Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
J Am Acad Audiol 6 : 150-162 (1995)
Preliminary Descriptions of Transient-Evoked
and Distortion-Product Otoacoustic Emissions
from Graduates of an Intensive Care Nursery
Brenda M. Bergman*
Michael P. Gorga*
Stephen T. Neely*
Jan R. Kaminski*
Kathryn L. Beauchaine*
Jo Peters*
Abstract
Transient-evoked (TEOAE) and distortion-product otoacoustic emissions (DPOAE) were
measured in 51 graduates of an intensive care nursery and compared to data obtained from
80 normal-hearing children and adults . All infants had click-evoked auditory brainstem
responses (ABR) at 30 dB nHL or less while the older subjects had pure-tone thresholds of
20 dB HL or less for octave frequencies from 250 to 8000 Hz . OAE data were collected using
commercially available devices. All data were analyzed in terms of emission amplitude, emission-to-noise ratio, and response reproducibility as a function of frequency. DPOAEs were
measured at three points per octave between f2 frequencies of approximately 500 and 8000
Hz . TEOAEs were elicited by clicks and were analyzed in both octave and'/3-octave bands
centered at frequencies from 500 to 4000 Hz, as well as in the broadband condition . In addition, stimulus amplitudes for the clicks used to elicit TEOAEs were analyzed within octave
and 1/3-octave bands to determine whether any age-related differences in responses can be
accounted for on the basis of stimulus differences . Both emission amplitude and noise amplitude were greater in neonates than adults, although there was variability across frequency.
Emission-to-noise ratio and response reproducibility were more similar between groups . For
TEOAEs, high-frequency emission-to-noise ratios were larger in neonates compared to older
subjects, while the reverse was true in the lower frequencies . Less obvious frequency effects
were observed for DPOAEs . These findings are discussed in relation to the potential use of
OAEs as screening measures for neonatal hearing loss .
Key Words: Distortion-product otoacoustic emissions (DPOAEs), infants, intensive care
nursery (ICN), otoacoustic emissions (OAEs), transient-evoked otoacoustic emissions
(TEOAEs)
here has been considerable interest in
otoacoustic emissions (OAEs) since they
T were first described by Kemp (1978) .
The presence of OAEs provides evidence of the
existence of normal nonlinear properties within
the cochlea. One consequence of cochlear damage is a reduction or loss of nonlinear behavior,
which is reflected by a loss of OAEs . As a con-
'Boys Town National Research Hospital, Omaha,
Nebraska
Reprint requests : Brenda Bergman, Boys Town
National Research Hospital, 555 North 30 Street, Omaha,
NE 68131
15 0
sequence, ears with hearing loss are unlikely to
produce OAEs . In their application with newborns, OAE measurements may provide basic
information regarding the development of
cochlear nonlinearities but also could be useful
in the early identification of hearing loss . A
number of screening programs are currently
investigating the use of OAE testing as a method
of screening for hearing loss (Kemp and Ryan,
1991 ; White et al, 1993).
Data are accumulating that describe OAEs
from the perinatal period in humans (e .g .,
Johnsen et al, 1983 ; Kemp et al, 1986 ; Norton
and Widen, 1990 ; Lafreniere et al, 1991 ; Stevens
et al, 1991 ; Uziel and Piron, 1991 ; Kok et al,
OAEs from ICN GraduatesBergman et al
1992 ; Smurzynski et al, 1993). Many of these
data have shown that it is possible to measure
OAEs in virtually all newborns with "normal
hearing." Further, there is evidence that OAEs
are larger in newborns compared to older children and adults with normal hearing (e .g., Norton and Widen, 1990 ; Kok et al, 1992). It is possible that both stimulus and response amplitudes
may be greater in infant ear canals due to their
smaller size compared to older subjects . Whether
this can account for differences in response
amplitudes remains undetermined . Almost all
available OAE data from infants are restricted
to TEOAEs . Few data exist that describe distortion-product otoacoustic emissions (DPOAEs)
(Lasky et al, 1992) or that compare TEOAEs and
DPOAEs from the same group of infants (Bonfils et al, 1992 ; Smurzynski et al, 1993). Data
reported by Gorga et al (1993b) suggest that
TEOAEs and DPOAEs, although differing in
their measurements, result in more similar test
performance, defined by their ability to separate
normal from impaired ears . They did report
some differences across frequency that are not
yet understood . Finally, detailed comparisons of
infant TEOAEs and DPOAEs to the OAEs
obtained from older subjects are only beginning
to emerge (e .g . the data of Smurzynski and Kim
[1992] for adults versus the data of Smurzyinski et al [1993] in neonates).
The present paper represents a preliminary
description of both TEOAEs and DPOAEs from
graduates of an intensive care nursery (ICN) and
compares these data to similar measurements
from normal-hearing older subjects . OAE amplitudes, noise amplitudes, OAE-to-noise ratios,
and response reproducibility are described and
compared for these two groups of subjects . In
addition, stimulus amplitudes for the clicks used
to elicit TEOAEs are analyzed within octave
and 1/3-octave bands in order to determine the
extent to which any age-related differences in
responses can be accounted for on the basis of
stimulus differences . We consider these data
preliminary in that they were obtained from
babies with normal hearing and thus can only
be used to estimate the false positive rate .
METHOD
Subjects
Fifty-one graduates from an ICN served as
one group of subjects . All babies spending more
than 24 hours in our ICN receive hearing screenings, mainly because risk registries tend to miss
as many as 50 percent of hearing-impaired
infants (Ellsmann et al, 1987). Thus, most but
not all of these babies presented with risk factors, such as prematurity, elevated bilirubin
(not necessarily requiring transfusion), and
treatment with potentially ototoxic drugs .
Twenty-seven subjects were males and 24 were
females. Their conceptional ages ranged from 35
to 45 weeks, but the infants were at least 7 days
old at the time of the test . Age at the time of the
test appears to be an important variable affecting the false positive rate (Kok et al, 1992).
ICN babies were tested just prior to hospital discharge on the same day on which ABRs
were measured . All babies had click-evoked
ABRs at 30 dB nHL or less (0 dB nHL = 35 dB
pSPL as measured in a 2-cc coupler) . Data are
also included from 80 normal-hearing children
and adults . These "older" subjects had audiometric thresholds of 20 dB HL (ANSI, 1989) or
less for octave frequencies from 250 to 8000 Hz
and no evidence of middle-ear dysfunction, based
on audiometric, immittance, and otoscopic examinations . No other subject selection criteria were
used .
Instrumentation
ABR stimuli were delivered through an
insert earphone (Etymotic, ER-3A) . Rarefaction
clicks were presented at a rate of 17 per second
and responses were measured between electrodes placed at the high-forehead and ipsilateral mastoid, with the center of the forehead
serving as ground . Responses were amplified
(100k), filtered (100-3000 Hz, 12 dB/octave),
digitized at a rate of 33k, and averaged (1024
stimuli) using a Bio-Logic Navigator. Each
response was replicated once.
TEOAEs were measured with the IL088
Otodynamic Analyzer at its default stimulus
conditions and in its nonlinear recording mode .
Default conditions were used because to date,
data do not exist that specify either stimulus or
response conditions that result in optimal OAE
test performance . Data from large samples of
both normal-hearing and hearing-impaired neonates are needed to develop these optimal conditions. In the absence of such well-defined criteria, we chose to use those conditions in routine
clinical use. An adult probe unit and impedancetip adapters were used for all measurements
with the older group of subjects while the
specially designed infant probe and its associated coupling cuffs were used with ICN graduates. Probe tips differed for infants and older
Journal of the American Academy of Audiology/Volume 6, Number 2, March 1995
subjects because of differences in ear canal size .
As a consequence, it was often more difficult to
obtain good seals in newborn ear canals . This
affected primarily the low-frequency energy in
the ear canal signal . The IL088 provides a fixed
voltage to its earphone, which, under default
stimulus conditions, produces a level of about 80
dB pSPL in adult ear canals for the highest-level
click in the stimulus ensemble (see below for
more details) . In an effort to achieve comparable sound pressures in infant ear canals, the
neonatal probe incorporates attenuation of 19 .5
dB . The noise rejection level was also set at the
default level of 45 dB SPL. If noisy test conditions precluded collection of responses at this
level, the rejection level was increased but did
not generally exceed 50 dB SPL.
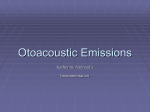
Figure 1 provides mean estimates (+ 1 standard deviation) of the amplitude of the clicks
used to elicit TEOAEs . These stimuli were analyzed in either octave (top) or 1/3-octave bands
(bottom) for both groups of subjects . It appears
that greater amplitude was achieved in the ears
of older subjects in low and mid frequencies,
while slightly greater stimulus amplitudes were
seen for infants in the higher frequencies. The
largest difference occurred in the 1/3-octave band
centered at 1260 Hz, where, on average, the
level in infant ears was 6.8 dB lower than that
achieved in older subjects . Averaged across all
frequency bands, the levels in the ear canals of
older subjects exceeded those observed in infants
by 2.6 dB . Possible explanations for these differences include differences in ear canal resonances and/or low-frequency leakage due to
imperfect seals of the probe in the ear canal of
infants. The stimuli appear to be similar between
the two groups in the higher frequencies with
greater difference in the lower frequencies.'
Other features of the IL088 system have
been described elsewhere (Kemp et al, 1986 ;
Bray and Kemp, 1987), and only a brief description will be provided here . A miniature microphone is used to measure ear-canal sound pressure changes following the presentation of 80usec clicks, presented at an overall rate of 50 per
second . These stimuli are presented in blocks of
four, with the first three clicks presented at
about 70 dB pSPL and one polarity while the
fourth click is presented at 80 dB pSPL but
opposite polarity. The responses from these four
'Differences in stimulus amplitudes as a function of frequency are less of a concern for DPOAEs, where amplitudes
were set on a frequency-by-frequency basis .
152
OCTAVE BAND
70
65
so
CIO
055
55
v
....
i ..........
.D
50
O - Older Children 6 Adults
H - ICN Graduates
Q
(470
1/3 OCTAVE BAND
t
E
7
E 65
N
60
55
50
500
1000
2000
Frequency (Hz)
4000
Figure 1 Mean estimates (+ 1 standard deviation) of
the amplitude of the TEOAE stimuli. Stimulus amplitude
is in dB re : equivalent SPL in a 10-kHz bandwidth. Top
panel shows octave-band analysis of the stimuli, and
bottom panel shows 1/3-octave band analysis .
clicks are added together, thus cancelling linear
(stimulus related) components of the ear-canal
waveform while leaving a portion of the nonlinear (cochlear) component of the response
intact . This process eliminates the stimulus
from measurement of the emission . The summed
responses from alternate blocks of clicks are
then stored in two buffers until each buffer
includes 260 responses, at which point the test
is terminated .
The IL088 software provides three useful
descriptions of these ear-canal waveforms.
TEOAE amplitude or level is estimated as the
cross-power spectrum of the two waveforms
while background noise is estimated as the
difference between these two waveforms. Response repeatability is estimated from the cross-
OAEs from ICN GraduatesBergman et al
correlation between the contents of the two
buffers and is expressed as a percentage .
While the above analyses are based upon
broadband responses, we were also interested in
knowing response and noise amplitudes, as well
as percent reproducibility, in frequency bands
associated with those frequencies typically evaluated during pure-tone behavioral audiometry.
To this end, the ear-canal waveforms were analyzed in octave and 1/-octave bands. Octave
bands were centered at the four octave frequencies from 500 to 4000 Hz, while the 1/3octave bands were centered at frequencies from
400 to 5040 Hz . For each octave and 1/3-octave
band, TEOAE level, noise amplitude, and percent reproducibility were estimated using a similar, although not identical, approach to that
used by the IL088 software to describe the
broadband response . Specifically, response amplitudes were estimated from the spectral magnitude of the sum of the two buffers, as opposed
to their cross-power spectrum (Gorga et al,
1993b; Prieve et al, 1993).
DPOAEs were measured using the CUBDIS
system distributed by Etymotic Research . This
system has been described in detail elsewhere
(Allen, 1990). Briefly, it includes an Ariel DSP16 signal processing board, an ER-10B low-noise
microphone system, a battery powered amplifier
providing 40 dB of gain, two ER-2A earphones,
a transformer, and software for extracting
acoustic distortion products from the ear-canal
waveform. Impedance-tip adapters were used to
couple the probe unit to the ear canals of older
subjects . As with TEOAE measurements, default
conditions of the CUBDIS system were used .
These included 200 samples of 20 .48-msec duration, resulting in a total time at each frequency
of 4 .096 seconds. No other stopping rule was
used and no noise reduction was performed.
Polyethylene tubing was cut to size and then
slipped over the probe unit in order to couple it
to the ear canal of neonates . Stimuli consisted
of two sinusoids that were independently generated by the two channels ofthe Ariel board and
then presented separately to the two ER-2A
earphones, the sound-delivery tubes of which
exited from the probe unit housing the low-noise
microphone system. The two sinusoids (f1 and f2)
were mixed acoustically in the ear canal. Stimulus conditions, which were identical to those
used in our previous work (Gorga et al, 1993a),
were as follows: f2/f1= 1 .2 ; L2 = 50 dB SPL; L1/L2
= 15 dB (L1 = level of lower frequency primary;
L2 = level of higher frequency primary) ; three
points per octave . These primary levels were
chosen based upon the assumption that the
interaction is greatest near the f2 place. Additionally, there is some indication that ears with
mild cochlear damage perform more normally
(i .e ., produce more normal DPOAE amplitudes)
for high-level primaries, but the responses
decrease rapidly and/or disappear for moderate level stimuli. During the calibration procedures included with CUBDIS, signal amplitude is measured in the ear canal of each subject so that specified primary levels are always
achieved, taking into account any effects of earcanal size .
Procedures
For both groups of subjects, OAE data collection was not initiated until hearing sensitivity had been evaluated . Depending upon
subject group, this meant that a pure-tone
audiogram or an ABR had been obtained prior
to OAE testing and the results were known to
the tester. Although middle-ear dysfunction
was not present in any of the older subjects, it
was not possible to be equally certain about
middle-ear status for the newborns . However,
the fact that these babies had ABRs at least as
low as 30 dB nHL and normal wave I latencies
for high-level stimuli reduces the likelihood
that significant middle-ear dysfunction was
present. Tests were performed on a randomly
selected ear in a quiet, although not soundtreated, environment . Older subjects were
seated comfortably, while neonates were sleeping in open cribs.
While data related to hearing sensitivity
were always obtained first, the order of OAE
measurements was alternated . For all subjects,
check-fitting procedures were performed prior to
TEOAE measurements in an effort to obtain a reasonably flat stimulus spectrum in the ear canal.
Recall from Figure 1 that this was more easily
achieved in older subjects compared to infants. For
DPOAE measurements, data collection began
only after calibration procedures indicated that
the two earphones produced reasonably flat spectra, which were similar to each other. The amount
of time devoted to probe fitting for either OAE
measurement was not captured .
RESULTS
Broadband TEOAE Responses
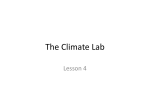
Figure 2 shows mean TEOAE amplitude
(circles), background noise (squares), TEOAE
Journal of the American Academy of Audiology/Volume 6, Number 2, March 1995
Figure 2 Mean TEOAE
amplitude (circles), background noise (squares),
TEOAE amplitude/noise (triangles), and percent reproducibility (diamonds) as a
function of frequency in both
older subjects (left column)
and in neonates (right column) . All amplitudes are
equivalent dB SPL in a bandwidth of 10 kHz .
30
1
1
-o
O - TEOAE Level
o - No"
_,o
30
A - TEOAE/Noise---
----
-I
- 1s
-w
loo
w
ii
i
i
0 - ti Relw o&xibility
Older Children 6 Adults
soo
1000
2000
4000
ICN Graduates
Be
soo
1000
2000
4000
so
Frequency (Hz)
amplitude/noise (triangles), and percent reproducibility (diamonds) as a function of frequency in both older subjects (left column)
and in neonates (right column). Error bars
represent ± 1 standard deviation. The results
of broadband response analyses, provided by
the IL088, are shown at the far right of each
panel. Although the broadband TEOAEs were
larger in neonates, estimates of background
noise also were larger by a comparable amount
(top row), resulting in TEOAE/noise that were
more similar across subject groups (middle
row) . Estimates of response reproducibility
also were comparable across the two groups,
which is an expected outcome, given the close
relationship between TEOAE/noise and percent reproducibility (Gorga et al, 1993b; Prieve
et al, 1993) . The observation of larger noise
amplitudes in neonates may be due to their
greater breathing noise and their more rapid
breathing pattern . Higher noise levels also
may be a consequence of poorer probe fit in
154
neonatal ear canals, allowing more ambient
room noise to be picked up by the microphone .
Octave Band Analyses of TEOAE
Waveforms
Asomewhat different pattern emerged when
broadband responses were analyzed in octave
bands, which is also shown in Figure 2 . TEOAE
amplitudes in newborns were larger for all bands
but especially for the two octave bands centered
at 2000 and 4000 Hz . While ICN graduates
showed greater background noise for all bands,
noise levels and variability were much greater
in the lower frequency bands (top row) . As a consequence, within the group of older subjects,
TEOAE/noise were larger for the two octave
bands centered at 500 and 1000 Hz . In contrast,
TEOAE/noise were larger for newborns in the
octave bands centered at 2000 and 4000 Hz (middle row) . As expected, a similar pattern was
observed for response reproducibility (bottom
OAEs from ICN Graduates/Berg-man et al
O -
I
Figure 3 Mean 1/3-octave
band TEOAE amplitude (circles), background noise
(squares), TEOAE amplitude/noise (triangles), and percent reproducibility (diamonds) as a function of frequency in both older subjects
(left column) and in neonates
(right column). All amplitudes
are equivalent dB SPL in a
bandwidth of 10 kHz.
TEOAE Level
s
0
f
-30
a -
30
TEOAE/wee
J
IS
. i.a- . .L
0
-1s
-30
too
60
so
.0
O
<r
20
0
0 -
K -20
I Rpreducibility
0
-40
-60
Older Children & Adults
S00
1000
2000
ICN Graduates
4000
S00
1000
2000
4000
Frequency (Hz)
row), although the high-frequency effects are
not as clear due to ceiling effects on this response
measure. That is, differences in response reproducibility decrease as the signal-to-noise ratio
increases beyond about 10 dB . The variability of
the OAE/noise measures tended to be less in the
low frequencies and greater in the high frequencies because the low-frequency measures
were dominated by the noise.
'/s-Octave Band Analyses of TEOAE
Waveforms
As might be expected, a virtually identical
pattern was observed when the broadband
responses were analyzed in Y3-octave bands, which
is shown in Figure 3. TEOAE amplitude and
background noise overlap in newborns for low-frequency regions, whereas some separation exists
in the data from older subjects (top row) . As a
result, positive TEOAE/noise are observed for
lower frequencies in older subjects but not in
infants (middle row) . However, greater separation
in neonates clearly exists between TEOAE amplitude and the background noise for higher frequencies, resulting in larger high-frequency
TEOAE/noise for this group. These patterns are
reflected in estimates of response reproducibility
(bottom row), although perhaps less clearly due
to the previously described ceiling effects.
Journal of the American Academy of Audiology/Volume 6, Number 2, March 1995
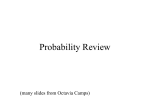
Figure 4 Means (+ 1 standard deviation) for DPOAE
amplitude, noise amplitude
(top row), DPOAE/noise (middle row), and derived correlation (bottom row) as a function of f2 frequency. Data for
older subjects are shown in
the left column while data
from neonates are shown in
OLDER CHILDREN & ADULTS
0
-00
I {{1iI°I °'` e
o - rb» .
o - OPO~E
the right column .
1.1111111
f
a- OPDX/N .i..
-30
too
I
so
a
11
..
.I
f0
K p
L
m
1
I
p
0
0 -20
-~0
0 - D.riv .d r (2)
-i0
Soo
tow
x000
4000
11000
7w
t000
.Ow
.ON
Im
Frequency (Hz)
DPOAE Measurements
Figure 4 shows means (±- 1 standard deviation) for DPOAE and noise amplitudes (top
row), DPOAE/noise (middle row), and derived
correlation (bottom row) as a function of f2 frequency. Data for older subjects are shown in
the left column while data from neonates are
shown in the right column . Using the present
paradigm for measuring DPOAEs, it is not possible to obtain a direct cross-correlation comparable to that used with TEOAEs . However, it
is possible to derive a correlation from signal-tonoise ratios using the following formula:
r = (S - 1)/(S + 1)
where S is defined as the ratio of DPOAE energy
to noise energy (Mills, 1924). The mathematical
relation between signal-to-noise ratios and con
156
relations (Mills, 1924) and its application to
OAE data (Gorga et al, 1993b) has been described
elsewhere. This equation was used to estimate
a derived correlation for DPOAE measurements
following one additional consideration. The present paradigm estimates the amplitude of the
DPOAE at the 2f1 f2 frequency but estimates
noise from the average amplitude of six points
adjacent to 2f,42 (three above and three below),
each spaced by 48 .8 Hz . If the amplitude at any
of the six points is greater than the amplitude
at 2f1-f2, negative DPOAE/noise may be
observed . Obviously, there is no response under
these conditions . However, if these values are
used to calculate a derived correlation, large
negative correlations will be observed . To avoid
this problem, values of 0 dB were assigned to all
conditions when the DPOAE/noise was less than
0 dB, resulting in a derived correlation of 0 for
these conditions . This rule was used both for ICN
graduates and for older subjects . Mean derived
OAEs from ICN GraduatesBergman et al
Octave TEOAE
E.
0
0
0
..e...'~ n
Qan .
'
00
Figure 5
DPOAE
1/3 octave TEOAE
.. .
too " ".
0200. .0-0o:&seo :o
0 - ICN craWora.
0 - oldw CNdrw A A".
i
".. .___ ta.
"
s. . .
a ._._ .
sr "f.
Q`law.
CPua °au. .Wa
QO. .a ."
`
bt] D : Q
~ . . :e
" - Oldw CNdrm & Ad&@
b
so
a . . .. : : ;;...
a'
1s
0
:: : .. . e
a:
n a°
6 . ..
e.a.ea
e
The means from
Figures 2, 3, and 4 are superimposed without error bars .
Data from older subjects are
shown as open symbols while
data from ICN graduates are
displayed with corresponding
filled symbols. TEOAEs, analyzed into octave bands, are
shown in the left column,
along with the results of the
broadband response analyses .
These same data, analyzed
into 1/3-octave bands, are
shown in the middle column.
For TEOAEs, all amplitudes
are equivalent dB SPL in a
bandwidth of 10 kHz . The
DPOAE data are shown in the
right column.
a - ICN crosxeta.
e - Ok1w artrw A Adu1M
00
0
00
Gradvotes
"0" -- ICN
o1a.r CMdrw s Adult.
s00
1000
:000
.000
0
"""
es
s00
0.9
.
"
1000 2000 .000
Froqu.ncy (1s)
0,
a~ "
0
s00
correlations, using the above rules, are given in
the bottom row of Figure 4.
As with TEOAE measurements, both
DPOAE amplitude and background noise tend to
be larger in newborns compared to older normalhearing subjects, but the DPOAE/noise are much
more comparable . Also, the DPOAE/noise measures show less variability in the low frequencies.
The effect of frequency on mean responses,
although present, is less obvious in these measurements compared to TEOAE measurements .
Comparisons across OAE Measures
All of the above observations are summarized in Figure 5, where the means from Figures
2, 3, and 4 are superimposed without error bars .
Data from older subjects are shown as open
symbols while data from ICN graduates are displayed with corresponding filled symbols.
TEOAEs, analyzed into octave bands, are shown
in the left column, along with the results of the
broadband response analyses . These same data,
1000
2000
.000
x000
analyzed into 1/3-octave bands, are shown in the
middle column . The DPOAE data are shown in
the right column .
First, let us consider the TEOAE data . Both
TEOAE amplitude (top row) and the background
noise (second row) are greater in newborns .
However, the separation between these two measures is more similar across groups, resulting in
virtually identical TEOAE/noise for broadband
conditions ("BB", third row, left column). In contrast, both octave and 1/3-octave band analyses
showed poorer signal-to-noise ratios for neonates
in lower frequencies and larger ratios for higher
frequencies (third row, left and middle columns).
Broadband analyses tended to obscure the fact
that neonates have larger TEOAE/noise in
higher frequencies but lower TEOAE/noise for
low-frequency conditions .
Some of these effects are undoubtedly a consequence of the higher noise levels in neonates,
which has its greatest energy in the lower frequencies . It is possible that including a greater
number of samples in each averaged response
157
Journal of the American Academy of Audiology/ Volume 6, Number 2, March 1995
would reduce the noise floor sufficiently to result
in more clearly observed low-frequency TEOAEs .
One other possible explanation for these
frequency effects is the fact that stimulus amplitudes were greater in the ears of older subjects
in the low and mid frequencies compared to the
amplitude achieved in infant ear canals (see
Fig. 1) . These greater amplitudes might have
elicited stronger responses in the ears of older
subjects . However, in no circumstance was
TEOAE amplitude greater in older subjects than
in infants . Differences in these responses were
more a function of differences in the level of
background noise . Additionally, a relation
between stimulus amplitude and response
should be observed if stimulus amplitude is the
source of these differences . However, correlations between TEOAE and stimulus amplitude
within each of four octave bands for infants
were not apparent . The strongest correlation
between response and stimulus amplitude (r =
.25) was observed at 500 Hz, which is the frequency at which a particularly poor signal-tonoise ratio was observed . At the three higher
octave frequencies, the correlations were less and
sometimes even negative . Although the range of
stimulus amplitudes was not large, these data
suggest that the present response differences are
not the result of differences in stimulus amplitude . There is little doubt, however, that stimulus and response amplitudes are related (Stover
and Norton, 1992). It is possible that the stimulus conditions used in the present study were
on the asymptotic, saturated portion of the
input/output function relating OAE amplitude
to stimulus amplitude. Had a wider (lower)
range of stimulus amplitudes been used, the
influence of stimulus amplitude would have
been observed .
The above arguments are based on the
premise that the response spectrum, measured
in the ear canal, reflects the stimulus spectrum
that reaches the cochlea. It is important to
remember, however, that the measured OAE is
influenced by both forward and reverse transmission characteristics. In a sense, the stimulus spectrum in the ear canal can be viewed as
an estimate ofthe energy provided to the cochlea.
Although direct estimates of reverse transmission (i .e ., from the cochlea to the external ear)
are not available, modelling data have been
used to suggest that the spectral shaping of
broadband TEOAEs may be a consequence of the
reverse transfer of energy (Kemp, 1980 ; Kemp
et al, 1986). Thus, it is possible that both the
energy provided to the cochlea (the forward
158
transmission as estimated by the stimulus spectrum in the ear canal) and the reverse transmission serve to attenuate low-frequency energy
in neonatal ears .
A slightly different picture emerged when
DPOAE measurements from these two subject
groups were overlapped, which is shown in the
right column of Figure 5. DPOAE/noise data
from normal-hearing older subjects and from
presumably normal-hearing newborns are similar across a wide range of frequencies (third
row), whereas TEOAE measurements revealed
more obvious frequency-dependent effects.
Cumulative Distributions
Cumulative distributions may have some
advantage over summary statistics, such as
means and standard deviations . While means
and standard deviations can be used to estimate
any percentile, this holds only when the data on
which these estimates are based are normally
distributed. This is unlikely to be the case for
OAE measurements, where both ceiling and
floor effects potentially will skew the distributions for both normal-hearing and hearingimpaired ears . No such assumptions are necessary when cumulative distributions are used.
Examples of this approach for TEOAE data
are shown in Figure 6. The left and right columns
represent data from older children/adults and
neonates, respectively. The top four rows represent TEOAE data analyzed into octave bands
centered at 500, 1000, 2000, and 4000 Hz, respectively, while the bottom row represents data
analyzed as broadband responses. Within each
panel, solid lines represent cumulative distributions of response amplitude while dashed lines
represent similar data for background noise.
At 500 Hz, there is only slight separation
between response and noise cumulative distributions in older subjects and virtually no separation for the infant responses . At 1000 Hz,
there is greater separation in older subjects,
with less separation between response and noise
cumulative distributions in infants. This trend
reverses at 2000 Hz and especially at 4000 Hz,
where the separation is much greater in the
infant responses. These effects are a direct consequence of the interaction between frequency
and the known behaviors of OAEs in infants
compared to older subjects . Infant responses
tend to be larger but so does the background
noise. However, background noise is dominated by low-frequency energy in both groups of
subjects . When the analysis is restricted to a
OAEs from ICN GraduatesBergman et al
important frequency effects. Thus, a narrowband analysis should allow for a better choice of
pass/fail criteria that accurately discriminate
impaired from normal ears .
INFANTS
OLDER CHILDREN
I
500 Hz
DISCUSSION
he following observations can be made from
T the present study:
1.
>K
d
t
v
E
U
-10
o
to
10
30
.o
-to
o
Amplitude (dB SPL)
to
m
ao
w
Figure 6 Cumulative distributions of response (solid
lines) and noise (dotted lines) amplitudes for older subjects (left column) and neonates (right column). Top row
shows 500-Hz data, with 1000-, 2000-, and 4000-Hz data
in the second, third, and fourth rows, respectively. Broadband response analyses are shown in the bottom row.
frequency region where the noise is low in amplitude for both groups (i .e ., 4000 Hz), then the
larger responses of neonates result in larger
signal-to-noise ratios . The previously described
stimulus differences also may be factors contributing to these effects. Although not identical, the differences between infants and older
subjects are not as obvious for the broadband condition . This occurs because both overall response
and noise amplitudes are greater in infants,
effectively offsetting each other. As noted above,
however, these analyses obscure potentially
TEOAEs and DPOAEs can be measured in
graduates of the ICN with click-evoked'
ABR thresholds of 30 dB nHL or better and
with no evidence of middle-ear dysfunction, as well as in older children and adults
with normal hearing sensitivity and normal
middle-ear function .
2. Both OAE amplitudes and noise amplitudes
are larger in newborns compared to older
normal-hearing subjects, resulting in more
similar OAE/noise for both DPOAE and
TEOAE measures . Reproducibility was also
similar between groups .
3. Subtle frequency differences were noted
when TEOAEs were measured that were
not as obvious in DPOAE measurements .
Whereas TEOAE/noise measures were less
in the low frequencies for newborns,
TEOAE/noise were greater in the high frequencies . These low-frequency decrements
and high-frequency increments were
reduced or absent when DPOAE/noise from
infants were compared to those seen in
older subjects .
4. The slight differences in stimulus amplitudes between newborns and older subjects
alone may not fully account for differences
in response amplitudes .
Our data are most comparable to those
reported by Smurzynski et al (1993) . For example, they evaluated both DPOAEs and TEOAEs
in neonates . They analyzed TEOAEs in frequency
bands, much like the present study. The shape
of their response amplitudes as a function of frequency also was similar to those observed
presently. Direct comparisons of absolute TEOAE
amplitudes, however, are not feasible, due to
possible differences in the reference for dB SPL.
Similarly, direct comparisons of noise amplitudes cannot be made . In contrast, direct comparisons between the two sets of DPOAE data are
possible . Our estimates of DPOAE amplitude
are similar to theirs, including a slight decrease
in amplitude around 3000 Hz (although they
observed a greater reduction in amplitude than
Journal of the American Academy of Audiology/ Volume 6, Number 2, March 1995
was presently observed). The present estimates
of background noise during DPOAE measurements, however, were greater than those observed
by Smurzynski et al . In fact, their estimates of
background noise are more similar to those we
observed in older normal-hearing subjects .
The reasons for some of these observations
may be related to differences between studies in
the criteria that were used for including data
from individual subjects in the analyses .
Smurzynski et al did not include data that were
characterized by high levels of background noise,
whereas we included data from all subjects
regardless of noise levels . Our reasons for including the data from every baby who presumably
had normal hearing (i .e ., passed an ABR test)
reflects our interest in understanding how OAEs
perform as a clinical test. Whether an infant fails
an OAE test because of cochlear hearing loss,
background noise, or even middle-ear dysfunction is perhaps irrelevant in terms of what happens next . That infant must either receive a
repeat OAE test or move to the next level of
care . One must include data from all babies
(regardless of the reasons for a failure) if the
goals of the program are to develop a screening
paradigm that is universally applicable .
It is important to consider some of the frequency effects observed in the present study in
relation to the clinical application of OAEs .
Depending upon the stimulus paradigm, both
TEOAEs and DPOAEs can be measured very
rapidly and thus may be well suited as efficient
screening measures for perinatal hearing loss .
The vast majority of educationally significant
sensorineural hearing loss involves at least the
higher frequencies . Low-frequency sensorineural
hearing loss in the presence of normal high-frequency hearing is much less common . Rehabilitative options, including the use of personal
amplification, are greater for hearing losses
involving higher frequencies. Indeed, it is less
likely that any intervention will occur in the
perinatal period, even if low-frequency hearing
loss was identified and quantified, as long as
normal hearing was present in the mid to high
frequencies.
Given these facts, the observation that OAEs
in neonates are more easily measured in the
higher frequencies but difficult to measure at
lower frequencies may have little negative clinical consequence . Whatever the reasons for
poorer OAE/noise in the low-frequency responses
of neonates (i .e ., reduced stimulus amplitudes
due to leakage or ear canal resonances, greater
ambient noise due to poor fit or greater breath160
ing noise), the present data suggest that OAEs
may provide useful information for the frequency
region over which such information may be of the
greatest clinical importance .
Regardless of the frequency region(s) for
which predictions about auditory status are to
be made, cumulative distributions of response
properties perhaps provide the most straightforward approach to selecting pass/fail criteria .
Distributions of response properties from normal
ears would allow selection of response criteria
to achieve any desired false-alarm (false positive)
rate . In a patient population where the incidence of hearing loss is very low (i .e ., the wellbaby nursery), the cost of the test may be driven by the false-alarm rate . Under these circumstances, it might be acceptable, at least to
a first approximation, to develop test criteria
based solely on data from normal-hearing
infants. Cumulative distributions from impaired
ears (not presently available) would allow the
selection of response criteria resulting in any hit
(true positive) rate . Selection of test criteria
probably should be driven more by this information if the patient population was more likely
to include patients with hearing loss, such as
those being evaluated through hearing clinics
and/or otolaryngology departments. In the
absence of data from hearing-impaired infants,
we have not specified optimal response criteria ;
however, the data presented here suggest that
best OAE test performance will occur for mid to
high frequencies, much like ABR test performance .
Thus, cumulative distributions of response
properties for normal and impaired ears allow one
to select criteria resulting in any combination of
both hit and false-alarm rates over the range of
levels of performances for a particular test. This
approach has been applied to data from older subjects (see, for example, Fig. 5 from Gorga et al,
1993a and Fig. 6 from Prieve et al, 1993). Unfortunately, these previous data may be of limited
applicability with neonates because their
response properties apparently differ from those
of older subjects . Thus, the present data can be
used to tell only one part of the story. Similar
cumulative distributions from infants with hearing loss are needed in order to fully describe
OAE test performance in a neonatal population.
It is important to recognize some additional
limitations of the present set of data . First, no
special efforts were undertaken to improve signal-to-noise ratios, such as increasing the number of averages or restricting the analyses to
more favorable frequency regions. For DPOAEs,
OAEs from ICN GraduatesBergman et al
data were collected without the use of an artifact rejection system . Improved signal-to-noise
ratios most likely would have been observed
had such a system been used . A system that
incorporates measurement-based stopping rules
might also result in more efficient data collection and perhaps extend the range of frequencies over which reliable data can be measured
without unacceptable increases in test time .
Another possible limitation of these data is
related to the fact that middle-ear dysfunction cannot easily be objectively measured in
neonates . Although a sizable conductive hearing
loss would be ruled out by ABR thresholds of 30
dB nHL and normal wave I latencies for highlevel stimuli, a slight conductive component
could potentially be present. Trine et al (1993)
demonstrated that negative middle-ear pressure affected the amplitude, reproducibility, and
spectral content of TEOAEs . Indeed, since the
amplitude of OAEs is typically 10 dB SPL or less,
an air-bone gap of 15 to 20 dB is likely to provide sufficient attenuation to reduce or eliminate
the OAE.
Most importantly, data are needed from
hearing-impaired infants. As stated above, a
description of OAE behaviors in infants with
normal hearing provides only a portion of the
information that is needed in order to determine the ability of these measures to identify
hearing loss . Data are needed from infants with
hearing impairment in order to describe the
distributions of responses from both normal and
impaired ears and to determine the extent to
which data from an individual baby can be correctly assigned to one of these groups . Hopefully,
ongoing research efforts will provide these data,
thus providing a more quantitative appraisal of
OAE test performance as a screening measure
for perinatal hearing loss .
Acknowledgments. This work was supported in part by
NIH grants DC00982 and DC01958. We would like to
thank Linda Mace for her help in the preparation of the
manuscript and its accompanying figures. We also thank
Drs. Lisa Stover and Edward Walsh for their comments
on an earlier version of this paper as part of our internal review process.
REFERENCES
Bonfils P, Avan P, Francois M, Trotoux J, Narcy P. (1992) .
Distortion-product otoacoustic emissions in neonates :
normative data . Acta Otolaryngol (Stockh) 112 :739-744 .
Bray P, Kemp DT. (1987) . An advanced cochlear echo
technique suitable for infant screening . Br J Audiol
21 :191-204 .
Ellsmann SF, Matkin ND, Sabo MP. (1987) . Early identification of congenital sensorineural hearing impairment .
Hear J 9 :13-17 .
Gorga MP, Neely ST, Bergman BM, Beauchaine KL,
Kaminski JK, Peters J, Jesteadt W. (1993a). Otoacoustic
emissions from normal-hearing and hearing-impaired
subjects : distortion product responses . JAcoust Soc Am
93 :2050-2060 .
Gorga MP, Neely ST, Bergman BM, Beauchaine KL,
Kaminski JK, Peters J, Schulte L, Jesteadt W (1993b).
Acomparison of transient-evoked and distortion-product
otoacoustic emissions in normal-hearing and hearingimpaired subjects . JAcoust Soc Am 94 :2639-2648 .
Johnsen NJ, Bagi P, Elberling C . (1983) . Evoked acoustic
emissions from the human ear. III . Final results in 100
neonates . Scand Audiol 12 :17-24 .
Kemp DT . (1978) . Stimulated acoustic emissions from
within the human auditory system . J Acoust Soc Am
64 :1386-1391 .
Kemp DT. (1980) . Towards a model for the origin of
cochlear echoes . Hear Res 2 :533-548.
Kemp DT, Bray P, Alexander L, Brown AM . (1986) .
Acoustic emission cochleography - practical aspects.
Scand Audiol Suppl 25 :71-83 .
Kemp DT, Ryan S. (1991). Otoacoustic emission tests in
neonatal screening programmes. Acta Otolaryngol Suppl
(Stockh) 482 :73-84 .
Kok MR, van Zanten GA, Brocaar MP. (1992) . Growth of
evoked otoacoustic emissions during the first days postpartum - a preliminary report . Audiology 31 :140-149 .
Lafreniere D, Jung MD, Smurzynski J, Leonard G, Kim
DO, Sasek J. (1991) . Distortion-product and click-evoked
otoacoustic emissions in healthy newborns . Arch Otol
Head Neck Surg 117:1382-1389 .
Lasky R, Perlman J, Hecox K. (1992) . Distortion-product
otoacoustic emissions in human newborns and adults .
Ear Hear 13 :430-441 .
Mills FC . (1924) . Statistical Methods. New York : Henry
Holt .
Norton SJ, Widen JE . (1990) . Evoked otoacoustic emissions in normal-hearing infants and children : emerging
data and issues . Ear Hear 11 :121-127 .
American National Standards Institute. (1989) .
Specifications forAudiometers . (ANSI S3 .6-1969, R 1973)
New York : ANSI.
Prieve BA, Gorga MP, Schmidt AR, Neely ST, Peters J,
Schulte L, Jesteadt W. (1993) . Analysis of transientevoked otoacoustic emissions in normal-hearing and
hearing-impaired ears . JAcoust Soc Am 93 :3308-3319 .
Allen JB . (1990). User Manual for the CUBDIS Distortion
Product Measurement System . Unpublished manual .
Smurzynski J, Jung MD, Lafreniere D, Kim DO, Kamath
MV, Rowe JC, Holman MC, Leonard G. (1993). Distortion-
161
Journal of the American Academy of Audiology/ Volume 6, Number 2, March 1995
product and click-evoked otoacoustic emissions of preterm
and full-term infants. Ear Hear 14 :258-274.
Smurzynski J, Kim DO . (1992) . Distortion-product and
click-evoked otoacoustic emissions of normally-hearing
adults . Hear Res 58 :227-240 .
Stevens JC, Webb HD, Hutchinson J, Connell J, Smith
MF, Buffin JT. (1991) . Evaluation of click-evoked otoacoustic emission in the newborn . Br JAudiol 25 :11-14.
Stover LJ, Norton SJ . (1992) . Comparisons among different otoacoustic emission types . Abstracts, Ass Res
Otolaryngol 15 :153.
Trine MB, Hirsch JE, Margolis RH . (1993) . The effect of
middle ear pressure on transient evoked otoacoustic emissions . Ear Hear 14 :401-407 .
Uziel A, Piron J. (1991) . Evoked otoacoustic emissions
from normal newborns and babies admitted to an intensive care baby unit . Acta Otolaryngol Suppl (Stockh)
482:85-91 .
White KR, Vohr BR, Behrens TR . (1993) . Universal newborn hearing screening using transient evoked otoacoustic
emissions: results of the Rhode Island hearing assessment project. Semin Hear 14 :18-29 .