.945) 0.90160.024 (0.854–0.948) *Data are mean 6 SD (95% confidence interval). a For b ¼ 500 (s/mm2), combined ¼ 0.9388ADC-0.0612(ChoþCre)/Cit; For b ¼ 800 (s/mm2), combined ¼ 0.9374ADC0.0626(ChoþCre)/Cit. Table 4 Sensitivities, Specificities and Accuracies of Metabolite Ratio Alone, ADC Alone, and Combination of the Two as Predictors of Prostate Cancer b ¼ 500 (s/mm2) Criterion for positive (cancer)* (ChoþCre)/Cit ADC Combined b ¼ 800 (s/mm2) Sensitivity (%) Specificity (%) Accuracy (%) Sensitivity (%) Specificity (%) Accuracy (%) 56.1 85.4 86.6 88.4 87.0 83.6 76.8 86.4 84.7 56.1 81.7 82.9 88.4 93.2 89.7 76.8 88.7 87.2 *Optimum cutoff values for b ¼ 500 (s/mm2): (ChoþCre)/Cit ¼ 0.81. ADC ¼ 1.34 103 mm2/s, combined ¼ 0.9388 ADC 0.0612 (ChoþCre)/Cit. Optimum cutoff values for b ¼ 800 (s/mm2): (ChoþCre)/Cit ¼ 1.96, ADC ¼ 1.26 103 mm2/s, combined ¼ 0.9374 ADC 0.0626 (ChoþCre)/Cit. MRS and DWI in the Diagnosis of Prostate Cancer time when imaging which is MRS’s another limitation. However, many studies have reported advantages of MRS including sensitivity to prostate cancer and correlation with Gleason score (17). Moreover, the disadvantage of low spatial resolution would be improved by increasing field strength and using more efficient acquisition sequences (7). Thus, the accuracy of combined DWI and MRS with better spatial resolution should be much improved and higher than that of each technique alone in cancer identification. Tumor regions were defined as low-signal-intensity areas within peripheral zone in a sextant that was biopsy-positive on T2-weighted images, as described in Reinsberg et al (8), and identified by experienced radiologist. As a result, malignant regions isointense to normal peripheral zone tissue on T2-weighted images were not included and there is also a false-positive rate of mimic cancer associated with other benign abnormalities also presenting low signal intensity on T2weighted images. It is not possible to identify those regions in the analysis without histologic proof of their inclusion and exclusion with tumor. Although using whole-mount histopathologic examination can improve the accuracy of the registration between MR images and histopathology (5), the availability of detailed histological comparison at radical prostatectomy has highly limited studies. Moreover, sextant analysis plays an important role not only in diagnostic purpose, but also in determining the prognosis, particularly before radical prostatectomy (18,19). Thus, despite of the defects of biopsy, the findings of our study still processed significance and merit in clinic practice. However, patients might harbor cancer that escaped one-time biopsy detection for prostate cancer heterogeneity, and the evaluation of the Gleason concordance between biopsy and prostatectomy specimens has demonstrated mixed results (20–24). Because most of the patients were suggested hormone therapy, there is no available whole-mount histopathology of the patients in the current study. Therefore, prostatectomy specimens and clinical follow-up are still needed as the reference standard to further confirm the accuracy of the current study. In addition, there is a huge overlap between normal and malignant tissues detections for both ADC and MRS. Therefore, more functional MR imaging techniques will be incorporated into our future research for better performance in discriminating between cancer and benign regions. In conclusion, DWI is more efficient than MRS in the diagnosis of prostate cancer; combined mean ADC value and mean metabolic ratio by FLDA provides a new and useful index as an indicator of prostate cancer and the combination of DWI and MRS is promising in the detection of prostate cancer. ACKNOWLEDGMENT This work was supported by the Fundamental Research Funds for the Central Universities. REFERENCES 1. Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA-Cancer J Clin 2005;55:74–108. 7 2. Stamey TA, Donaldson AN, Yemoto CE, McNeal JE, Sozen S, Gill H. Histological and clinical findings in 896 consecutive prostates treated only with radical retropubic prostatectomy: epidemiologic significance of annual changes. J Urol 1998;160:2412–2417. 3. Wang L, Mullerad M, Chen HN, et al. Prostate cancer: incremental value of endorectal MR imaging findings for prediction of extracapsular extension. Radiology 2004;232:133–139. 4. Heijmink SWTPJ, Futterer JJ, Hambrock T, et al. Prostate cancer: body-array versus endorectal coil MR imaging at 3T-comparison of image quality, localization and staging performance. Radiology 2007;244:184–195. 5. Mazaheri Y, Shukla-Dave A, Hricak H, et al. Prostate cancer: identification with combined diffusion-weighted MR imaging and 3D (HMR)-H-1 spectroscopic imaging correlation with pathologic findings. Radiology 2008;246:480–488. 6. Desouza NM, Riches SF, Vanas NJ, et al. Diffusion-weighted magnetic resonance imaging: a potential non-invasive marker of tumor aggressiveness in localized prostate cancer. Clin Radiol 2008;63:774–782. 7. Kumar V, Jagannathan NR, Kumar R, et al. Correlation between metabolite ratios and ADC values of prostate in men with increased PSA level. Magn Reson Imaging 2006;24:541–548. 8. Reinsberg SA, Payne GS, Riches SF, et al. Combined use of diffusion-weighted MRI and 1H MR spectroscopy to increase accuracy in prostate cancer detection. AJR Am J Roentgenol 2007;188:91–98. 9. Kurhanewicz J, Swanson MG, Nelson SJ, Vigneron DB. Combined magnetic resonance imaging and spectroscopic imaging approach to molecular imaging of prostate cancer. J Magn Reson Imaging 2002;16:451–463. 10. Star-Lack J, Nelson SJ, Kurhanewicz J, Huang LR, Vigneron DB. Improved water and lipid suppression or 3D PRESS CSI using RF band selective inversion with gradient dephasing (BASING). Magn Reson Med 1997;38:311–321. 11. Tran TK, Vigneron DB, Sailasuta N, et al. Very selective suppression pulses for clinical MRSI studies of brain and prostate cancer. Magn Reson Med 2000;43:23–33. 12. Metz CE. ROC methodology in radiologic imaging. Invest Radiol 1986;21:720–733. 13. Metz CE. Some practical issues of experimental design and data analysis in radiological ROC studies. Invest Radiol 1989;24:234–245. 14. Hahn P, Smith IC, Leboldus L, Littman C, Somorjai RL, Bezabeh T. The classification of benign and malignant human prostate tissue by multivariate analysis of 1H magnetic resonance spectra. Cancer Res 1997;57:3398–3401. 15. Kitajima K, Kaji Y, Kuroda K, Sugimura K. High b-value diffusion-weighted imaging in normal and malignant peripheral zone tissue of the prostate: effect of signal-to-noise ratio. Magn Reson Med Sci 2008;7:93–99. 16. Toyoda K, Kitai S, Ida M, Suga S, Aoyagi Y, Fukuda K. Usefulness of high-b-value diffusion-weighted imaging in acute cerebral infarction. Eru Radiol 2007;17:1212–1220. 17. Zakian KL, Eberhardt S, Hricak H, et al. Transition zone prostate cancer: metabolic characteristics at proton MR spectroscopic Imaging-initial results. Radiology 2003;229:241–247. 18. Salomon G, Kollerman J, Thederan I, et al. Evaluation of prostate cancer detection with ultrasound real-time elastography: a comparison with step section pathological analysis after radical prostatectomy. Eur Urol 2008;54:1354–1362. 19. Romics J. Ultrasound guided biopsy, a gold standard diagnostical test of the prostate cancer. Acta Chir Iugosl 2005;52:23–26. 20. Bostwick DG. Gleason grading of prostate needle biopsies: correlation with grade in 316 matched prostatectomies. Am J Surg Pathol 1994;18:796–803. 21. Spires SE, Clbull ML, Wood DP Jr. Gleason histologic grading in prostate carcimoma: correlation of 18 gauge core biopsy with prostatectomy. Arch Pathol Lab Med 1994;118:705–708. 22. Steinberg DM, Sauvageot J, Piantadosi S, Epstein JI. Correlation of prostate needle biopsy and radical prostatectomy gleason grade in academic and community settings. Am J Surg Pathol 1997;21:566–576. 23. Tomaskovic I, Bulimbasic S, Custovic Z, Reljic A, Kruslin B, Kraus O. Correlation of gleason grade in preoperative prostate biopsy and prostatectomy specimens. Acta Clin Croat 2003;42:225–227. 24. Cohen MS, Hanley RS, Kruteva T, et al. Comparing the gleason prostate giopsy and gleason prostatectomy grading system: the Lahey Clinic Medical Center experience and an international meta-analysis. Eur Urol 2008;54:371–381.