Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Electrocardiography wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Myocardial infarction wikipedia , lookup
Coronary artery disease wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Analysis of Left Ventricular Pressure
During Isovolumic Relaxation
in Coronary Artery Disease
D.S. THOMPSON, M.B., C.B. WALDRON, M.SC., S.M. JUUL, M.SC.,
N. NAQVI, M.B., R.H. SWANTON, M.D., D.J. COLTART, M.D.,
B.S. JENKINS, M.B., AND M.M. WEBB-PEPLOE, M.B.
SUMMARY When a decrease in left ventricular isovolumic pressure is considered as an exponential, the
rate of relaxation can be defined by a time constant (T). Previously, T has been calculated from the slope of
In (pressure) against time, but this method is valid only when the asymptote of the exponential is zero. In this
study two estimates of T were made: Tin from the slope of In (pressure) against time, and TEXP by a method of
exponential analysis that also estimated the asymptote. These techniques were applied to measurements of left
ventricular pressure made at increasing pacing rates in three groups of patients catheterized for chest pain:
normal coronary arteriograms; group 2 (n = 9) coronary artery disease (CAD) but no
group 1 (n = 9)
angina or lactate production during pacing; and group 3 (n = 9) CAD and angina during pacing. Tjn was
always shorter than TEXP, and in groups 1 and 2 TEXP was dependent on heart rate, whereas Tin was not. The
asymptote was negative, and increased toward zero during pacing in groups 1 and 2. The difference between
TEXP and Tin could be related to the value of the asymptote. In 18 of 20 beats tested, pressures calculated from
TEXP and the asymptote were in closer agreement with measured pressures than were the pressures predicted
by T1n. Despite their different values, TEXP and Tin each distinguished between the three groups. Although the
choice of an exponential model is arbitrary, isovolumic pressure decrease approximates to a single expontial;
but this study suggests that both T and the asymptote are variable.
-
Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017
used these techniques to analyze pressure measured
during pacing in patients who were evaluated for chest
pain.
THE STUDY of the decrease in left ventricular pressure during isovolumic relaxation is hindered by the
lack of a method of quantifying pressure decrease that
can be used to compare individual subjects. The maximal rate of pressure decrease (dP/dt min) can decrease during ischemia,l but dependence on endsystolic pressure and fiber length limits its value.2'
More recently, a pressure decrease from the point of
dP/dt min has been treated as a single exponential,
which allows derivation of a time constant that
describes relaxation.4 6 The time constant is calculated
as the negative reciprocal of the slope of ln (pressure)
against time, and the correlation coefficient is used to
test the validity of the monoexponential model.4-6 The
time constant so derived is relatively insensitive to
heart rate, ventricular volume and the level from
which pressure decreases,4 7 8 but is prolonged dur-
Patients and Methods
Twenty-seven patients (ages 34-59 years) limited by
chest pain were studied during diagnostic cardiac
catheterization for suspected coronary artery disease.
The protocol was approved by the hospital ethical
committee, and each patient gave written consent.
Cardiac Catheterization
The catheterization procedure has been described in
detail elsewhere.10 Briefly, after routine pressure measurements and coronary arteriography, a catheter-tip
micromanometer (Telco MM52 or #5 Millar) was
positioned in the left ventricle through a long sheath.'1
A Ganz pacing and thermistor catheter was advanced
into the coronary sinus from a left antecubital vein.
No measurements were made for at least 20 minutes
after coronary arteriography. Left ventricular pressure was measured and blood samples were drawn
from the left ventricle and coronary sinus at the basal
heart rate and at increasing paced rates. Left ventricular cineangiography was performed at the end of the
study.
ing ischemia.6'
This semilogarithmic method of estimating the time
constant of an exponential is valid only when the
asymptote of the exponential is zero. The zero
reference for pressure measurement is an external
point; one cannot assume that it corresponds to the
asymptote of ventricular pressure decrease or that the
asymptote remains constant under different conditions. In this study, we estimated the time constant of
isovolumic pressure decrease both from the plot of In
(pressure) against time and by a method of exponential analysis that also estimates the asymptote. We
Computer Analysis of Pressure Signals
The sternal angle was used as zero reference for all
pressure measurements. Left ventricular pressure was
measured simultaneously by the catheter-tip micromanometer and by the lumen of the Telco (or the
long-sheath when the Millar catheter was used). The
signals were displayed on a Cambridge 12-channel
recorder and stored on tape (Phillips seven-channel
FM recorder) and analyzed off line with a Varian
computer (620/L-100).
From the Departments of Cardiology, Bioengineering and
Medicine, St. Thomas' Hospital, and the Department of Cardiology, Middlesex Hospital, London; and the Department of Cardiology, Royal Albert Edward Infirmary, Wigan, England.
Address for correspondence: Dr. D. S. Thompson, Department of
Cardiology, St. Thomas' Hospital, London SEI, England.
Received February 6, 1981; revision accepted July 2, 1981.
Circulation 65, No. 4, 1982.
690
ISOVOLUMIC PRESSURE DECREASE/Thompson et al.
The computer analyzed pressure signals in 9-second
periods, each of which was accompanied by a zero and
calibration signal for the fluid-filled pressure channel.
The record was broken into individual beats by computer recognition of the R wave of the ECG. The
micromanometer signal was digitized every 5 msec
and the fluid-filled pressure every 10 msec. After an
appropriate correction for time delay, the two signals
were matched; the correct zero and calibration for the
micromanometer were calculated by least-squares
regression and used in the analysis of that record.
Ideally, pressure should be analyzed from the point
of dP/dt min to mitral valve opening. As the latter
cannot be identified confidently from the left ventricular pressure signal, we used the period from the point
of dP/dt min to the time at which pressure decreased
to the level of end-diastolic pressure of the preceding
beat." 8 For each beat, the digitized micromanometer
signal during this period was analyzed in two ways.
Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017
Semilogarithmic Method
The semilogarithmic method assumes the asymptote of pressure fall is zero. Thus, P(,) = aebt, and In
P(t) = A + bt. The value of b was estimated from the
slope of ln (pressure) against time by least-squares
regression. The time constant (T1n) = -I /b.4
Exponential Method
The exponential method does not assume the
asymptote to be zero. Thus, P(t) = aebt + c. The
parameters a, b and c can be determined by considering three points equally spaced in time on a pressuretime curve. For three values of pressure at times o, m
and 2m, it can be shown that
b=
1
m
P(2m)
P(m)
PJM)
(0)
and the asymptote (c) is given by c = P(o) - a, where a
(P(m)
P(O))/(e-bM
1).
These equations were applied to the digitized pressure signal as follows: The parameters were calculated
using sets of three points - P(O), P(20) and P(o), where
0, 20 and 40 refer to time in msec after dP/dt min
then P(6,), P(25) and P(,,) . . . until all the points were
used. The mean values of b and c were calculated for
each beat. The time constant (TEXP) = -1l/b. The
computer also calculated KVmax (from developed
pressure), dP/dt max and dP/dt min for each beat.
The values that appear in the results are the mean of
all the beats in a 9-second record. The beats were displayed during analysis, so that ectopic, postectopic
and technically unsatisfactory beats could be excluded. The digitized pressure record could be
retrieved from the computer to test the predictions of
the time constants with measured pressure.
Measurement of Lactate Concentration
Left ventricular and coronary sinus blood were
sampled simultaneously. Samples were added to an
aliquot of perchloric acid, put on ice and stored at
-20°C. Lactate concentration was estimated by a
691
fluorometric method.'2 The extraction ratio is defined
as the difference in concentration between arterial and
coronary sinus blood expressed as a percentage of
arterial concentration.
Statistical Methods
For individual beats, pressures at 5-msec intervals
were calculated for the period of isovolumic pressure
decrease from the parameters of the two models of
pressure decrease and compared with the digitized
micromanometer signal. The chi-square test was used
to test the hypothesis that predicted and observed
pressures were identical. The ratio of the residual to
the total sums of squares (RSS/TSS) was used to estimate the proportion of the total variance in the
observed pressure-time curve that could not be accounted for by the predictions of the model. Thus, the
smaller the ratio the better the agreement between
predicted and observed pressure. Elsewhere, the t test
and linear regression were used. Values are expressed
as mean ± SEM andp < 0.05 is considered significant.
Results
The 27 patients were divided into three groups on
the results of coronary arteriography and effects of
pacing. Group 1 included nine patients with normal
coronary arteries who did not have pain or produce
lactate on pacing. Group' 2 included nine patients with
coronary artery disease in whom pacing did not
provoke angina' or lactate production. Group 3 included nine patients with coronary arterydisease who
had angina during pacing. The details of the three
groups are listed in tables 1-3.
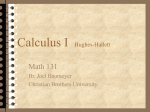
Twenty heart beats from eight patients, including at
least two patients from each group, were used to test
the goodness 'of fit of the pressure decrease predicted
by the two models with measured pressure (fig. 1.) Exponential analysis estimated the time constant (TEXP)
to be 66 msec and the asymptote of pressure decrease
to be -32 mm Hg; the semilogarithmic method gave
an estimate of 32 msec for the time constant (Tln).
When predicted and observed pressures are compared,
X2 = 0.52, p > 0.9995 and RSS/TSS = 0.3% for the
exponential model, and x2 = 7.54, 0.95 < p < 0.99
and RSS/TSS = 4.5% for the semilogarithmic
method. Figure IC shows the plot of In (pressure)
against time from which Tl, was derived. The points
do not form a straight line, the slope becoming steeper
at low values of In (pressure); despite this, r = -0.97.
In figure 1D, this departure from the linear has been
abolished by plotting In (pressure - asymptote)
against time. Linear regression now yields a time constant of 67 msec instead of 32 msec, and r = -0.99.
Large differences were found between TEXP and Tln in
all three groups, particularly when the estimate of the
asymptote was low (fig. 2). The fit of pressure
predicted by the exponential model to measured pressure was superior to the predictions of the semilogarithmic model in 18 of 20 beats tested. For the exponential model, the range of values was X2 - 0.33, p
> 0.9995, RSS/TSS = 0.1%, to X2 = 5.4, 0.95 <p <
0.99, RSS/TSS 2.6%; for the semilogarithmic model,
CIRCULATION
692
VOL 65, No 4, APRIL 1982
TABLE 1. Angiographic and Basal Hemodynamic and Metabolic Results
Group I (n = 9)
Group 2 (n = 9)
5 one-vessel
Normal
Coronary arteriograms
1 two-vessel
3 three-vessel
0.66 ± 0.016
0.56 ± 0.055
Ejection fraction
59 ± 4
End-diastolic volume index (ml/m2)
69 ± 7
3.07 ± 0.32
2.54 ± 0.23
Cardiac index (1/min/m2)
LVEDP (mm Hg)
6.3 ± 2.0
6.2 ± 1
1527 ± 58
1745 ± 110
dP/dt max (mm Hg/sec)
91.8 ± 5
95 ± 8
KVmax (sec-1)
-1844 ± 104
dP/dt min (mm Hg/sec)
-1825 ± 87
25.7 ± 4.3
18.5 ± 4.8
Lactate extraction ratio (%)
*p < 0.05, group 1 vs group 3.
+p < 0.01, group 1 vs group 3.
+p < 0.025, group 2 vs group 3.
§p < 0.005, group 2 vs group 3.
Abbreviations: LVEDP left ventricular end-diastolic pressure.
Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017
X2= 0.5,p > 0.9995, RSS/TSS = 0.5%, to x2 = 23.5,
0.3 <
p
Group
1
< 0.4, RSS/TSS
=
9%.
The patients in group 1 had good left ventricular
function and normal myocardial lactate extraction
(table 1).'With pacing,'dP/dt max increased and left
ventricular end-diastolic pressure decreased between
the highest and lowest pacing rates, and lactate extraction ratio did not change significantly (table 2).
The estimates of TEXp and the asymptote are shown
in figures 3A and 3D. Between the lowest and highest
heart rates, TEXP decreased from 55 4 msec to 34 i
2'msec (p < 0.001), and the asymptote increased from
-25 3 mm Hg to -9 ±'2 mm Hg(p < 0.01). There
was a significant inverse relation between TEXP and
heart rate (r =-0.75, p < 0.01) and a positive correlation between the asymptote and heart rate (r =
0.68, p < 0.01). In all instances, TEXP was greater than
Tln. Between the lowest and highest heart rates, Tln
decreased from 32 + 3 msec to 24 ± 3 msec (p <
0.05), but when all pacing rates were considered
together, Tln was not related significantly to heart
rate. The ratio of the time available for relaxation (the
Group 3 (n-9)
3 two-vessel
6 three-vessel
0.58 ± 0.03
95 ± 14*
2.34 ± 0.15*
12.6 ± 1.3
1282 ± 49t§
82 ± 5
-1451 ± 80t:
11.5 ± 3.5t
interval between dP/dt min and end-diastole) to TEXP
decreased as heart rate increased (r = -0.8,p < 0.01),
but never fell below 3 (fig. 4A).
Group 2
The basal hemodynamic results of the patients in
2 did not differ significantly from those in group
1, although ejection fraction, cardiac index and myocardial lactate extraction ratio tended to be lower
and end-diastolic volume index higher. With pacing,
KVmax increased, but dP/dt max, end-diastolic
pressure and lactate extraction ratio did not change
significantly.
The estimates of TEXP and the asymptote are shown
in figures 3B and 3E. Between the lowest and highest
heart rates, TEXP decreased from 57 ± 2 msec to 46
3 msec (p < 0.01), and when all pacing rates were considered, TEXP related inversely to heart rate (r =
-0.61, p < 0.01). The asymptote increased from -24
4 mm Hg to -15 4 mm Hg (NS), and there was a
weak correlation between the asymptote and heart
rate (r = 0.44, p < 0.05). T,n decreased from 35 ± 3
msec to 32 ± 3 msec (NS). The ratio of the time
available for relaxation to TEXP decreased as pacing
group
TABLE 2. Hemodynamic and Metabolic Changes Induced by Pacing
Group 1
Group 2
Heart rate
Heart rate
LVEDP
Minimum
6.3 ± 2
(mm Hg)
1527 ± 58
dP/dt max
(mm Hg/sec)
KVmax
Maximum
2.9 ± 1.5
Minimum
6.2 ± 1.1
p < 0.05
1745 ± 110
p<0.001
-1825 ± 87
(mm Hg/ sec)
Lactate extrac- 27.5 ± 3.6
tion ratio
100.4 ± 82
95 ± 7.8
=
1853 ± 146
1282 ± 49
-1823 ± 138
8
82 ± 5
22.7 ± 4.3
-1632
161
left ventricular end-diastolic pressure.
NS
4
-1451 ± 80
-1482
86
NS
13.4 ± 3.2
18.5 ± 4.8
82
NS
NS
NS
1614 ± 79
p<0.005
106
-1844 ± 104
NS
Maximum
(angina)
17.1 ± 3.0
NS
p < 0.05
(%)
Abbreviations: LVEDP
Minimum
12.6 ± 1.3
NS
NS
dP/dt min
Maximum
5.2 ± 1.9
NS
2083 ± 8.2
91.8 ± 5.1
Group 3
Heart rate
-14.7 ± 10.4
11.5 ± 3.5
p < 0.05
ISOVOLUMIC PRESSURE DECREASE/Thompson et al.
in the
TABLE 3. Mean Values of TEXP, the Asymptote and
Three Groups of Patients
Group I
Group 2
Group 3
Basal heart rate
77 ±6
85 ± 7
Heart rate
86 ± 6
57 ±2
80 ±6§**
55 ±4
TEXP(msec)
Asymptote
-24 ± 4
-38 ± 4¶
(mm Hg)
-25 ± 3
49 ± 3§¶
T1 (msec)
31 ± 3
35 ± 3
Highest pacing rate
129 ± 5
127 7
Heart rate
132 ± 5
47 ± 3t
84 10§**
34 ± 2
TEXP (msec)
Angina
Asymptote
-15 4
-9 ± 2
-35i 8+
(mm Hg)
24 ± 2
32 3*
50 6§¶
Tln (msec)
Group I vs group 2:
*p < 0.05.
Tln
693
group 1 were calculated using the results at the second
highest pacing rate for three of the nine patients. At
the basal heart rate, the mean values of TEXP, the
asymptote and Tl, were similar in groups 1 and 2, but
TEX, and T1n were longer and the asymptote lower in
group 3 than in groups 1 and 2. At the highest pacing
rate, TEXP and Tln were longer in group 2 than in
group 1, and greater in group 3 than in groups 1 and 2.
The asymptote was similar in groups 1 and 2, but
lower in group 3 than in groups 1 and 2.
Discussion
Treating the decrease in left ventricular pressure
from the point of dP/dt min as a monoexponential
(B)
(A)
100
100
Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017
tp<0.01.
Group I vs group 3:
tp < 0.05.
§P<O.OI.
Group 2 vs group 3:
< 0.05.
¶p
**
<0.01.
| 50
0:
ui
rate increased (r = -0.83, p < 0.01), and the lowest
value was 3.0 (fig. 4B).
Group 3
Basal cardiac index, dP/dt max, dP/dt min and
myocardial lactate extraction ratio were significantly
lower and end-diastolic volume index higher in group
3 than in group l, and dP/dt max and dP/dt min were
lower than in group 2. At the highest pacing rate, all
nine patients experienced angina, which was associated with a significant reduction of myocardial
lactate extraction from resting levels. Despite angina,
dP/dt max increased significantly between lowest and
highest pacing rates; dP/dt min did not change
significantly, and in only one patient was a large
reduction observed during angina (from -2041 to
-900 mm H:g/sec).
There was considerable individual variation in TEXP
both at rest and during pacing (figs. 3C and 3F), and
TEXP failed to decrease as heart rate increased. The
mean values at the lowest and highest pacing rates (80
± 6 msec and 84 ± 10 msec) did not differ
significantly. At the highest heart rate, during angina,
several patients had very high values of TEXP (range
63-131 msec). Similarly, the asymptote did not
change significantly with pacing, and the values
showed considerable individual variation. Tl, was
similar at the lowest (49 ± 3 msec) and highest (50 ± 6
msec) pacing rate. The ratio of time available for
relaxation to TEXP decreased as heart rate increased (r
=-0.53, p < 0.02), and was 3 or less in each patient
during angina (fig. 4C).
Comparison of Groups
The mean values of TEXP, the asymptote and T1n are
listed in table 3. To allow comparison of the three
groups to be made at similar heart rates, the means for
o
uI
25
50
TIME
75
("SEC)
(c)
w
50
25
75
I
~,(D)
4,1 3
4.0
a.0
ON
-
25
50
2.0
75
25
50
75
TIME (MSEC)
FIGURE 1. Analysis of the decrease in left ventricular pressure from the point of dP/dt min (time o) until it reaches the
level of end-diastolic pressure of the preceding beat. (A)
Dots represent measured left ventricular pressure digitized
at 5-msec intervals. The solid line indicates the course of the
pressure decrease predicted by exponential analysis. For this
beat, TEXP = 66 msec and the asymptote =-32 mm Hg. (B)
The same beat as in panel A. Dots represent measured pressure digitized at 5-msec intervals. The solid line indicates the
course of the pressure decrease predicted by semilogarithmic analysis. For-this beat, Tl,, = 32 msec. (C) The plot
of In (pressure) against time for the same beat. T1, was
derived by linear regression of this plot. The plot deviates
from linearity at low values of In (pressure), but r = -O 97
(D) The plot of In (pressure - asymptote) against time for
the same beat. The plot is linear, r = -0.999, and the slope
gives a time constant of 67 msec, which is in close agreement
with TEXP (66 msec). In this and subsequent figures, TEXP =
time constant estimated exponentially;' T1,, = time constant
estimated semilogarithmically.
CIRCULATION
694
2.0
0 @
0
0
allows the derivation of a time constant that describes
isovolumic relaxation.4 5 7 As the time between dP/dt
min and mitral valve opening is short, any model
predicting rapid pressure decrease will show some
success. The choice of an exponential model is arbitrary, and statistical analysis cannot confirm that
pressure decrease is exponential, but merely tests how
closely the predictions of the model approximate
measured pressure.
In previous studies, the time constant has been
calculated as the negative reciprocal of the slope of In
(pressure) against time.4-9 This method is valid only
when the asymptote of pressure fall is zero. Our
results suggest the asymptote is lower than zero
reference pressure and dependent on heart rate.
In figure 5A, all three hypothetical pressure-time
curves are monoexponential and have the same time
constant but different asymptotes. The slope of ln
(pressure) against time (fig. 5B) differs for each value
of asymptote, and Tln is correct only when the asymptote is zero. In addition, when the asymptote is not
zero, the relation between In (pressure) and time is a
curve, so the slope determined by linear regression
depends upon the part of the curve analyzed, and
hence the level to which pressure decreases (fig. 6).
0
0
0
z
0
*
0.
x
LL
0
1.0
Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017
-20
-40
ASYMPTOTE (MMHIG)
FIGURE 2. Relationship between TEXP/ Tlf and the asymptote for the patients in group 1. The ratio increases as the
asymptote decreases further below zero.
A GROUP
120
1201
i
VOL 65, No 4, APRIL 1982
120i
B GROUP II
R = -0. 80
R
=
-0.61
00
60
0
0
.es.
0
60
v
yTGROQU..ILL
V
90
90
90
C
0
0
V
y, yVV
.
60
x
w
S
00
30
C
0
0
:~~~~~~
HEART RATE
0%
30
170
0
30
0
O1
50
50
170
HEART RATE
0
0
.
0
-20
-20
0
I
*
CD
x
*
-40
0
0 9
0
0
V
V
V
0
0
I
v
O*t
R = O.44
F.
GROUP 1 LI
F
0
0
170
HEART RATE
V
C,,
-60
I
-60
0
sn
170
HEART RATE
50
170
HEART RATE
50
17
170
HEART RATE
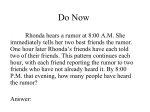
FIGURE 3. Individual values of TEXP and the asymptote in the three groups. (A) Group 1. Relation
between TEXP and heart rate (r = -0.80, p < 0.01). (B) Group 2. Relation between TEXP and heart rate (r =
0.61, p < 0.01). (C) Group 3. Values before (dots) and during angina (triangles) are shown. TEXP and heart
rate were not related significantly. (D) Group 1. Relation between asymptote and heart rate (r = 0.68, p <
0.01). (E) Group 2. Relation between asymptote and heart rate (r = 0.44, p < 0.02). (F) Group 3. Values
before (dots) and during angina (triangles)
significantly.
are shown. The
asymptote and heart rate were not related
ISOVOLUMIC PRESSURE DECREASE/Thompson et al.
A
9
7
5
3
1
170
130
90
50
HEART RATE
9
7
c
9
B
7
*
*
.
0
5
5
0
Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017
.111
1
.9
3
3-
L
TV "
NX
1
50
90
130
170
50
130
90
170
HEART RATE
HEART RATE
FIGURE 4. The ratio of the time available for relaxation
(the interval between dP/dt min and end-diastole) to TEXP is
plotted on the abscissa. This ratio has been used as an index
of how completely the ventricle relaxes between beats. For
this model of pressure decrease, P(t) = aebt + c, or P(t) =
ae TEXP+ c. When t = the interval between dP/dt min and
end-diastole, the percentage of relaxation that can occur in
this period = (1 - Pe )TEXP 100. For ratios of t: TEXP of
1, 2, 3 and 4, relaxation would be 63%, 86%, 95% and 98%
complete before the next beat. (A) Group 1. The ratio
declined as heart rate increased (r = -0.80, p < 0.01). The
lowest value was 3.0. (B) Group 2. The ratio declined as
heart rate increased (r = -0.83, p < 0.01). The lowest value
was 3.0 (C) Group 3. Values before (dots) and during
angina (triangles) are shown. During angina the ratio was
3.0 or less in all nine patients. The ratio decreased as heart
rate decreased (r = -0.53, p < 0.02), but to lower values
than in groups I and 2.
695
These factors have a large effect on the slope, but little
effect on the correlation coefficient. Therefore, Tin is
an unreliable estimate of the time constant, and the
correlation coefficient does not test its validity.
Tin is correct only where the asymptote and zero
reference pressure coincide, and the greater the
difference between them, the greater the inaccuracy of
Tin. Thus, Tin for a given beat will depend upon the
choice of zero reference. Had our reference pressure
been at the midchest level rather than at the sternal
angle, the values of Tin would have been slightly
longer.
The exponentially derived time constant (TEXP) is
independent of the asymptote. As it is calculated from
differences in pressure between successive points in
time, TEXP is also independent of absolute pressure.
Thus, TEXP for a given beat will be the same whether
pressure is measured with respect to the sternal angle,
midchest, or intrathoracic pressure. The estimate of
the asymptote depends on absolute pressure; a given
change in reference pressure produces an equal but opposite change in the asymptote.
Although the exponential model has these advantages, it is based on a more complicated model. The
asymptote cannot be measured, and the only
statistical test that can be applied is the comparison of
the predictions of the whole model with measured
pressure. In all examples tested, predicted and
observed pressures agreed closely, and in 18 of 20
beats the exponential model was superior to the semilogarithmic model. The TEXP was always longer than
Tln, and, as would be expected, the ratio of TEXP to Tln
decreased as the asymptote increased toward zero.
The relation between TEXP: Tin and the asymptote was
not precise, because Tln depends upon both the asymptote and the level to which pressure decreases. This
discrepancy between TEXP and Tln should be
eliminated by calculating Tin from the plot of In
(pressure - asymptote) against time (fig. 1D).
The independence of Tln and heart rate can be explained by changes in the asymptote. At low heart
rates, when the asymptote was negative, Tln underestimated markedly the time constant, but at high
heart rates, when the asymptote increased toward
zero, T1i was in closer agreement with the shorter time
5
100
oB
u
:3
\c
co
1
0
70
TIME (MSEC)
70
0
TIME (MSEC)
FIGURE 5. (A) All three pressure-time
curves are monoexponential. Each has a
time constant of 50 msec, but different
asymptotes: A, 20 mm Hg; B, 0 mm Hg; C,
-20 mm Hg. (B) Plot of In (pressure)
against time of three exponentials in panel
A. For curve A, r = -0.99, although the
slope becomes shallower at low values of In
(pressure). Tln = 78 msec. For curve B, r =
-1.0 and Tln = 50 msec. For curve C, r =
-0.98, although the slope becomes
progressively steeper at low values of In
(pressure). Tln = 26 msec.
CIRCULATION
696
90
I;;x
E
ac
n
w
'acn
a:
0.
0
70
0
TIME (MS)
TIME
(MS)
4.5
UJ
n
Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017
--
1.0I
80
0
TIME (MS)
FIGURE 6. (upper left) The two pressure-time curves are
monoexponentials, having the same time constant (50 msec)
and asymptote (-20 mm Hg). (upper right) The plot of In
(pressure) against time of the curves A and B shown in the
left-hand panel. Linear regression of A yields r = -0.97 and
T1n = 23 msec, and of B yields r = -0.99 and Tln = 29 msec.
Thus, when the asymptote is negative, an upward shift of the
pressure-time curve results in prolongation of Tln, even
though the time constant has not really changed. (below)
The plot of ln (pressure) against time for a monoexponential of which the time constant is 50 msec and the asymptote
-20 mm Hg. Pressure decreases from 0-40 msec and from
45-75 msec have been analyzed separately. For 0-40 msec, r
= -0.999 and Tln = 36 msec; for 45-75 msec, r = -0.99
and Tl, = 18 msec. Thus, the early and late parts of the plot
yield different values of T1..
constant. A similar explanation for the load-independence of TIn4 7 cannot be excluded.
Isolated cardiac muscle relaxes slowly during
hypoxia. 13 In human coronary disease, ventricular
relaxation is incoordinate,'4, 16 and this, rather than
slow relaxation of myocardial fibers, might be responsible for prolongation of TEXP. Isovolumic pressure
decrease is the net result of relaxation of the different
regions of ventricular myocardium and, although it
approximates to a monoexponential, can be determined by several exponentials with different time constants, asymptotes and times of onset. If pressure
decrease is determined by several identical exponentials, each starting at a slightly different time, exponential analysis of measured pressure will yield the
time constant and asymptote of the constituent exponentials. Thus, in an exponential model, incoor-
VOL 65, No 4, APRIL 1982
dination alone does not prolong the time constant of
pressure decrease.
Incoordinate relaxation has been studied by analyzing the early and late parts of isovolumic pressure
decrease separately, and in patients with coronary disease, T1n derived from the first 40 msec is longer than
T1n derived from the later points;"6 but this does not
provide evidence of incoordination or allow its quantification, because when the asymptote is negative, as
is usually the case, the ln (pressure)-time relation is a
curve, and linear regression of its early and late parts
inevitably yields two different values of T1n (fig. 6).
Ventricular volume and contractility have little
effect on Tn'4 I but one cannot assume that TEXP is
similarly independent. Prolongation of TEXP might
therefore be caused by ventricular dilatation or depressed contractility rather than by a specific effect
of ischemia on relaxation. Within the three groups,
TEXP could not be related to indexes of contractility or
ventricular volume. There was considerable overlap
between groups 2 and 3 in values of KVmax, ejection
fraction and end-diastolic volume, but TEXP was significantly longer in group 3. Our observations suggest
that prolongation of TEXP is due to ischemia, and may
precede angina and lactate production.
The asymptote is the level to which pressure would
decline if isovolumic pressure decrease continued indefinitely, rather than the pressure to which the ventricle would relax if it did not fill; for it cannot be
assumed that the process underlying isovolumic
relaxation continues into diastole. Indeed, the low
values of the asymptote during angina are contrary to
what would be expected if it represented pressure at
complete relaxation. The asymptote is a mathematical
term that, in conjunction with TEXP, describes isovolumic pressure decrease and is applicable only to
this part of the cardiac cycle.
Weisfeldt et al.5 considered that the process
described by Tln continues throughout diastole,' so
that the ratio of the interval between dP/dt min
and end-diastole to T1n measures how completely the
ventricle relaxes (fig. 4). Ratios less than 3.5 are
associated with an upward shift of the pressure-dimension curve of the canine ventricle, suggesting that incomplete relaxation alters diastolic properties.5
Because Tln depends upon the level to which pressure
decreases, the association of low value of this ratio
and high end-diastolic pressure may not be causal. We
used TEXP to calculate the ratio, which was always 3 or
less during angina; but end-diastolic pressure did not
increase with pain in all patients, suggesting that the
ratio is a poor predictor of diastolic properties. If this
is the case, calculating the ratio adds no information,
as the differences in its value between the groups are
due solely to differences in TEXP.
We conclude that although the choice of an exponential model is arbitrary, the isovolumic pressure
decrease closely approximates a single exponential.
Our results suggest that in the human heart, an exponential model requires both the time constant and
ISOVOLUMIC PRESSURE DECREASE/Thompson et al.
the asymptote to be variable. Although TEXP and Ti0
each discriminated between the three groups of patients, Tln measures the time constant only when the
asymptote coincides with zero reference pressure.
References
1.
2.
3.
4.
5.
Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017
6.
7.
McLaurin LP, Rolett EL, Grossman W: Impaired left ventricular relxation during pacing-induced ischaemia. Am J Cardiol
32: 751, 1973
Weisfeldt ML, Scully HE, Frederiksen J, Rubinstein JJ, Pohost
GM, Beierholm E, Bello AG, Daggett WM: Hemodynamic
determinants of maximum negative dp/dt and periods of
diastole. Am J Physiol 227: 613, 1974
Cohn PF, Liedtke AJ, Serur J, Sonnenblick EH, Urschel CW:
Maximal rate of pressure fall (peak negative dP/dt) during ventricular relaxation. Cardiovasc Res 6: 263, 1972
Weiss JL, Frederiksen JW, Weisfeldt ML: Hemodynamic
determinants of the time course of fall in canine left ventricular
pressure. J Clin Invest 58: 751, 1976
Weisfeldt ML, Frederiksen JW, Yin FCP, Weiss JL: Evidence
of incomplete left ventricular relaxation in the dog. Prediction
from the time constant for isovolumic pressure fall. J Clin
Invest 62: 1296, 1978
Mann T, Goldberg S, Mudge GH, Grossman W: Factors contributing to altered left ventricular properties during angina
pectoris. Circulation 59: 14, 1979
Karliner JS, Lewinter MM, Mahler F, Engler R, O'Rourke
RA: Pharmacologic and hemodynamic influences on the rate of
isovolumic left ventricular relaxation in the normal conscious
697
dog. J Clin Invest 60: 511, 1977
8. Frederiksen JW, Weiss JL, Weisfeldt ML: Time constant of
isovolumic pressure fall: determinants in the working left ventricle. Am J Physiol 235: H701, 1978
9. Taw RL, Lawrence SC, Griffith C. Conti R, Ducci H, Weisfeldt
ML: Impaired isovolumic relaxation during pacing induced
ischemia in man. (abstr) Circulation 54 (suppl II): 11-6, 1976
10. Thompson DS, Naqvi N, Juul SM, Coltart DJ, Jenkins BS,
Webb-Peploe MM: Haemodynamic and metabolic effects of
atenolol in patients with angina pectoris. Br Heart J 43: 668,
1980
11. Brooksby IAB, Swanton RH, Jenkins BS, Webb-Peploe MM:
Long sheath technique for introduction of catheter tip micromanometer or endomyocardial bioptome into left or right
heart. Br Heart J 36: 908, 1974
12. Hohurst HJ, Kreutz FM, Buich T: Metabolitgehalte und
Metabolitkonzentationen in der Leber der Ratte. Biochem Z
332: 18, 1959
13. Bing OH, Keefe JF, Wock MJ, Finkelstein LJ, Levine HJ: Tension prolongation during recovery from myocardial hypoxia. J
Clin Invest 50: 660, 1971
14. Upton MT, Gibson DG, Brown DJ: Echocardiographic assessment of abnormal left ventricular relaxation in man. Br Heart J
38: 1001, 1976
15. Gibson DG, Prewitt TA, Brown DJ: Analysis of left ventricular wall movement during isovolumic relaxation and its relation to coronary artery disease. Br Heart J 38: 1010, 1976
16. Pouler H, Rousseau M, Wijns W, Mengeot P, Detry JM,
Brassueur L: Changes in left ventricular relaxation pattern during atrial pacing in ischaemic heart disease. VIlIth European
Congress of Cardiology, 1980, p 81
Analysis of left ventricular pressure during isovolumic relaxation in coronary artery
disease.
D S Thompson, C B Waldron, S M Juul, N Naqvi, R H Swanton, D J Coltart, B S Jenkins and
M M Webb-Peploe
Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017
Circulation. 1982;65:690-697
doi: 10.1161/01.CIR.65.4.690
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1982 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is located on
the World Wide Web at:
http://circ.ahajournals.org/content/65/4/690.citation
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally
published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the
Editorial Office. Once the online version of the published article for which permission is being requested is
located, click Request Permissions in the middle column of the Web page under Services. Further
information about this process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/