Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
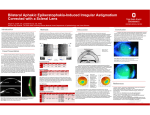
9/24/2014 That’s a BIG lens!! Scleral Contact Lenses MOA Convention 10.4.2014 Chris DeRose, OD Size matters Average Corneal diameter = 11.5mm Average RGP lens = 9.5 mm Soft Contact lens = 14.0 to 14.5mm Mini‐scleral lens = 15.0 to 18.0mm Scleral lens = 18.0 to 24.0mm RGP Soft Contact Lens 1 9/24/2014 Scleral Lens What makes Sclerals different? Rest on the sclera (don’t touch the cornea) Vault over the cornea Tear Reservoir between the contact lens and the eye Insertion and removal process So What? Who is a good patient for scleral lenses? Corneal irregularity Corneal scarring or post trauma Keratoconus S/P refractive surgery Advanced dry eye or incomplete lid closure (exposure) S/P Corneal transplant Extreme astigmatism Cosmetic (albinism, trauma, aniridia) Resurgence Advantages No corneal touch = no chance of worsening scar progression No corneal contact and less movement = less awareness (kinda) Tear reservoir can be therapeutic Better VA (sometimes dramatic) Easier to compensate for crazy corneal shapes Messed Up Corneas Increased O2 permeability of new lens materials New digital manufacturing processes 2 9/24/2014 Vault Can we fix this cornea with scleral lens? Corneal Topography (normal) Corneal Topography (astigmatism) Corneal Topography (Keratoconus) 3 9/24/2014 Corneal Topography (?) Fitting Fitting Must be fit diagnostically Alignment with sclera No bearing on limbus Based on sagittal height Little to no movement Must settle for 30 minutes No conjunctival impingement Spherical over‐refraction Vault Reduction Therapeutic Sclerals Tear Reservoir promotes healing in Ocular Surface Disease Sjogren’s Stevens Johnson Syndrome Graft vs Host Ocular cicatricial pemphigoid Neurotrophic corneal disease Exophthalmos Ectropion Eyelid Coloboma Start Steep Minimal Vault Touch 4 9/24/2014 Insertion and Removal Insertion and Removal Insertion and Removal Insertion and Removal Fill the lens with non‐preserved saline Place lens on formed "tripod" (thumb, index, and middle finger) or use scleral cup Position face parallel to a horizontal plane, typically the table/mirror and open eyelids wide using opposite hand. Insert lens edge into lower cul‐de‐sac while pushing the lens onto cornea Must break the negative pressure underneath the lens Manual method – Using fingers, guide eyelid margin under the bottom edge of the lens. This will break suction and allow lens to come out Plunger method – Place the plunger on bottom portion of lens NEVER place the plunger centrally on lens – may result in corneal damage Insertion and Removal Use anesthetic for initial lens dispense Study: Reduces long term drop outs by 75% Patients may be intimidated by size of lens and handling – Doc presentation is the key 5 9/24/2014 Complications Complications Complications Contact Lens Optics Sagittal height Increased sagittal height steepens corneal‐lens fit Systemic Conditions that Affect CLs Cosmetic Sclerals Diabetes Collagen Vascular Disorders Pregnancy Birth Control Thyroid Eye Disease Allergy Anti‐histamine use 6 9/24/2014 Cosmetic Sclerals Hollywood Sclerals Hollywood Sclerals Why fit scleral lenses? Differentiate your practice Incredibly grateful patients = more referrals Full scope of professional practice More referrals from Ophthalmology/cornea Case Case Patient AW ‐ 55 year old Male + Severe Keratoconus OD > OS Has been wearing Rose K lenses OU for many years Lenses have begun to spontaneously eject VA cCLs: OD 20/40‐ OS 20/40 BVA with specs: 20/400 OD, OS 7 9/24/2014 Case Slit lamp: Case Refit to scleral lens – diameter 18.0 mm Central corneal scarring OD > OS Significant apical thinning OU 2‐3+ central SPK OU Refit to SynergEyes Ultrahealth hybrid CL Poor comfort and limited wear time Significant protein build‐up on lenses Case BVA cCL: OD 20/30 OS 20/30+ 16 hours of comfortable wearing time No corneal contact on central scarring References ES, Barr JT, Szczotka‐Flynn LB. Keratoconus. In: Clinical Manual of Contact Lenses. Bennett and Henry, Wolters Kluwer, 4th ed. 2014; Chapter 1: 518–577. DeNaeyer G, Breece R. Fitting techniques for a scleral lens design. Contact Lens Spectrum. 2009; 1: 34–37. DeNaeyer G. Scleral contact lens fitting. Contact Lens Spectrum. 2010; 6: 20–25. DeNaeyer G, Jedlicka J, Schornack MM. Scleral Lenses. In: Clinical Manual of Contact Lenses. Bennett and Henry, Wolters Kluwer, 4th ed. 2014; Chapter 21: 609‐647. Eggink FAGJ, Nuijts RMMA. Revival of the scleral contact lens. Cataract & Refractive Surgery Today Europe. 2007; 9: 56–7 Jacobs DS. Update on scleral lenses. Current Opinion in Ophthalmology. 2008; 19: 298–301 Kalwerisky K, Davies B, Mihora L, et al. Boston Ocular Surface Prosthesis in the management in severe periorbital thermal injuries: a case series of 10 patients. Ophthalmology. 2012; 119: 516‐521. 8