Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
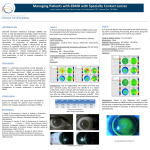
Bilateral Aphakic Epikeratophakia-Induced Irregular Astigmatism Corrected with a Scleral Lens Abigail G. Graeff, OD, Chantelle Mundy, OD, FAAO Havener Eye Institute, The Ohio State University Wexner Medical Center Department of Ophthalmology and Visual Science Introduction Epikeratophakia onlay procedures were first introduced by Werblin in 1979 and further developed by Kaufman and McDonald in 1980.1 This procedure involves donor corneal tissue lathed into a lamellar disk and surgically transplanted onto the anterior surface of the host cornea and stabilized via a small incisional “pocket” in the host tissue periphery. Indications for this surgery included pediatric or adult aphakia, hyperopia, myopia, and keratoconus. There were many advantages to this procedure, including potential reversibility, minimal invasion, and preservation of posterior layers of the host cornea.2 This procedure was particularly useful in the pediatric aphakic population as it is indicated for aphakic patients with contact lens intolerance, unilateral cataracts, and trauma induced cataracts with anterior segment damage contraindicating an intraocular (IOL) lens implantation.2 Epikeratophakia demonstrated a favorable success rate and impressive stability over long-term follow-up care. However, complications included myopic shifts and graft-host interface edema and scarring. Methods Conclusion Discussion A diagnostic contact lens fitting was conducted in both eyes. Prognosis with contact lenses was guarded the patient had a history of contact lens intolerance due to discomfort. Because of this, scleral lenses were used for the diagnostic fitting (Europa scleral, Visionary Optics). Corneal topography and Endothelial Cell Counts were taken in both eyes (Pentacam, Oculus and CellChek Specular Microscope, Konan Medical). Pachymetry was 976 microns in the right eye and 978 in the left eye. Available literature concerning the success of scleral lens wear and epikeratophakic corneal onlay procedures is limited. However, quantifying endothelial cell counts can signify corneal pump integrity and therefore potential risk for corneal edema. Low endothelial cell counts, usually counts less than 600-700 mm2, could result in corneal edema as the increased corneal thickness increases stress on endothelial cells rendering them incapable of maintaining corneal deterguescence. In a study of average endothelial cell counts pre- and 16 months post-epikeratophakia surgery, the average endothelial cell count pre surgery was 1450 per mm2 (+/- 218) and 1438 per mm2 (+/- 218) 16 months post-surgery. Both endothelial cell counts were low, but did not vary significantly after surgery, thus concluding that epikeratophakia is well tolerated by the cornea and can be performed safely without substantial trauma to the host endothelium.3 Because of this, scleral lenses are not contraindicated in epikeratophakic patients. Figure 4 (Left): The anatomy of a postepikeratophakic eye 4 Case Presentation A 49 year old white female, referred by her glaucoma specialist for a cornea and contact lens evaluation, presented to our OSU clinic with a chief complaint of blurred vision with her current glasses. She was born with congenital cataracts and underwent bilateral cataract surgery as a child and as a result, was aphakic. She then had an epikeratophakia onlay procedure at age 20 to treat her pediatric aphakia. She was also diagnosed at age 10 with Type 1 Diabetes Mellitus. She is currently using an insulin pump, notes stable blood sugar readings, and average HbA1c readings of 6.8mg/dl. She is being treated for Ocular Hypertension of both eyes with Cosopt BID OU. She is also taking Fluorometholone 0.1% BID OU. Upon slit lamp examination, external examination was normal for both eyes. There was a slight anisocoria with the right pupil displaced nasally. During the corneal examination, epikeratoplasty lenticules were noted in both eyes. No corneal edema was noted and the interface between the donor lenticule and the host corneal tissue was clear with no scarring or deposits noted. No NVI noted in both eyes. Both eyes were aphakic. Goldmann applanation IOP was 23 mmHg in the right eye and 25 mmHg in the left eye. Upon DFE, C/D ratios were 0.2 in both eyes. No NVD or NVE or CSDME was noted in either eye. Figure 7 (Above): This is the right eye with the 16.0 mm final scleral lens in place demonstrating uniform vault. Notice a slight nasally displaced pupil. Figure 8 (Below): This is the left eye with the 16.0 mm final scleral lens in place demonstrating uniform vault and no edge blanching. Current Spectacle Rx: Sphere Cylinder Axis ADD Distance VA PH VA OD +6.50 -3.50 096 +2.50 20/300 20/100 OS +5.75 -1.75 141 +2.50 20/150 20/70 There are several complications associated with epikeratophakia procedures. Complications can be graft-centric, including failure of graft tissue to reepithelialize, graft haze, infection, deposits and vascularization of the graft tissue.5 However, complications can also be associated with refractive changes or visual compromise. These complications include induced irregular astigmatism, reduced contrast sensitivity, and progressive myopic shifts (Kang). Because of these complications, treating pediatric aphakes with epikeratophakic onlay procedures has been replaced by refractive surgery and IOL implantation. Scleral Lens fitting: OD OS Brand Visionary Optics, Europa Scleral BC 7.181 Diameter 16.0 Power +7.50 PC Standard VA 20/25 Visionary Optics, Europa Scleral 6.888 16.0 +7.25 Standard 20/25 Upon follow-up visit, she notes good comfort and vision and is able to wear lenses for 12 hours per day. Upon over-refraction, a small amount of residual astigmatism remained and prescribed along with a bifocal as a pair of glasses to wear over the contacts. After settling time, there was slight corneal touch on the right eye, therefore it was steepened by 2.00 D. Over-Refraction: Sphere Cylinder Axis ADD Distance VA OD +0.50 -0.75 088 +2.50 20/25-2 OS +1.25 -0.50 085 +2.50 20/25+2 Final Scleral Lens Prescription: OD Figure 1 (Top): Scheimpflug image of right eye using the Pentacam corneal topographer. The interface between the host cornea and epikeratophakic lenticule is visible. Also visible is a deep anterior chamber and aphakia. Figure 2 (Bottom): Sheimpflug image of left eye using the Pentacam corneal topographer. Figure 3: (Right): Slit lamp optic section of diagnostic scleral lens . In patients with pediatric aphakia treated with epikeratophakia, long-term success of the procedure has been documented for upwards of 20 to 30 years post-surgery. In patients with refractive error shifts or induced irregular astigmatism from epikeratophakic lenticules, rigid gas permeable lenses have proven a successful treatment option in both comfort and visual acuity improvements. As little is known concerning scleral lens wear and epikeratophakia, more research is needed in order to fully understand prognostic success with lens wear. OS Brand BC OZD Visionary Optics, Europa Scleral Visionary Optics, Europa Scleral 6.89 8.5mm 16.0 mm Diameter Power Peripheral Curves CT +6.50 6.89 8.5mm 16.0 mm +7.25 PC1: PC2: PC3: PC4: PC1: PC2: PC3: PC4: 6.780/2.10 9.00/0.75 13.00/0.50 14.50/0.40 6.806/2.10 9.250/0.75 13.250/0.50 14.50/0.40 Material Vault 0.64 Boston XO 300 microns 0.64 Boston XO 300 microns Figure 6 (Left): Axial/Sagittal Curvature (Front Surface) map of Right eye using the Pentacam Corneal Topographer. This map is consistent for irregular astigmatism. Figure 7 (Right): Axial/Sagittal Curvature (Front Surface) map of Left eye using the Pentacam Corneal Topographer. This map is consistent for irregular astigmatism. As irregular astigmatism is poorly treated with spectacle lenses, rigid gas permeable contact lenses are an effective treatment in improving both visual acuity and perceived visual quality. Scleral lenses, particularly, are successful in patients with irregular astigmatism as they have improved comfort over smaller diameter rigid gas permeable contact lenses. Scleral lenses must be carefully monitored when first dispensed as corneal edema may result in situations such as contact lens overwear, corneal hypoxic events, or a tight fitting lens. In patients with epikeratophakia, increased corneal thickness combined with below average endothelial cell counts predisposes them to corneal edema. References 1. Rostron, Chad K. Introduction to epikeratophakia. Laser and conventional refractive surgery. Chapter 8, 1996. Pages 157-209. 2. Kang, Julia, Florence Cabot, and Sonia H. Yoo. "Long-term follow-up of epikeratophakia." Journal of Cataract & Refractive Surgery. Volume 41.3 (2015): 670-673. 3. Guss, R. B., et al. "Endothelial cell counts after epikeratophakia surgery."Annals of ophthalmology. Volume15.5 (1983): 408-409. 4. Morgan, Keith S. “Optical Rehabilitation of Aphakia with Epikeratophakia”. Duane’s Ophthalmology (2006). Chapter 103. http://www.oculist.net/downaton502/prof/ebook/duanes/pages/v6/v6c103.html 5. Greenbaum, Aaron, Igor Kaiserman, and Isaac Avni. "Long-term reversibility of epikeratophakia." Cornea. Volume 26.10 (2007): 1210-1212.