Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
UNFPA - Sudan
An Update of Reproductive Health, Gender, Population
and Development Situation in Sudan, 2011
by
Dr. Samia Elnagar – Gender Specialist and Team
Leader
Dr. Hassan Abdel Ati – Population Development
Specialist
Dr. Lamia Eltigani – RH Specialist
Dr. Huda Mohamed Mukhtar - Demographer
December, 2011
1
TABLE OF CONTENTS
SECTION
PAGE
Table of Abbreviations
3
List of Tables
5
List of Figures
7
Executive Summary
9
1.
Objectives & Principles of the Situation Analysis
13
2
Overview: Economic, Socio-cultural, Political and
Institutional Context
16
2.2 Progress in complying with MDGs and ICPD Goals
30
3
TOPIC
Population, RH and Gender Dynamics
3.1 Population Dynamics
35
3.2 Reproductive Health and HIV/AIDS Dynamics
66
3.3 Gender Dynamics
89
3.4 Youth and Adolescents
110
4
Priorities for Strategic Intervention
122
5
References
129
2
LIST OF ABBREVIATIONS
ABBREVIATION
ANC
ART
BSc
CAAF
CBOs
CEDAW
CPA
CRC
CSOs
CMR
EFA
EmONC
EXCs
FMoE
FMoH
FMoWSS
FSWs
FP
GBV
GDP
GDoWFA
GM
HAI
HIV/AIDS
ICPD
IDPs
ILO
IPRSP
MARPS
MDGs
MMR
MSM
MPS
MVA
NA
NGOs
NRHP
PAC
MEANING
Antenatal Care
Antiretroviral Therapy
Bachelor of Science
Children Associated with Armed Forces
Community Based Organizations
Convention for Elimination of All Discrimination
Against Women
Comprehensive Peace Agreement
Convention for Children Rights
Civil Society Organizations
Clinical Management of Rape
Education For All
Emergency Obstetric and Neonatal Care
Ex- combatants
Federal Ministry of General Education
Federal Ministry of Health
Federal Ministry of Welfare and Social Security
Female Sex Workers
Family Planning
Gender Based violence
Gross Development Product
General Directorate of Women and Family Affairs
Gender Mainstreaming
Health Alliance International
Human Immunodeficiency Virus/
Auto-immunodeficiency Syndrome
International Conference on Population and
Development
Internally Displaced People
International Labor Organization
Interim Poverty-Reduction Strategy Paper
Most At Risk Populations
Millennium Development Goals
Maternal Mortality Ratio
Men Who Have Sex With Men
Making Pregnancy Safer
Manual Vacuum Aspirator
Native Administration
Non- governmental Organizations
National Reproductive Health Programme
Post-abortion Care
3
PHC
PITC
PLHIV
PMTCT
RH
SHHS
SMOH
SMS
SNAP
STIs
TB
TBAs
TFR
UNFPA
UNICEF
VAW
VCT
VMWS
WAAF
WHO
Primary Health Care
Provider Initiated Testing and Counseling
People Living with HIV
Prevention of Mother to Child Transmission
Reproductive Health
Sudan Household Health Survey
State Ministry of Health
Safe Motherhood Survey
Sudan National AIDS Programme
Sexually Transmitted Infections
Tuberculosis
Traditional Birth Attendants
Total Fertility Rate
United Nations Population Fund
United Nations Children's Fund
Violence Against Women
Voluntary Counseling & Testing
Village Midwives
Women Associated with Armed Forces
World Health Organization
4
LIST OF TABLES
NO
TABLE
Table 2.1:
Regional Disparities in Some MDG Indicators
(2009)
Table 2.2:
Sudan HDI 2011
Table 2.3:
Poverty Incidence and Poverty Gap by Region
Table 2.4:
Poverty Incidence, Poverty Gap and Severity
Table 2.5:
Basic Capability Index (BCI)
Table 2.6
MDGs Progress
Table 3.1.1
Percentage distribution of the total area of Sudan
and total population by region
Table 3.1.2
State Population density per square Kilometer,
Republic of Sudan, 2008
Table 3.1.3
Percentage distribution of population by age and
sex, Republic of Sudan, 2008
Table 3.1.4
Percentage distribution of children ever born alive
by ever married women and average number of
children born alive, according to age groups, 2008
census
Table 3.1.5
Infant, child and maternal mortality rates, Crude
death rates and Life expectancy by State, 2008 and
2010
Table 3.1.6
Current In-Migrants, Out-Migrants and Current
Net Streams of Migration and Migration TurnOver, Sudan: 2008 census
Table 3.1.7
Current In-Migrants Out-Migrants and Net
Lifetime Streams of Migration and Migration
Turn-Over by sex, Sudan: 2008 census
Table 3.1.8
Percentage distribution of population by marital
status according to age and sex , 2008 census, and
PAGE
5
percentage never married persons by age and sex,
SMS 1999 and 1993 census, Republic of Sudan
Table 3.1.9:
Percentage distribution of population economically
active an employed by sex, 2008 census
Table 3.2.1.
Health Facilities by Type and Number
Table 3.2.2.
Reproductive Health Indicators, 2006 and 2010
Table 3.3.1
Gender Related Development Index in Sudan
Compared to World Regions, 2006
Table 3.3.2
Percentages of Literate in Population 10 Years and
Over by Sex and Mode of Living, 1993 and 2008
Table 3.3.3
Labor Force Rate of Population Age 10 Years and
Over by Sex and Mode of Living
Table 3.3.4
School enrolment at basic education and secondary
level by sex and mode of living:
Table 3.3.5
Percentage of Respondents Definition of Violence
Against Women Concept, by Sex and Education
Table 3.4.1
Percentage of married among males and females
population by age and mode of living
Table 3.4.2.
Age specific activity rates by mode of living, 2008
Table 3.4.3.
Poverty Aspects of Youth in Kassala
and Gadaref States
Table 3.4.4.
Adolescents’ Reproductive Health, Knowledge and
Practices
Table 3.4.5
A
Youth Reproductive Health Profile from SHHS,
2006(Knowledge Attitude and Behavior)
Table 3.4.5.
B
Youth Reproductive Health Profile from SHHS,
2006(Services Provided)
Table 3.4.6
Views of Youth in Kassala and Gedaref on
Women Rights
6
LIST OF FIGURES
NO
FIGURE
Figure 2.1
Economic Sector Share 04 - 2010
Figure 2.2
Sudan Imports & Exports 2005-2010
Figure 2.3
Sudan Human Development Index 1980 - 2011
Figure 2.4
Population and GDP Growth rates 2004 - 2009
Figure 3.1.1
Population Growth and percent change between
the censuses 1956-2008
Figure 3.1.2
Annual population growth rates 1956-2008
Figure 3.1.3
Population projections 2011-2031
Figure 3.1.4
Population change according to mode of living
1955/56-2008
Figure 3.1.5
Percentage distribution of urban population by
state, Republic of Sudan, 2008
Figure 3.1.6
Crude birth rate 1955/56-2008
Figure 3.1.7
Age specific fertility rates for Republic of Sudan
1993 and 2008
Figure 3.1.8
Trends in total fertility rates in 1973-2010
Figure 3.1.9
Total fertility rates in 2008 by State
Figure 3.1.10
Percentage distribution of either of couples used
FP methods, by State 2010
Figure 3.1.11
Mean number of children born alive according to
the mode of living, by age, Republic of Sudan,
2008
Figure 3.1.12
Mean number of children born alive by education,
Republic of Sudan, 2008
Figure 3.1.13
Life expectancy 1956-2010.
PAGE
7
Figure 3.1.14
Crude death rates 1956-2010
Figure 3.1.15
Maternal mortality rates1989-2010.
Figure 3.1.16
Child and infant mortality rates 1956-2010,
Republic of Sudan
Figure 3.1.17
Percentage of urban population to the total
population 1956-2008
Figure 3.1.18
Distribution of never married women by age,
SDHS1989, 1993 Census, SMS 1999 and 2008
Census.
Figure 3.1.19
Economic activity participation rate in urban, rural
and nomadic areas by age, Republic of Sudan,
2008
Figure 3.2.1
Contraceptive Prevalence Rates by state, 2010
Figure 3.2.2
Health Facilities Providing Testing & Counseling2006-2010
Figure 3.2.3
Numbers of TB Centers and Patients Tested For
HIV 2007-2010
Figure 3.3.1
Percentage of Literate People in Population 6 and
Over by State and Sex and Mode of Living
Figure 3.3.2
Labor force participation rate by states,
NBHS,2009
8
EXECUTIVE SUMMARY
udan is in a critical political, socio-economic and demographic transition, particularly in the
post-cessation era, together with emerging national opportunities and challenges vis-à-vis the
Schanging governance in the Arab region and the internationally down-turning economies.
The newly two established post-cessation countries (Sudan and Southern Sudan) have serious
disputes and a long trail to reach a peaceful coexistence. Although the Government has recently
signed Peace Agreement in Doha with some of the Darfuri rebel movements, brutal fighting is
perpetual in South Kordofan, Blue Nile, and some pockets in Darfur.
Sudan’s external debt was estimated to have reached about US$ 38 billion in 2010 recording a
rise of 85% of its level in 2000. The oil discovery in 1999 has transformed the economy from
food-producing into a mono-product food-importing and service economy with high vulnerability
to international crises. Oil used to contribute over 95% of merchandise exports and about 50% of
government revenues. Due to the country’s cessation, the Sudan has lost 80% of its oil fields, thus
leaving a highly exposed economy that is hardly able to service its debts, attract FDI, and achieve
tangible progress in the MDGs. Shortage in supply of hard currency has left huge budget deficit
and has nearly doubled the US$ exchange rate against the SDG (from almost a stable rate of SDG
2.0 to above 4.0 in the parallel market). The result has been a sharp increase in prices of almost
all the basic consumer goods/services, thus further worsening the already beleaguered living
conditions of the bulk of the population who are classified as poor.
In recent estimates (2009), Sudan has scored medium human development rate (52%) with 17%
of the population live on less than US$ 1.25 per day. Poverty has been formally estimated to have
engulfed about 47% on national average with enormous variations between and within states,
particularly areas with conflict, pastoralists, displaced, poor/primary production, and dependency
on natural resources. While the lowest ratio of population under the poverty line has been
recorded in Khartoum (26%), the highest has been recorded in Darfur Region (average 62.7% North Darfur recorded 69.4%), followed by Kordofan Region (58.7%).
The national poverty map suggests that there are gaps and socio-economic disparities between
states and within the same state at the different locality levels. This situation is increasing the
population dynamics, particularly migration from rural to urban areas, thus further weakening the
productive capacity of the rural economies, deepening poverty in both rural and urban areas, and
widening the regional imbalances with serious implications to national peace and human security.
However, the geographical move has made little change in the life style of most migrants and
IDPs, particularly those who reside in unplanned areas in the fringes of big urban centres.
udan national population census (2008) recorded a net internal migration of about 1.8 million
persons, about 95% of whom were received by Khartoum and the rest (about 100,000) by the
Seastern States of Red Sea and Gedarif. While migration was predominantly rural-urban, it has
recently become urban-urban in direction, not planned/prepared for, prompted by push rather
than pull factors, and no longer young-male-selective but involves families and sometimes whole
communities (e.g. IDPs) and businesses (e.g. from periphery towns to the national capital);
sometimes, migration was even a forced one. These are some of the issues that should factor the
population policies and planning (national and state).
The cessation has left Sudan with 30,894,000 peoples (33% urban and 67% rural, including 9%
nomads) with 2.4% annual growth rate and a broad-based cohort of young population (62% of the
9
country’s population are less than 25 years). While male population below 20-year age bracket
outnumber females, the opposite is true in the age bracket 20-40 years; this skewed population
pyramid may be partially due to males’ outmigration. Since 2004, population has been growing at
a rate less than the annual economic growth (real GDP) by almost 3-folds (1:3). However, the
current population growth together with a high but declining total fertility rate (5.5% in 2008)
means that the Sudan’s population will double every 29 years. Having a largely young and
growing population base is a critical demographic bonus and human capital for economic and
social development in Sudan. What the country needs is investment in young people and rational
population policies to influence the trends in population dynamics, as well as encourage
government spending on social services, especially education and health.
pending on health in general has been identified as a government priority. The government also
committed itself to make reproductive health services available to all citizens through its
SReproductive Health Policy launched in 2010. However, the 2008 national health accounts
revealed that government spending was only 9% of its total public expenditure. It was also
evident that 64% of the spending on health is privately incurred against household budgets, while
the rest is provided for by health insurance schemes and charities.
Low public levels of spending on health in general and on RH in particular indicate that Sudan is
still far from achieving MDG 5 on universal access to RH services and reduction of maternal
mortality. The direct results of low health spending are limited services/facilities, weak health
system, shortage in health personnel, weak logistical management system, and irregular flow of
information to guide planning and policy-making. There are even regional disparities and poor
coverage of the existing RH services, facilities, and personnel particularly in humanitarian
settings, and in the under-served rural areas and the urban peripheries.
The Sudan Household Health Survey II (2010) has revealed some progress but also some lagging
RH indicators. Key indicators were MMR, which stood relatively high at 216 per 100,000 Live
Births (though significantly dropped from 638 in 2006), about 73% of the births attended by a
trained health personnel (out of which 50% assisted by village midwives), only 47% of pregnant
women receive the standard 4 antenatal care visits, only 46% of the health facilities provide
comprehensive EmONC, only 21% of the deliveries were in health facilities, contraceptive
prevalence rate was 9%, and unmet need family planning stood at 29%.
There were many health and social determinants contributing to decelerate progress towards
achieving targets of MDG 5. For example, the post-partum haemorrhage remains the major cause
maternal death (20%), while the obstetric fistula continues to be the major cause for maternal
morbidities. Main barriers to contraceptive relate to attitudes, preference of large family size, lack
of knowledge and religious beliefs. Users of contraceptives are the better educated, wealthier and
urban-based peoples. This means to consider improving accessibility to family planning services
and information (availability and affordability) and raising awareness, particularly in rural
communities.
The RH work should capitalise on the newly endorsed National Road Map for MNMR (20112015), which provides an overall vision of the required interventions, as well as a guide to
harnesses resources into a unified national plan. Strategic priorities addressed in the roadmap
include: (i) gradual phase-out of the 1-year midwifery curriculum towards 2-year midwifery
technician and then B.Sc. midwifery curricula aiming at qualifying midwives to meet the
international standards; (ii) focus on family planning and EmONC; and (iii) integration of early
preparedness and response (including MISP and CMR) into regular programming.
10
udan used to have a generalised HIV/AID epidemic prevalence of 1.6%. Current data on
HIV/AIDS reflects a relatively low epidemic prevalence of 0.67% particularly in the general
Spopulation (15-49 years), but highly concentrated in the MARPs, namely FSW, and MSM.
However, projections are expecting gradual increase in the HIV prevalence to reach 1.12% by
2015. The national vision of a “Sudan free from HIV/AIDS” has positioned HIV/AIDS/STIs
among the top national priorities through the HIV/AIDS Strategic Plan 2010-2014. Many
strategic priorities should include provision of VCT, PMTCT, ART and STIs services and
treatment, community awareness, and strong programme monitoring. Efforts made so far have
increased VCT centres from 34 to 138, PMTCT sites from 8 to 38, and built up expertise in
outreach services to MARPs including VCT, peer-education, condom distribution and research
(mapping and bio-behavioural).
While stigma remains the major obstacle to effective implementation of HIV interventions, public
silence continues to propagate the virus. Major gaps to increase access to HIV/AIDS services
include knowledge, inadequacy of financial resources to implement national commitments, and
presence of two separate national structures for RH and for HIV/AIDS each implementing in
isolation of the other. But there are wide opportunities to future, such as presence of strategic
partnerships and networks across the country.
udan has high illiteracy (48%) particularly among women whose economic participation is still
very low (21%) compared to men (54%). Despite the political and economic rights they have
Sacquired for decades, women are still suffering some gender gaps. Women have limited and
urban-biased political participation, low school attainment especially in rural areas and
disadvantaged states, and the majority engage in unpaid work and in the informal sector activities,
which lack legal protection.
There accumulating efforts between civil society and government to address gender inequalities
and violence against women in Sudan have yielded formulation of policies (e.g. WEP),
establishment of government structures (e.g. Gender, and VAW units), processes/mechanisms to
mainstream gender in planning/budgeting, and supporters within government institutions. Despite
this, challenges include domestic violence, early marriages, FGM, various forms of violence in
humanitarian settings, socio-cultural dictates against women/girls, and how to maintain women
gains so far.
Gender Inequality and Women Empowerment:
Despite that Sudanese women have acquired political and economic rights for decades, and
there is progress in their economic and political participation, still gender gaps persist. This is
indicated by high literacy rate, low school attainment specifically among girls in rural areas and
disadvantaged states, and by engagement of majority of women in unpaid work and in informal
sector activities which are not protected by law. The political participation of women remained
limited in quantity and quality and urban-based.
Violence against women is prevalent; including domestic violence, Female Genital Mutilation
and early marriage. The main success achieved is the break of silence on the violence against
women, as a result of pressure by civil society organizations. In addition, the government
responded by the establishment of Violence against Women Unit. The challenge is how to
arrange for a coordinated and consolidated response.
Women in conflict areas, especially in Darfur, as displaced, have experienced exposure to new
skills and interactions and accessed new services. The challenge is how to maintain these new
11
experiences in resettlement contexts. Some women in internally displaced people camps in
Darfur, have gained recognition for their leadership roles, and have been participating in Native
Administration meetings with Development Partners. However, still male leaders have limited
perception to the leadership capacities of women and the latter are not fully empowered to break
through all barriers.
There have been tremendous efforts for addressing problems of gender inequality by initiating a
gender mainstreaming process in policies and plans at all levels. The result is the establishment
of units and mechanisms for gender mainstreaming, as well as the existence of champions
within government institutions advocating for gender mainstreaming and budgeting. The
process of gender mainstreaming is challenged by limitations of resources.
The prevalence of gender gaps and violence against women are related to the lack of genderresponsive policies, budgets and predominance of male-dominance culture. The strategic
priorities for addressing gender equality, should focus on reduction of early marriage (as
violence against women) and maternal mortality. A focus on rural areas & integrated approach
are essential for sustainable development.
Youth and Adolescents:
Viewing the youth situation from the perspective of human rights and human development is
strategic in supporting youth as potential leaders. With such perspective, it is apparent that the
majority of adolescents and youth in Sudan including the privileged are deprived from basic
human rights; not given a choice in all stages of life.
Education does provide them with skills and knowledge relevant to their life and needs; but
does not help in creating youth with critical mind and independent thinking. Also, many
adolescents, young men and women are forced to drop education for familial economic
conditions, or for lack of needed educational facilities and services. Those who continue do not
choose the type of education, as this again is determined by limiting surrounding conditions.
Most adolescents, young men and women, are forced to marry or are restricted in spouse
selection by families. They are not informed about reproductive rights, and thus cannot claim it.
If young people get married, they have to have children or would be forced to divorce and
remarry.
As most adolescents and youth, particularly in rural and nomadic areas, are not in educational
institutions and not participating in social life, they do not have opportunities for accessing
knowledge, usage of technology, experiencing dialogue or being exposed to other cultures and
life styles. However, those who get higher education may have such opportunities. The
challenge is how to provide such opportunities to the majority outside educational institutions.
Historically, there have been no strategies for social development of adolescents and youth, and
the existing youth institutions are under-resourced, mostly not functional and not accessible to
them, specifically those in rural areas. Thus, most of the youth lack awareness and opportunities
for social participation. Accordingly, the strategic priority actions are to empower adolescents
and youth for improved social participation and civic engagement, for controlling decisions
related to their bodies, reproductive rights and health.
12
SECTION ONE:
OBJECTIVES AND PRINCIPLES OF THE SITUATION ANALYSIS
Sudan is in a historical moment after the separation of South Sudan, the signature of a new
peace agreement with some rebel groups from Darfur, and the resumption of conflicts in South
Kordofan and Blue Nile States. In addition the economy is in a critical situation with loss of oil
revenues, high debt burden, prevalence of poverty, and challenges of strengthening reforms,
maintaining performance achieved after the Comprehensive Peace Agreement, 2005, and
improving performance. These transformations have generated social and cultural challenges
and all affect the processes of population development. The Population Situational Analysis
(PSA) is expected to contribute to a better understanding of the causes of a country’s population
dynamics, levels and trends, the reproductive health situation and the status of gender equality,
equity and the empowerment of women and how these are interrelated with the overall
economic development of Sudan, particularly the well-being of the poor. These issues are to be
examined within the context of national development policies and plans, in particular as they
relate to ICPD goals, the national Millennium Development Goals, and the national povertyreduction strategies (as contained in the draft Poverty Reduction Strategy Papers (PRSP).
The PSA is important because it postulates the main challenges faced. Priorities are set forth by
the country through an assessment, demonstrating the importance of population dynamics, their
relationship with social, economic, political and cultural processes. The short and medium-term
repercussions are considered, thus serving as a bench-mark for the country and for national and
international organizations, particularly the United Nations.
1.1 Guiding principles of the PSA:
The PSA emphasizes a human right- based approach and specifically considers the principles of
universality, inalienability, indivisibility, interdependence and interrelatedness. The principles of
participation and inclusion are critical to all population and development activities. In addition,
there is a need to take into account the extent to which existing services are available, accessible
and acceptable and the existing quality standard.
The analysis is guided by principles of equality and the exercise of rights, in pursuant to
international agreements and goals. The ways in which social, gender, age-related and ethnic
differences and their demographic repercussions feed back upon each other through various
pathways and mechanisms are underscored. These inequalities have a natural and direct link
with the exercise of rights in as much as they are symptomatic of the difficulties and constraints
involved when people and groups living under disadvantaged conditions seek to exercise their
rights.
The PSA is considered as a flexible conceptual framework, able to consider transitions, long
term and new emerging trends, for example regarding the character of the national economy and
population mobility. The legal framework in which individual behavior is formed needs to be
considered.
13
The PSA should contribute to greater efficiency and strategic impact of technical assistance in
the field of population and development for public policy formulation and implementation and
especially for the elaboration of national development strategies based on the Millennium
Development Goals (MDGs). To this end, it is anticipated that its content and the language used
will result in a document that will be attractive for various national actors in government, civil
society, and the private sector, as well as cooperation agencies.
1.2 The objectives of the PSA:
Analyze the root causes of the changing a) population dynamics and demographic
profile (levels and trends); b) reproductive health situation; and c) status of youth,
women and girls; taking in consideration the extent to which these realities are
interrelated given the economic, political, socio-cultural and institutional context in
Sudan.
Identify priority population, youth, gender and reproductive health development
challenges/needs and opportunities given the complex context.
Assess the relevance and adequacy of major national and state level population and
development –related policies, legislation, programmes and plans in the context of
social economic and social processes.
Provide a basis for recommending strategic actions responsive to the identified
population gender, youth and reproductive health priority development needs.
1.3 Methodology:
The analysis depends partially on desk–review of available literature and secondary data.
Consultations were done with UNFPA staff and their government and civil society partners on
priority issues requiring deeper analysis. The analysis was discussed with UNFPA staff in
Khartoum and from Regional office. Their insights were taken in consideration.
The timeframe for the production of the document was 20 days. The limited timeframe has not
allowed collection of primary data. However, within this limited time, the team considered a
participatory process discussing interrelatedness of the issues and exchanging preliminary
findings and draft outputs.
The major constraints for the team and a shortcoming in the analysis are the paucity analytical
studies on some issues such as women political and economic participation and youth situation
in rural areas and changes in cultural perspectives. The team dealt with that tactfully using the
available national data, pointing out the gaps and taking them in consideration when
formulating recommendations.
The quality control of the PSA was a priority for the team and was approached by depending on
accessible and recognized sources, being objective in analysis, peer review, openness to
criticism and interaction with UNFPA staff.
14
1.4 Content of PSA:
Following the introduction, section two provides an overview of the socio-economic contexts in
Sudan. This includes a presentation of the political, economic developments with specific
consideration to the health and education public spending as it affects the outcome of assistance
provided by Sudan Development Partners. The social and cultural contextual dynamics noted
the inequalities, poverty and conflict as major challenges related to population dynamics, gender
and RH. Consideration is given to the progress in complying with International Agreements and
Goals
Section three provides the analysis on population dynamics, reproductive health, gender and
youth in consideration to the contextual dynamics of Sudan. The analysis starts with the more
aggregate changes at the level of population issues and RH, where it identifies the most relevant
challenges or problems. It then moves on to a more detailed analysis of the demographic or RHrelated manifestations of social inequality, making it possible to identify the social gaps that are
caused by unequal exercise of rights. The analytical part culminates in the analysis of the
relationships and impacts between population dynamics and social and economic phenomena
and operational conclusions, from which implications for public policies are deduced. Based on
these analyses, framed in the economic, socio-cultural, political and institutional context of
Sudan it finally shows the challenges, opportunities and priorities faced by Sudan in the field of
population and development, RH, gender, and human rights.
In consideration to the analysis provided in the above sections, the priorities, opportunities and
challenges identified, section four proposes areas for future support. The strategic interventions
considered as priority are those that: a) aim to consolidate previous achievements; b) address
different levels of cause and effect common to population and RH challenges; c) focus on
priority needs, rights and capacities; d) address negative or problematic trends; f) offer
opportunities to strengthen national capacities; h) address new emerging critical situation
specifically related to conflicts’ contexts; i) build on lessons learned and good practices; j) have
potential for longer term impact on national goals and priorities;
Suggestions for capacity development and coordination mechanisms are informed by analysis,
challenges and recommendations. The aim is to identify not only effective mechanisms but also
realistic and feasible ones.
15
SECTION TWO:
OVERVIEW: POLITICAL, ECONOMIC AND SOCIO-CULTURAL CONTEXTS
2.1. Political Context:
In the last two decades Sudan has witnessed profound political transformations with the
accession of power by the National Salvation regime, the introduction of an Islamic ruling
system and continuity of recurrent conflicts which disturbed the political relations with some of
the neighboring countries. However, the Comprehensive Peace Agreement (CPA) signed in
2005 ended the long standing civil war in Southern Sudan and gave the people in South Sudan
the choice of unity or separation from the North. The referendum, undertaken in July, 2011,
resulted in the secession of South Sudan. The political challenges for the new government
formed after the secession of the south include among others how to manage economy without
oil resources, maintain peace in the new borders and maintain stability in turbulent political
situation in the Arab region.
The Darfur conflict continues and recently an agreement was signed with some of the rebel
groups and is now in process of implementation. This conflict resulted in a large mass of
internally displaced people who for a long time have been living under critical humanitarian
situation. The emerging conflicts in South Kordofan and the Blue Nile states add to the political
burden.
The relationships of the government with the international community have taken different
momentum with the facilitation role of the latter for the different peace agreements signed and
their continued support.
According to the decentralized system adopted the Sudan is divided into 15states with each state
divided into localities. The states have their autonomy, constitution and legislative councils and
systems of generating resources. They are also entitled to transfer of some resources from the
Federal government. Although, some states have shown independence from the center in taking
some decisions but still most of the political powers and resources are centralized. There are
great variations among the states in the situation of resource base and social development. The
challenge for most of the states is that substantial share of the country resources are allocated
for security and thus very limited resources are available for human and social development.
An important development in the last decade is the tremendous increase in the number of civil
society organizations which are sharing in provision of services and many of them are
advocating for compliance with international agreements and framework.
2.2 The Economy
2.2.1 Economic Liberalization
1. The adoption of a sharp-shock economic liberalization and privatization policy in the early
1990s resulted in hundreds of thousands of job losses, high inflation, scarcity of goods and
16
rising poverty rates with estimates ranging between 40% (official estimate) and 90% (UNDP,
HDR, 1998) of population under the poverty line.
2. The stiff political and diplomatic relationship between Sudan government and the
international community during most of the 1990s, resulted, among other things, in a sharp drop
in foreign aid, from some US$ 800 million in 1989 to 608 in 1990 to 225 in 1994, with direct
implications on welfare and social services and as a result, per capita share of development aid
fell from 23 to 8 US dollars1. ODA became largely limited to humanitarian assistance, mainly
to drought and war affected population and the urban poor, primarilyly through international
NGOs. Internal and external conflicts shifted state resource from economic and social services
to security and defense, causing a sharp rise in unemployment, poverty rates and very low rates
of all human development indicators2. The combination of the liberalization/ privatization
policies, sanctions and the sharp drop in foreign aid has implied the following:
a. The gearing of the aid flow to address humanitarian needs which exploded into
humanitarian crisis as a result of civil wars, drought and desertification, which largely
affected rural population and the laying offs prompted by the economic adjustment
programme and the politically-motivated dismissal of public sector employees in what
was called (Alsalih Al Am policy), which have contributed particularly to the rise in
urban poverty among the middle class.
b. The gradual shift of state social responsibility to the UN agencies, INGOs and civil
society organizations, especially in rural areas, IDP camps and in the states other than
Khartoum. These non-governmental organizations took the lead in providing social
services such as water supply, basic health services, adult education, IGA projects and
were also champions of small scale credit and business projects.
c. The sanctions also contributed to blockage of technology and spare parts which led to
the depreciation and/or total stoppage of operating machinery in some of the public
sector institutions which employ a large number of the labor force such as Sudan
Railways, Sudan Airways, Gezira and Halfa Agricultural schemes as well as the closure
of hundreds of private manufacturing industrial establishments; all leading to drop in
production, labor redundancies, and rising dependency on imports.
2.2.2 Oil and the Growth of the Mono-Product economy:
3. Following the advent of oil in 1999, Sudan economy has experienced its strongest period of
growth and its Gross National Product has doubled more than five times from US$ 10 billion in
1999 to US$ 53 billion in 2008 and real GDP growth rate averaged about 8% during the nine
1 UNDP, World Human Development Report,. 1994 and 1997 quoted in Hassan Abdel Ati The State of Sudanese Children a decade
after the Child Rights Convention, 1999
2 See Sudan Human Development Report 1998 which estimated between 86 and 92% of Sudanese population living under the
poverty line.
17
year period ending in 2008 and approximately 10 per cent in 20073 . However, the pattern of
growth has been characterized by enormous inter-regional and intra-regional variations and
imbalances. The Structure of the Sudanese Economy has gradually shifted from predominantly
reliant on agriculture for growth and exports almost total reliance on the oil. One element of the
structural change in the Sudanese economy has been the increase in the share of the industrial
sector (oil-related) from about 9% during the late 1990s to 21% during the 2004- 7 period. The
shift has been to a greater extent attributed to the advent of the oil sector which alone since 2000
contributes about 12% of GDP. The emergence of the oil sector has also induced growth in the
service component of GDP as reflected in fast growth in the construction services which grew
by about 10% per annum since 1999.
4. The Service Sector has been the fastest growing sector in recent years, surpassing even the
growth in the oil sector. Telecommunication, hotels and restaurants have also flourished, mainly
in the country’s capital (Khartoum) and generated about one-fifth of the GDP during 19962006, Yet, despite these structural shifts, agriculture still remains the main driver of
employment outside the large urban areas4.
5. Oil, the signing of the CPA and the boom in the construction, transport and communication
sectors have contributed to a marked increase in Foreign Direct Investment (FDI) but it was also
heavily concentrated in these sectors and in major towns.
Fi g. 2.1: Econ om i c S e ctor sh are s 2004-9
50
40
30
20
10
0
2004
2005
2006
Agriculture
2007
2008
Indus try
2009
Se rvice s
Source: Central Bureau of Statistics, 2009
3 World Bank Draft Country Economic Memorandum 2009, p. 2; United Nations, Sudan Common Country Analysis 2007, November
2007, p.8
4 World Bank DTIS, December 2008
18
6. The fast growth was checked by the global financial crisis. Prior to the global financial crisis,
the IMF described the Sudanese economy as one of the fastest growing in the world despite the
sanctions. The Gross Domestic Product (GDP) grew from US $ 9.9 billion in 1980 to US$ 57.9
billion in 2008 and was estimated to be around US$ 52.2 billion in 2009. Growth rates increased
from 7.1% in 2003 to 10.2 % in 20075. Sudan’s national investment as a ratio to GDP increased
from 18.4% in 2004 to 19.3% in 2009. Sudan’s foreign direct investment (FDI) increased to
reach 10 billion US$ in 2009. This growth reflects the improvement in foreign direct investment
largely driven by the oil and the telecom and the financial sectors and policies pursued to attract
investors in the respective areas. In 2006, the levels of foreign direct investment (FDI) were
among Africa’s highest with over US $3.5 billion, stimulated mainly by the signing of the CPA
and encouraged by policy reforms, favourable energy and crop prices, rising urban
consumption, and macroeconomic stability6. The global economic shock of 2009 which
resulted in lower oil prices, stagnating domestic oil production and reduction in government
spending7, the annual growth rate dropped to 3.9%. Also Net FDI registered a drop by some US
$ 500 million already by mid 2008, partly due to the completion of several major infrastructure
projects, as well as the estimated US$ 800 million fall of net private transfers (remittances),
from its level in 20068. The IMF in 2009 estimated the drop caused by the global financial
crisis to be between 30% and 36% on both FDI and private transfers9.
7. Up to 2009, and despite the international sanctions, Sudan was considered the 17th-fastestgrowing economy in the world10, coupled with rapid development, largely from oil profits.
Although investment has expanded, most of it was destined for the oil sector and development
was heavily concentrated both sectorally and geographically, leading to inter-regional and interpersonal development and economic gaps, fueling further grievances about regional
marginalization. The poor performance of the non‐oil exports, which altogether contributed
about half a billion of the 2007 export value, raise the challenges of exports diversification,
employment creation and sustained growth, which necessitate the revival of traditional exports
e.g. cotton and the development of non‐traditional exports11.
8. With oil contributing over 95% of merchandise exports and about 50% of government
revenues, the economy was transformed in the third Millennium to a mono‐product economy,
highly dependent on oil exports and revenues. This made the economy highly vulnerable to
global economic shocks and with the cessation of South Sudan with 80% of the oil fields made
the economy highly exposed and practically unable to service its debts or attract FDI (i.e.
5 IMF First Review of performance Under the 2007-08 Staff-Monitored Program, June 2008 and projections for 2008
6 UNDP Sudan: http://www.sd.undp.org/mdg_sudan.htm
7 IMF, World Economic Outlook Database, April 2009, www.imf.org
8 IMF First Review of performance Under the 2007-08 Staff-Monitored Program, June 2008
9 IMF Report on the implications of the Global Financial Crisis for Low-Income Countries, March 2009,
10 Economy, 20 October 2009
11 Ibid p. 8
19
through infrastructural investment) and obviously unable to achieve any tangible progress in the
MDGs.
2.2.3 Economic Vulnerabilities and Challenges:
9. In 2009 the IMF report ranked Sudan as one of the most vulnerable low -income countries in
the global financial crisis due to its high vulnerability to trade, aid and remittances shocks and
adjusted its 2009 GDP growth projections downwards by 6.7%12. The Global Finance Report
on Poorest and Richest Countries (2011), rated Sudan 14th among the Arab countries and 138th
worldwide out of 182 countries with a per capita income of US$ 2465 in 2010 compared to
2380 in 2009, an increase of 3.6%. In the World Bank's Doing Business Survey, Sudan is rated
153 out of 174 countries in 2010 and it fell to 154 in 201113. Most recently, and according to
Geopolicity Inc. (2011), Sudan economy has significantly been affected by the Arab Spring and
it estimated the impact on Sudan GDP to be a loss of 1,047 Million14 (decline in investment
and revenues) and real GDP growth is expected to drop from about 5.2% in 2010 to an average
of 4.2% in the coming months. The IMF estimates of the effect on public expenditure to be (1.56) billion and (-0.37) billion on public revenues15.
10. External debt of Sudan stands at US$ 37.98716 billion by the end of 2010, a rise of 85.4%
of its level in 2000. It is important to note that the principal debt was 16.1 billion, while 21.9
billion (57.6%) is composed of interests and penalties17. Sudan did not benefit from the HIPC
initiative or the debt cancellation (one promise of the CPA dividends) and with the low
repayment rates (average 50 million a year), the drop in ODA, Sudan will remain in debt
distress, can not service its debt or make progress on reducing poverty.
2.2.4 Gold Production & Export Diversification:
11. Non-oil exports as a share of total exports increased from 5% in 2008 to 15% in 2010 and
the total value increased by 68%, reaching US$ 1.7 billion while oil exports reached 9.7 billions
(Fig. 2.2). While the trade balance was actually in deficit for three out of the last five years, the
non-oil export development contributed to the trade surplus in 2010. However, looking at the
composition of this growth in non-oil exports shows, it seems almost entirely driven by rising
values of gold exports. This comes not only at the background of rising prices but also from
increasing gold production, which almost doubled from 2009 to 2010. As a result, export of
gold reached US$ 1bn in 2010, up from US$ 0.4bn in 2009. Diversification away from oil is a
12 Ibid
13 Sudan Interim Poverty Reduction Strategy Paper (IPRSP), Draft No 1, Aug. 2011
14 Geopolicity Inc. (2011), "The Cost Of The Arab Spring & Roadmap For G20/UN Support?: Supporting Political,
Security and Socio-economic Transition Across the Arab Realm", October 2011, pp 34-35, 41
15 IMF Press Release, July 25, 2011, www.imf.org/external/np/sec/pr/2011/pr11292.htm
16 Central Bank of Sudan
17 PRSP p 7
20
welcome and necessary development, but the reliance on yet another commodity to drive this
transition is cause of serious concern18.
Fig. 2.2 Sudan Imports & Exports 2005-2010
2.2.5
Inflation and
Rising Food
Prices:
12. Driven
by a
boost
in
proceeds
from
gold exports
and
favourable oil prices, the official exchange rate moved by 3.7% on a month-to-month basis,
decreasing to 2.68 SDG/US$ in the April-May period, compared to 2.78 SDG/US$ in March
(Fig. 2), but a significant gap exists between the official rates and the black (parallel) market
rates, the latter reached around 4.0 SDG/US$ by September 2011.
13. In view of the growing food imports, this put a sustained pressure on food prices, keeping in
the range of 17-20% according to official reports. However, some basic consumer prices rose by
over 200% since the beginning of 2011. According to the Central Bank of Sudan, imported
inflation increased to 12.4% in April 2011 compared to 9.1 percent in December 2010. This is
largely attributed to the pass-through of the exchange rate impact on imported consumer goods
and the cost of locally produced goods (through higher cost of imported raw materials)19.
14. Sudan prices of staple foods in May 2011 remained close to the all time highs in
March/April 2011, but pressure eased slightly by May to Jump again by August, following the
official independence of South Sudan. Over two months, the staple grains index dropped 22.8%
below the values of March 2011. This decline was driven by dukhn and maize while rice and
wheat price volatility followed instability in their world prices. Prices for the largely imported
rice and wheat continued their upward trend and in May 2011 were respectively 33% and 22%
higher from their level one year ago. Thus, recent developments in food prices are driven by
both domestic and global factors. These are supply-side issues induced by weather-related
production shortfalls and higher and more volatile world grain and food prices which have risen
by 47% since June 201020.
18 Economy, 20 October 2009, p. 4
19 Ibid
20 Ibid
21
15. Although several policy measures have been announced by the authorities to contain
inflation pressures and to mitigate its adverse impact on the vulnerable and the poor, including
cutting import tariffs for wheat, flour, sugar, and capital goods; and releasing grain stocks of
domestic reserves, particularly for sorghum as well as a number of safety net and social
protection programs (e.g. cash transfer, school feeding, free health support, and agriculture and
industry support funds), implementation remains week as indicated by the astronomical
increases in food prices in August and September and the discontent that prompted several
demonstrations in different states.
2.2.6 Economic Adjustments prompted by South Sudan Cessation:
16. Since the beginning of 2011, the government started some fiscal adjustments to meet the
anticipated large fiscal challenges posed by South Sudan secession and loss of oil revenues,
estimated to be as high as 36.5% of total revenues21. According to the World Bank, a large part
of the fiscal adjustment is expected to fall on the expenditure side, which raises the challenge of
Sudan balancing fiscal consolidation against the pressing needs for the development agenda22,
including of course the MDGs commitments.
19. The authorities' plans for adjustment aims mainly at smoothing the transition to re-orient the
economy from an oil-led to an agriculture sector-led model with the inclusion of appropriate
social safety measures. "Past patterns of fiscal adjustment raise concerns for possible negative
effects on service delivery for the poor and supporting the longer term growth agenda"23.
Experience of previous state response to the financial crisis of 2009 showed that cuts were
mainly in the public investment portfolio and the federal transfers to states. The share of public
investment expenditures in overall expenditures was cut down to 13% in 2008/09 from around
19% during 2005-2007. The federal transfers to states, the main source of financing basic
services, also declined in 2009. Other than the concern about the negative impact of such
adjustments on the poor and on the status of social services in the states, there is a concern
about the financing of the intended reorientation of the economy (the corner stone of the policy)
as it requires huge investments in the agricultural sector to revitalize it24.
2.3 Human Development:
21 Statement by Minister of Finance and National Economy Minister, Ali Mahmoud, June 14, 2011 (AlRay
Alaam newspaper, issue No. 476256).
22 World Bank, Sudan, Country Economic Brief, July 2011, The World Bank – Africa Region – PREM
Unit
23 Ibid
24 It is important to note that the government-initiated Public Expenditure Tracking Survey (PETS) report in the health
sector, issued May 22, 2011 indicates that resources allocated to the sector are not used efficiently, are not reaching
lower administrative levels and health facilities and a large share does not reach the intended level/facility
22
1. In 2009, Sudan has scored medium in human development, ranking number 150, with
statistics indicating that about 17% of the population live on less than US $1.25 per day25. The
report also shows there were enormous variations between the different states; with the lowest
ratio of population under the poverty line recorded in Khartoum (26.6%) and the highest
(62.7%) recorded in Darfur (Table 2.1). According to the NBHS (2009) report, the national
poverty rate stands at 46.5% with regional disparities ranging from a minimum of 26% in
Khartoum to a maximum of 69.4% in North Darfur State and the same trend applies for poverty
gaps and severity It is also important to note that gaps also exist within states between the
different localities. The state of affair has increased migration from rural to urban areas, thus
weakening the productive capacity in rural areas, deepened poverty in both rural and urban
areas, and widened the regional imbalances.
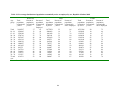
Table 2.1 : Regional Disparities in Some MDG Indicators (2009)
Highest
Lowest
region
region
National
MDG
1.1
% of population below poverty line
62.7
26.6
46.6
MDG
1.2
Poverty Gap ratio
24.6
6.4
16.2
MDG
1.3
Employment Ration for population 15 years &
over
48.5
35.9
41.4
MDG
1.6
% of employed population below poverty line
58.8
21.0
42.5
Source: Sudan National Budget Household Survey, 2009
2. The UNDP 2011 Human development report, ranked Sudan 169 out of 187 countries covered
by the report, a regress of 19 points in international ranking. However, the overall trend has
been progressive since 1980 (Fig. 2.3), though the improvement is modest, especially during the
last decade if compared to economic indicators during the same period. Sudan featured last
among Arab countries26, behind Yemen and Djibouti which ranked 154 and 165 respectively
and was 14% lower than the average HDI for Sub-Sahara African countries (Table 2.2).
25 UNDP, Human Development Report 2009, Overcoming barriers: Human mobility and development. Macmillan.
NY
26 Data for Somalia incomplete
23
Fig. 2.3: S udan HDI 1980-2011
0.5
0.4
0.3
0.2
0.1
0
1980
1990
2000
2005
2009
2010
2011
Source UNDP, HDR 2011
Table 2.2: Sudan HDI 2011
HD
I
Countr
y/
Ran
k
Regio
n
Human
Life
Mean
Developm
ent
expectan
cy
Years
of
Index
at birth
schooli
ng
(HDI)
(Years)
Expect
ed
years
of
schooli
ng
(Years)
(Years)
Gross
Natio
nal
Incom
e
(GNI)
per
capita
GNI
per
capi
ta
Noninco
me
HDI
Ran
k
min
us
HDI
rank
169
Sudan
0.408
61.5
3.1
4.4
1,894
-21
0.402
Arab
States
0.641
70.5
5.9
10.2
8,554
—
0.643
Arab Low HDI States
154
Yem.
0.462
65.5
2.5
8.6
2,213
-11
0.471
165
Djib.
0.430
57.9
3.8
5.1
2,335
-25
0.420
0.463
54.4
4.5
9.2
1,966
—
0.467
Subaharan
Africa
Source: Human Development Report 2011: Sustainability and Equity: A Better Future for All Tables
24
2.3.1 Poverty:
1. The findings of the NBHS (2009)27 on poverty in (North) Sudan28, were the following:
a. Darfur and Kordofan are the highest regions in poverty incidence, poverty gaps and
severity, followed by eastern Sudan, while Khartoum is the lowest in all three indicators
(Table 2.3)
Table 2.3: Poverty Incidence and Poverty Gap by Region
Region
Poverty
incidence
Poverty gap
Severity
(MDG1.2)
(MDG 1.1)
Khartoum
26.0
6.4
2.4
Northern
33.7
9.4
3.8
Eastern
46.3
17.1
9.0
Central
45.4
13.8
6.1
Kordofan
58.7
23.1
11.7
Darfur
62.7
24.6
12.6
Sudan
46.5
16.2
7.8
Source: NBHS (2009)
b. Employment ratio for population above 15 years of age is 41.4% and the ratio of
employed population living below the poverty line is 42.5%, which indicates the gap
between the level of incomes and households' basic needs
c. National average monthly consumption in 2009 was 148 SDGs, with a 61% gap
between urban and rural areas recording consumption levels of 197 and 122
respectively. By region, consumption is highest in Khartoum and Northern region and
lowest in Kordofan and Darfur
d. Average consumption by state clearly show four clusters: Khartoum, followed by River
Nile, Kassala and Northern states; Gezira, Sennar, Western Darfur and Gedarif states
constitute the third group; while White Nile, Blue Nile, Red Sea, North Kordofan,
South Kordofan, South Darfur showed the lowest average consumption
27 CBS, Poverty in Northern Sudan, Estimates from the NBHS, 2009, Sept, 2010
28 It is important to note that many economists have reservations on the food basket upon which the calculation
is based and also one needs to consider the price changes since the cessation of South Sudan
25
e. Food is the highest in consumption items amounting to 62% of consumption, with a
significant difference between urban and rural areas
f.
With poverty line calculated at 113.8 SDGs, 46.5% of the population was found to fall
below the poverty line, 26.5% in urban areas and 57.6% in rural areas.
g. Khartoum is the region with the lowest poverty incidence (about one fourth of the
population and North Darfur the highest with about two thirds of the population below
the poverty line (See Table 2.4)
Table 2.4: Poverty Incidence, Poverty Gap and Severity
State
Poverty
Poverty
Severity
Incidence
Gap
Northern
36.2
10.5
4.2
River Nile
32.2
8.8
3.5
Red Sea
57.7
24.9
13.7
Kassala
36.3
14.7
8.0
Gedarif
50.1
15.9
6.7
Khartoum
26.0
6.4
2.4
Gezira
37.8
10.1
4.1
White Nile
55.5
17.6
7.8
Sennar
44.1
14.0
6.4
Blue Nile
56.5
20.6
9.9
North Kordofan
57.9
24.6
13.1
South Kordofan
60.0
20.7
9.4
North Darfur
69.4
27.4
14.2
West Darfur
55.6
19.8
8.9
South Darfur
61.2
24.5
12.7
Sudan
46.5
16.2
7.8
Source: NBHS (2009)
26
Poverty By Region
Incidence
Gap
Severity
33.7
9.4
3.8
46.3
17.1
9.0
26.0
6.4
2.4
45.4
13.8
6.1
58.7
23.1
11.7
62.7
24.6
12.6
2. According the IPRSP (2011), 46.5% of Sudanese households (approximately 14.4 million
persons) are living below the poverty line. The share of the rural poor is 75%. About 31.5% (13
million) were also classified as food deprived, highest in the Red Sea state (44%) and lowest in
Gezira and River Nile state (15%)29.
2.3.3 Basic Capability Index:
3. Sudan recorded 69 in SocialWatch "Basic Capability Index - BCI 2011"30 ranking. The
index is based on three indicators Child Mortality, Maternal Health and Education in which
Sudan score was, respectively 89, 49 and 49. In fact, as shown in Table 2.5 below, Sudan was
one of the very few countries that recorded a regression from its position in 1990.
Table 2.5: Basic Capability Index (BCI)
Regions
1990
2000
2011
Europe & North America
97
98
98
East Asia & Pacific
86
93
95
Central Asia
90
92
95
Latin America & Caribbean
85
91
94
Middle East & North Africa
76
85
90
South Asia
62
67
74
Sub-Saharan Africa
59
63
68
The World
79
84
87
Sudan
75
69
69
Source: Socialwatch Basic Capability Index 2011
4. The NBHS (2009) report attributed the root cause of the widespread poverty to the long civil
wars and conflicts, urban and regional bias in development policies and programs, lack of
coherent anti-poverty or poverty reduction measures, lack of an economic reform to diversify
the economy and address the regional imbalances, low allocation of public resources to alleviate
poverty particularly in the rural sector, absence of partners (donors) to compensate for the under
29 Sudan Interim Poverty Reduction Strategy Paper (IPRSP), Draft No 1, Aug. 2011, p. 15
30 Source: Socialwatch: Basic Capability Index 2011: progress and regression towards basic social goals;
http://www.socialwatch.org/node/13776
27
funding and the heavy external debt, international sanctions31. Other factors that significantly
contributed to poverty increase include (a) the lack of political will as most of the above factors
require political rather than economic decisions e.g. settlement of conflicts, debt
cancellation/relief and transparency and accountability on public funding, etc., (b) corruption32
and lack of accountability which contributed to the acceleration of poverty situation despite the
oil boom and fast GDP growth, and (c) the sectoral bias in resource allocation mainly at the
expense of the productive, job creating rural sectors
5. The Interim PRSP recommendations for poverty reduction are mainly through what the PRSP
paper calls sustained economic growth, structural transformation and diversification of the
economy and they include (a) Strengthening governance and institutional capacity of the public
sector; (b) Reintegration of IDPs and other displaced population; (c) Developing human
resources; and (d) Promotion of economic growth and job creation33.
2.3.4 Concluding Remarks:
1. The regional geographical distribution of poverty, in both scale and depth (Table 2.3),
indicates that it positively and highly correlates with conflict & pastoral areas, population
displacement, primary production & reliance on natural resources. Ironically, it also correlates
negatively with the areas producing extraction wealth (oil and gold). Thus, Sudan provides
another evidence of the present-day worldwide observation that economic growth driven by
extractive industries "is not benefiting the majorities" of the population of developing
countries34.
2. The deepening of poverty can not be attributed to population-resource imbalance since, as
shown in Fig. 2.4 below, during the last five years economic growth trends were much higher
than population growth rates, which suggest that the central problem is distribution of resources
and not scarcity.
31 Ibid., p 16
32 Internationally recognized institutions have classified Sudan as one of the highest in terms of corruption
http://www.transparency.org/policy_research/surveys_indices/cpi/2010/results
33 Sudan IPRSP, p. 20
34 Social Watch Report 2012, will be launched in the middle of December in New York, Published on 25/11/2011
28
12
10
8
6
4
2
0
Fig. 2.4: Population and GDP Growth rate s
2004-2009
2004
2005
2006
2007
Population Growth Rate (%)
2008
2009
Real GDP Growth Rate (%)
Source; http://www.indexmundi.com/facts/sudan/population-growth
3 When we compare regional poverty rates with the sectoral contribution to the GDP, it reflects
not only lack of development but also exploitation and inequality in terms of state inputs and
revenues from the traditional, natural resource-dependent sectors, which may explain the rise in
ethno-politics and localized nationalism that is expanding in poor regions.
4. The current classification of rural /urban needs to be taken with caution for two reasons.
From the NBHS (2009) while the Red Sea state has the second highest urbanization rate after
Khartoum it is the fourth poorest state and in contrast the northern state has the 3rd lowest
urbanization rate and also the third lowest poverty rate. Besides measured in terms of poverty
depth and the gaps between the poor and the rich (relative poverty) is generally higher in urban
than rural areas35.
5. Critical measures needed to reduce poverty include:
a. Political stability and settlement of ongoing conflicts
b. Improved governance and combating corruption
c. International assistance both technical and financial for direct interventions and political
support to address tensions
d. Enhancing economic interdependencies between Sudan and South Sudan
e. Economic diversification with emphasis on food production and productive
employment-creating sectors.
f.
Regional equality in development and resource allocation
35 Ibid., pp. 12-13
29
g. A special focus on marginalized social groups
6. The impact on the population of the current ongoing conflicts in Darfur, South Kordofan and
Blue Nile states as well as the unresolved issues of the border, oil, debt and Abyei between the
Sudan and South Sudan governments and the discontent with the price increases in the north is
likely to cause (a) large scale instability and massive population displacement and increasing
humanitarian needs, (b) if the conflicts were settled there will be a need for international
assistance to support the repatriation and the rehabilitation of the destroyed infrastructures; (c)
as the conflicts in both South Kordofan and Blue Nile states exploded before the cultivation
season and since both are food producing areas dependent on rainfall cultivation, the occurrence
of a food gap is highly likely not only in the two states but also in other parts of the country.
2.5. Socio- cultural Context
2.6: Compliance to ICPD Programme of Action, MDGs and Beijing Plat- form of Action:
Progress and challenges
2.6.1.: ICPD PROGRESS
There has been some progress in implementing the ICPD Programme of Action at the
country level documented by the Sudan MDGs/ICPD progress report, 2009. The ICPD
goals have increasingly been incorporated into national development frameworks, plans
and policies. A population policy based on ICPD objectives was formulated with
consideration to the specific context of Sudan in 2007 and now in processes of being
updated to adapt to changing context of Sudan. There are initiatives for integration of
population issues in sectoral policies and programmes.
The ICPD Programme of Action emphasized that valid, reliable, timely, sexdisaggregated and internationally comparable data should form the basis for all stages of
policy and programmematic action. The Sudan Household Survey, 2006 and 2008 Census
in addition to other health and education surveys have contributed to provision of data;
however, there continue to be gaps in data quality, gender-sensitivity, availability and
utilization.
2.6.2.: MDGs PROGRESS
Country progress towards the set targets for achievement of the eight MDG goals is as
reflected in Table 2.1. below:
30
TABLE 2.6 Progress in MDG goals
Goals
Targets
Eradicate
extreme
poverty and
hunger
Reduce by half the proportion
of people living on less than a
dollar-a-day
Achieve full and productive
employment and decent work
for all, including women and
young people
Reduce by half, between 1990
and 2015, the proportion of
people who suffer from
hunger
Achieve
Universal
primary
education
Promote
gender
equality
and
empower
women
Ensure that all boys and girls
complete a full course of
primary schooling
Eliminate gender disparity in
primary and secondary
education preferably by 2005,
and at all levels by 2015
Indicators
The proportion of
population below
dollar per day
The proportion of
population below
poverty line
Employment rate
Progress
the
one
25%
the
the
46.5%
Proportion of ownaccount in total
employment(workers
Proportion
of
contributing
family
workers
in
total
employment(workersfamily workers)
Prevalence
of
underweight
children
under five years of age
Proportion of population
below minimum level of
dietary
energy
consumption
Gross enrolment in basic
education
Proportion of pupils
starting in grade 8 of
basic education
Literacy rates of 15-24
year olds, women and
men
Ratio of girls to boys in
primary, secondary and
tertiary education
Share of women in
employment in the nonagricultural sectors
Proportion of seats held
by women in national
31
83%
34%
22%
31.8%
28.0 %
71.1%
N.A
77.5 %
53.9 to 46.1 %
51.6 to 49.4%
54.1% females
59%
25%
Reduce
child
mortality
Reduce by two-thirds,
between 1990 and 2015, the
mortality rate among children
under five
parliament
Under five mortality rate
Infant mortality rate
Proportion of one year old
children immunized
against measles
Improve
maternal
health
Reduce by three quarters,
between 1990 and 2015, the
maternal mortality ratio
Maternal mortality ratio
32
78.4/ 1000 LB SHHS
2010
2008 Census data also
shows that U5MR
decreased by 30% from its
1993 figure; overall, this
indicates a significant
improvement in child
health conditions during
this period
57/1000 LB SHHS 2010
2008 Census data also
shows that IMR decreased
by 27 % from its 1993
figure; the data also shows
a better mortality
conditions for females
than males, Current data
indicates that Sudan is far
from achieving MDG4
given the current trends,
with IMR being closer to
the target than U5MR.
70.1% SHHS 2010
(children 12-23 months)
In 2008 and 2009, FMOH
and development partners
conducted measles
immunization campaigns
focusing mainly on high
risk areas with low
coverage, reaching
629,266 children aged
between 6 and 59 months.
216/100,000 LB SHHS
2010
The huge drop in MMR
reflects the intense efforts
being undertaken, but is
rather disproportionate
when compared to
previous figures and
prevailing service
coverage indicators.
Achieve, by 2015, universal
access to reproductive health
Combat
HIV / AID,
malaria
and other
diseases
Have halted by 2015 and
begun to reverse the spread of
HIV/AIDS
Proportion of births
attended by skilled health
personnel
Contraceptive prevalence
rate (current use)
Adolescent birth rate (1214) years
Antenatal care coverage
(at least one visit and at
least four visits
HIV prevalence among
population aged 15-24
years
Condom use at last highrisk sex
Proportion of population
aged 15-24 years with
comprehensive
correct
knowledge of HIV/AIDS
Achieve, by 2010, universal
access to treatment for
HIV/AIDS for all those who
need it
Have halted by 2015 and
begun to reverse the incidence
of malaria and other major
diseases
Proportion of population
with advanced HIV
infection with access to
antiretroviral drugs
Incidence and death rates
associated with malaria
Proportion of children
under 5 sleeping under
insecticide-treated
bed
nets
33
72.5% SHHS 2010
9% SHHS 2010
76/1000 2008
1 visit; 74.3% SHHS
2010
4 visits: 47.1% SHHS
2010
0.5% males & 1.24%
females 2009
According to SHHS 2010,
the estimated HIV
prevalence among the
general population 15-49
years is 0.67%, reflecting
a low level or
concentrated epidemic
mainly affecting most at
risk and vulnerable
populations.
NA
4% 2006
SHHS 2010 has also
shown that 5.8% of
women aged 15-49 yrs
have correct knowledge
of HIV/AIDs
13.12%
3.1 million reported cases
8,844 deaths
41 %
Incidence, prevalence and
120 per 100,000 pop
death rates associated
with tuberculosis
Proportion of tuberculosis
81.8 %
cases detected and cured
under directly observed
treatment short course
Source: Sudan National MDGs report, 2010; Census 2008, SHHS 2008, 2010
34
SECTION THREE:
POPULATION DYNAMICS, REPRODUCTIVE HEALTH D AND GENDER
3.1. Population dynamics
3.1.1 Population Change and distribution
Increased population growth generally represents challenges for a country; it means increased
need for food, shelter, infrastructure, and services. To plan for the provision of these needs it is
important to know the levels and trends of population growth. This chapter highlights population
size and distribution changes through time in states and by mode of living.
The 2008 census counted 30.9 million people in the Republic of Sudan, a 21 percent increase
from the 1993 census. Sudanese population was counted at successive census as 10.3 million in
1955/56, 14.1 million in 1973, 21.5 million in 1983 and 25.6 in 1993. As indicated by Figure (1),
the population growth of 7.4 million people (52.5%) between 1973 and 1983 represents the
largest census-to-census increase up to date.
During this period the crude death rate decreased from 21to 17.2 and infant mortality rate
decreased from 154 to 118 whereas the crude birth rate changed from 47.5 to 42.6 and total
fertility rate changed from 6.8 to 6.5. The percent change in crude birth rate (10%) and total
fertility rate (4%) were by far much lower than the percent change in crude death rate (18%) and
infant mortality rate (23%). This relative decline in death rates compared to birth rates was the
cause of the rapid population growth in the 1980s. Total decennial population growth declined
sharply in the next decade following the 1980s peak and continued declining but in slow rate
during the 2000s.
35
Figure 3.1. Population Growth and percent change between the censuses 1956-2008.
60
52.5
50
36.9
40
30
20.7
19.1
20
7.4
10
5
4.1
3.8
0
1956-73
1973-83
Grow th (in m illion)
1983-93
1993-2008
Pe rce nt change
Source: Central Bureau of Statistics, 2008 census.
In terms of annual growth rates, The Republican Sudan’s population growth rate (overall as well
as natural) in 2008 was about 2.4%, representing a doubling time of 29 years. We can expect the
Republic of Sudan’s population of 30.9 million in 2008 to become 61.8 million by 2037 if current
growth continues. The population growth rate peaked in 1983- 93 at 2.88% and a doubling time
of 24 years.
Figure 3.2. Annual population growth rates 1956-2008
3.5
3
2.5
2
1.5
1
0.5
0
1956-73
1973-83
1983-93
1993-2008
Source: Central Bureau of Statistics.
36
3.1.2 Population projection for future population growth
According to the official population projections, there are three scenarios of potential population
growth "(low-medium and high). Population is likely to reach in 2031 by the end of the quarter
century strategic plan (2007-2031) to 56.5, 59.9 and 63.4, according to the scenarios referred
before, respectively (see Figure 3).
Figure 3.3. Population projections 2011-2031
High variant
Medium variant
Low variant
63
59
30,9
30,9
56
30,9
2008
2011
2012
2017
2022
2027
2032
Source: National Population Council.
3.1.3 Population distribution by mode of living
There is also a considerable change in population distribution by mode of living. Figure (4)
depicted the percentage distribution of population according to mode of living at successive
census. During the 1955/56 census about 8 percent of the total population live in urban areas
compared to about 19 percent in 1973, 21 percent in 1983, 29 percent in 1993 and 33 percent in
2008. It is clear that there was rural -urban migration because as the urban population was
increasing with annual growth rate more than 4 percent, the rural population decreased from 78
percent in 1955/56 to 70 percent in 1973, and decreased by 10 percent between the 1993 and
2008 censuses. The Nomads were about 13 percent in 1955/56 census, decreased to 11.5 percent
in 1973 and 11percent in 1983, however, in 1993 census the share of the nomads in total
population decreased by 75 percent and increased sharply by more than 100 in the 2008 census
indicating that there was some certain problems in the 1993 census regarding definition of
nomads or in counting them Figure (4).
37
Figure 3.4: Population change according to mode of living 1955/56-2008
90
78
80
70
68.5
70
68.1
58
60
50
40
33
29.2
30
10
20.6
18.5
20
8.3
12.7
11.5
11
9
2.7
0
1955/1956
1973
1983
Urban
Rural
1993
3008
Nom ads
Source: Central Bureau of Statistics.
Percent of urban population to the total population by state is calculated and depicted in Figure
(5). It is clear that the proportion of urban population is by far higher in Khartoum State
compared to the rest of states. The second highest proportion of urbanization is found in Red Sea
State. Both of Khartoum State (The Capital) and Red Sea State (The Country Port) also showed
positive net migration rates.
38
Figure 3.5: Percentage distribution of urban population by state, Republic of Sudan,
2008
Northern State
16.9
W. Darfur
17.3
N. Darfur
17.3
Ge zira
19.1
N. Kurdufan
19.9
S. Darfur
21.6
Sinnar
21.7
S. Kurdufan
23.5
Blue Nile
24.3
Kass ala
26.3
28.5
Al-Gadarif
River Nile
29.6
33.6
White Nile
39.5
Red Sea
81
Khartoum
33.2
The Republic of Sudan
0
10
20
30
40
50
60
70
80
90
Percent
Source: Central Bureau of Statistics, 2008 census.
3.1.4 Population density by region
Population density is the term that describes the number of individuals occupying an area in
relation to the size of that area. Understanding spatial distribution of population is a crucial issue
in planning for development and for distributing resources and power.
Census 2008 put Khartoum’s population at 5,274,321. Khartoum State occupies less than 1
percent of the total area of Republic of Sudan; however, it contains about 17 percent of the total
population. The population density of the state is about 238.20 people per square kilometers, 15
times the national average (before the separation of Southern Sudan). Khartoum is one of the
39
densest regions in the country and it recorded an inter-cenasl population growth of 24 percent
(1993-2008) Table (1 and 2).
Darfur region occupies one fifth of the total area of the country and encompasses about one
quarter of the total population. The share of the total population increased by 3.9 percent points in
1993 and 5.5 percent points 2008 census. On the other hand Northern region occupies 19 percent
of the total area but is the least densely populated region. In 1983 the population of Northern
region was 5.3 percent of the total population, then population decreased to 5.1 percent in 1993
census and increased to 5.9 percent in 2008 due to the exploration of gold.
Table 3.1: Percentage distribution of the total area of Sudan and total population by region
Region Percent
of
Percent of total population
total area
1983
1993
2008
Sudan
%100.00
%100.00
%100.00
%100.00
Eastern
13.61
10.7
12.1
14.8
Northern
19.06
5.3
5.2
5.9
Khartoum
0.84
8.8
13.7
17
Central
5.67
19.6
21.7
24
Kurdofan
15.2
15
12.7
13.4
Darfur
19.79
15.1
19
24.5
Source: Population Report 1994 and 2008 Census.
Table 3.2: State Population density per square Kilometer, Republic of Sudan, 2008
State
Sudan (Before 11/7/2011)
Population density by Kilometer square
15.89
40
Northern
Nar -Alnil
Red Sea
Kassala
Al-Gadrif
Khartoum
Al-Gazera
White Nile
Sinnar
Blue Nile
North Kurdofan
South Kurdofan
North Darfur
West Darfur
South Darfur
2.00
9.17
6.38
48.76
17.92
238.20
152.97
33.96
18.15
56.91
13.16
8.88
7.13
16.46
32.16
Source: Central Bureau of Statistics, 2008 census.
3.1.5. Age and sex structure of population
The most important demographic characteristic of a population is its age-sex structure.
Understanding a population’s age and sex composition yields insights into changing phenomena
and highlights future social and economic challenges. According to the 2008 census, just over
half of the total population was male (51%) and 49 percent were female. Although there are more
males than females born and males outnumber females among children, the sex ratio changes in
adulthood. (The sex ratio is a common measure used to describe the balance between males and
females in the population. It is defined as the number of males per 100 females).
For instance, as presented in Table (3), there were more females than males in every age group
from 20–24 years onwards. The sex ratio dropped from rage of (106-115) males for every 100
females at ages 0–19 years, to 93 males per 100 females at ages 30–34 years. This reversal may
reflect higher mortality among males during civil wars, and sex differences in net migration at the
peak migrant ages of 25–40 years. Counter to expectations at older ages, the difference reflects
higher female mortality rates.
The data presented in Table 3 also include the age distribution of the population. In the 2008
Census, the percent of people under age 14 was 42.6 percent of the total population. The
working-age population, ages 15 to 64, made up 54.02 percent. Finally, the 65 and over
population was 3.38 percent and the dependency ratio is 85%.
41
Analyzing age and sex data is crucial in planning for adequate schools for the school age
population and planning for numerous social services such as, hospitals, health services, and
services for the older population, and measurement of people eligible for retirement and pensions.
Table 3.3: Percentage distribution of population by age and sex, Republic of Sudan, 2008
Age Group
Male
Female
Total
Sex ratio
0-4
14.97
14.89
14.93
106
5-9
15.06
14.56
14.82
109
10-14
13.40
12.30
12.86
115
15-19
10.72
10.61
10.67
106
20-24
8.67
9.42
9.03
97
25-29
7.31
8.64
7.96
89
30-34
6.02
6.79
6.40
93
35-39
5.65
6.19
5.91
96
40-44
4.51
4.55
4.53
104
45-49
3.43
3.22
3.33
112
50-54
2.90
2.69
2.80
113
55-59
1.74
1.50
1.62
122
60-64
1.90
1.63
1.77
123
65-69
1.13
0.88
1.01
135
70-74
1.14
0.97
1.06
124
75+
1.45
1.16
1.31
131
Total Percent
100.00
100.00
100.00
Total number
20,073,977
19,080,513
39,154,490
Source: Central Bureau of Statistics, 2008 census.
Population of median age under 20 years is known to be young, population of median 30 or more
is described as old and populations with median 20-29 is described as intermediate age
Changes in the structure of the population also impact median age. The median age in 2008 was
18.5 years compared to 18.5 in 1993 and the median age for female and male was respectively
18.1 and 19. This indicates that the population is young and in the very few years if fertility is
decreased the percent entering the labor market will increase and a demographic window will be
obtained. However, the major challenge to be faced is securing quality education and augmenting
employment opportunities to absorb the increase in the working age groups.
3.1.6. Components of population dynamics
42
Three demographic forces – fertility, mortality and migration - determine the overall changes in
population. These changes of population impact on size, age composition, sex structure, spatial
distribution and future population growth. These demographic forces can be influenced by
population policies. For instance population policies, through specific programs can directly or
indirectly affect on fertility, mortality and migration. Thus understanding the levels and trends of
these forces help in designing evident- based policy programs that positively influence on these
forces and enhance achieving social and economic development. In the coming sections the
components of population dynamics will be discussed.
3.1.7 Fertility: levels and trends
Fertility is an important factor of human reproduction and is usually the dominant factor in
population growth and population policies. Using several ways of measuring the levels and
patterns of fertility, the report showed the current and inter- censual situation of fertility in the
republic of Sudan.
3.1.7.1. Crude birth rates (CBR)
The crude birth rates is the most basic form of fertility measures referring to the ratio of births
occurred during a year to the total mid-year population and it is usually expressed per 1000
population. It is a crude measure because it refers to the total population and not necessarily
women exposed to childbearing. It is widely used to indicate the overall effect of fertility upon
the growth of population during one year. Inter- censual crude birth rates was calculated and
showed in Figure (6). The crude birth rates declined dramatically between 1956 and 1983, raised
again in 1993 and declined in 2008. It is important to mention that the rates for 1993 and 2008
were the adjusted rates.
Figure 3.6: Crude birth rate 1955/56-2008
43
60
50
40
30
20
10
0
1956
1973
1983
1993
2008
Source: Central Bureau of Statistics.
3.1.7.2. The Age-specific fertility rates (ASFR)
The ASFR are estimated as the number of births to women aged 15-49 by specific age groups.
This information was based on the census question specifically asked to women aged 15-49 on
the number of children they gave birth to, during the 12 months preceding the census date. Based
on these results, the number of births per specific age groups was estimated. Figure (7) shows the
ASFR for the 1993 and 2008 censuses.
Figure (7) obviously shows that the levels of ASFR for 2008 census are lower when compared to
those of 1993 indicating lower fertility levels one year before 2008, especially in the age-groups
20 to 40 years, however the fertility level for both censuses peaked at age 25-29, indicating that
departure time from child birth for women in the two last censuses is the same. Expansion in
females’ education may be behind the stable peak during the two censuses.
Figure 3.7: Age specific fertility rates for Republic of Sudan 1993 and 2008.
44
0.25
0.2
0.15
0.1
0.05
0
15-19
20-24
25-29
30-34
ASFR1993
35-39
40-44
45-49
ASFR2008
Source: Central Bureau of Statistics, 1993 and 2008 censuses.
3.1.7.3. Total fertility rates (TFR)
The total fertility rate determines the average number of children that would be born alive to a
woman (or a group of women) during her childbearing years assuming that she would live
through this period without dying and if the fertility patterns of a given period did not change.
The total fertility rate is a more useful indicator as it’s a single rate that makes it easier for
comparative purposes. The trend in total fertility rates for the period 1973-2010 is depicted in
Figure (8). The total fertility rate 2008-2010 is the lowest compared to the previous censuses. The
lower TFR could be due to the increase in female education and employment. The reported rate in
2008 census was 3.9 whereas the adjusted rate was 5.5. P/F ratio method was used to adjust for
the unreported births one year before the 2008 census (Saif Al-Nasir 2011)
Figure 3.8: Trends in total fertility rates in 1973-2010
8
7
6
5
4
3
2
1
0
1973
1983
1993
2008
2010
Source: Central Bureau of Statistics, 1993 and 2008 censuses.
Total fertility rates and contraceptive prevalence rate by state were calculated and presented in
Figure (9 and 10). According to findings, the overall contraceptive prevalence rate raised from
7.7 percent in 2006 to 9.0 percent in 2010. Although overall progress is only modest, the
45
experience of a few states in increasing contraceptive prevalence particularly stands out. Among
those states are White Nile, Al-Gadarif, South Kurdofan and West Darfur, however, in terms of
total fertility rates, Al-Gadarif, South Kurdofan and West Darfur are still among the states with
the highest rates Figure (9). In Red Sea State, though the contraceptive prevalence rate declined
by 4 percent point, the total fertility rate is by far the lowest. We need to raise contraceptive
prevalence rates in states where fertility rates are high such as Darfur region, Kurdufan region
and Blue Nile State, whereas in Red Sea State further in-depth analysis of determinants of fertility
is needed.
Figure 3.9: Total fertility rates in 2008 by State
Figure 10: Percentage distribution of either
of couples used FP methods, by State 2010
2.4
Red Sea
5.8
Red Sea
2.9
Northern State
4.4
Kassala
3.1
Khartoum
21.6
Northern State
3.1
Kassala
21.3
Khartoum
S. Darfur
3.8
Gezira
3.9
White Nile
4
River Nile
4
S. Darfur
Al-Gadarif
4.8
N. Kurdufan
3
4
5
8.7
Al-Gadarif
6.6
N. Kurdufan
3.5
S. Kurdufan
5.6
Blue Nile
4.2
W. Darfur
5.3
S. Kurdufan
2.5
N. Darfur
4.9
2
7.3
Sinnar
4.8
1
16.4
River Nile
W. Darfur
0
12.8
White Nile
4.5
N. Darfur
9.7
Gezira
4.1
Sinnar
2.1
3
Blue Nile
0
6
5
10
15
20
25
Source: Central Bureau of Statistics, 2008 censuses and Sudan Household Health Survey 2010.
3.1.7.4 Number of children ever born alive
Table (5) presents the distribution of ever married women by number of children ever born alive,
according to five-year age groups. The table also shows the average number of children ever
born. Data on the number of children ever born reflect the accumulation of births to women over
their entire reproductive years, and therefore have limited correlation with current fertility levels,
particularly when a country has experienced a decline in fertility. However, the information on
46
children ever born is useful for observing how average family size varies across age groups, and
for observing the level of primary infertility, particularly for women who have not been able to
conceive any children.
According to the findings of 2008 census data presented in Table (5), about 19 percent of ever
married women reported that they had no children which is an indication of voluntary or
involuntary infertility. Compared to 1993 census, the percentage reported 0 children (9%) was
almost doubled in 2008; the result seems to be exaggerated because the voluntary infertility is not
expected to be high given the low prevalence rate of contraceptives. Most probably those who
did not report were added to 0 children category.
Miss report of births or age is also evident because 18.39 percent of those who were in the age
group 12-14 reported that the number of children they had ever given birth to, was 3 children or
more; the fact which is not supported by their age or duration of marriage. The same error is also
noticed for the successive age groups up to 25-29.Thus we expect the women at these age groups
either misreported their age or the number of children they had given birth to, and most probably
they misreported their age because number of births are always reported much lower than the real
to avoid evil eyes.
47
Table 3.4: Percentage distribution of children ever born alive by ever married women and average number of
children born alive, according to age groups of ever women, Republic of Sudan, 2008
Age
group
Total
0
1
2
3
4
12 -14
66.64 8.02
4.90
4.03
3.72
15 -19
51.65 28.53 12.12 3.43
1.53
20 - 24
26.70 22.80 23.84 14.20 7.02
25 - 29
17.08 11.93 17.57 17.71 15.08
30 - 34
14.20 7.51
11.29 13.31 14.43
35 - 39
12.19 4.82
7.54
9.64
12.31
40 - 44
12.37 4.23
6.46
8.52
10.44
45 - 49
11.71 3.88
5.64
7.42
9.37
50 - 54
14.54 4.19
5.53
6.89
8.34
Total
18.56 10.50 12.14 11.38 10.86
Source: Central Bureau of Statistics, 2008 census.
5
6
7
8
9
10
3.37
0.65
2.49
9.56
12.87
12.34
10.99
10.13
9.06
9.08
3.56
0.85
1.51
6.15
12.18
14.54
13.59
12.53
11.42
9.27
1.89
0.34
0.46
2.35
6.04
8.80
8.97
9.35
8.66
5.45
0.99
0.23
0.29
1.22
3.77
7.05
7.78
8.61
8.55
4.34
0.83
0.14
0.12
0.46
1.87
4.61
5.74
6.89
7.15
2.98
2.05
0.53
0.55
0.88
2.52
6.16
10.91
14.46
15.67
5.42
48
100.00
100.00
100.00
100.00
100.00
100.00
100.00
100.00
100.00
100.00
Number
of
women
ever
married
32204
346450
751282
965227
840237
842119
637147
456175
393868
5264708
No of
children
born alive
Average
Number of
children
born alive
44386
309849
1326291
2761444
3225275
4015028
3330234
2569777
2197981
19780265
1.38
0.89
1.77
2.86
3.84
4.77
5.23
5.63
5.58
3.76
3.1.7.5 Mean number of children born alive according to the mode of living
Average number of children born according to mode of living was calculated and depicted in
Figure (11). The mean number of children ever born increases with women’s age. While women
aged 12–14 (for all modes of life) had less than 2 children on average, women aged 50– 54 had at
least 4.7 children. Counter to expectations, the average number of children ever born to the
nomad’s women across all age groups is less than that of their urban and rural counterparts.
Figure 3.11: Mean number of children born alive according to the mode of living, by age,
Republic of Sudan, 2008
7.00
6.00
5.00
4.00
3.00
2.00
1.00
0.00
12 -14
15 -19
20 - 24
25 - 29
30 - 34
35 - 39
Urban
Rural
Nomad
40 - 44
45 - 49
50 - 54
Source: Central Bureau of Statistics, 2008 census.
3.1.7.6 Mean number of children ever born alive by education
Mean children ever born alive was also measured against women educational level. It was found
that the educational level influences the average parities negatively, implying that the average
parities decreases with increasing level of education. In Figure (12), the mean children ever born
alive decreases from 4.3 children for the women whose level of education was junior secondary
to 3.2 children for those whose level of education was secondary and to 2.8 for educational level
above secondary.
However, the relationship between educational level below primary and
average parities is mixed, in that the mean children ever born alive for women with no
educational attainment was lower than that of women with Khalwa1 education (3.9 vs.4.5) and
49
lower parities were reported by women with incomplete primary level compared to those with
primary level (3.6 vs. 4.2).
Figure 3.12: Mean number of children born alive by education, Republic of Sudan, 2008
4.5
4.5
4.2
4.3
3.9
3.6
4
3.3
2.8
3.5
3
2.5
2
1.5
1
0.5
0
No educational
attainment
Khalwa
Incomplete
primary
Primary
Junior
Secondary
Above
secondary
Source: Central Bureau of Statistics, 2008 census.
1-Pre- school education for religious studies
3.1.8 Trends in mortality
As indicated by Figure (13), the estimated Crude Death Rate (CDR) declined sharply between
1956 and 1993 and this was evident by the rise in life expectancy at birth from 38 in 1956 to
about 54 in 1993, however, between 1993-2008 the CDR decreased and life expectancy increased
50
but in a decreasing rate, may be due to civil wars in Southern and Western Sudan (Figure 13 and
14).
Figure 3.13: Life expectancy 1956-2010.
Figure 3.14: Crude death rates 1956-2010
life expectancy
Crude death rates
70
30
60
25
C D R /1000
years
50
40
30
20
20
15
10
5
10
0
0
1956
1973
1983
1993
2008
1956
2010
1973
1983
1993
2008
2010
Source: Central Bureau of Statistics, 1955/56-2008 censuses and (SHHS) 2010.
Maternal mortality rate declined from 554 maternal deaths per 100000 live births in 1989/1990
(as estimated by Sudan Demographic and Health survey) to 559 in 1999/2000 as indicated by
Safe Motherhood Survey, and declined further to 436 in 2008 census and to 215 in (Sudan
Household Health Survey 2010) (Figure 15). The sharpest decline was between 2008 and 2010
(50.7%). The reduction in maternal mortality rate between 1990 and 2010 was 57.8 percent, and
further reduction of 17.2 percent points is required if the Millennium Development Goal 5 is to be
achieved by 2015.
Figure 3.15: Maternal mortality rates1989-2010.
51
600
554
509
500
436
400
300
215
200
100
0
SDHS
SMS
Census
SHHS2
Source: Central Bureau of Statistics.
SDHS= Sudan Demographic and Health survey, SMS= Safe Motherhood Survey, Census
2008, SHHS2= Sudan Households Health Survey 2010
The infant mortality rate declined from 175/1000 live birth in 1956 to 79/1000 in 2008 and to
57/2010 in 2010. The under five mortality rate also declined from 233/1000 in 1956 to 78/1000 in
2010. For infant and child mortality rates, the least decline was between 1983 and 1993. During
this period the country witnessed the starting of the second civil war in Southern Sudan and some
natural crises such as drought and desertification in Western Sudan, which had an adverse effect
on infants and child health.
Figure 3.16: Child and infant mortality rates 1956-2010, Republic of Sudan
250
200
150
100
50
0
1956
1973
1983
1993
Under five m ortality rate
2008
2010
Infant mortality rate
Source: Central Bureau of Statistics.
The infant, child and maternal mortality rates as well as the crude death rates and life expectancy for
the 2008 census (by state), are depicted in Table (6). The table also includes the maternal mortality
52
rates in 2010. According to the results, Blue Nile State reported the highest crude death rate and the
lowest life expectancy, whereas the lowest crude death rate and highest life expectancy was found to
be in Northern State. The Blue Nile State also reported the highest infant mortality rate while the
highest child mortality rate was reported by Sinnar In addition to these states, infant and child
mortality rates were high in Al-Gadarif and S. Kurdufan. Moreover, North and West Darfur reported
by far the highest rate of maternal mortality in 2008. Nevertheless, 71 percent reduction in maternal
mortality in 2010 was evident in Northern Darfur (Table 6).
Table 3.5: Infant, child and maternal mortality rates, Crude death rates and Life expectancy by
State, 2008 and 2010
Infant
Under five
Maternal Crude
Life
Expectancy
State
mortality rate
mortality rate
mortality rate death
rate
2008
2008
2008
2010
2008
2008
Northern State
65
89
437
127.1
15.7
63
River Nile
69
96
443
147.2
16.2
61.7
Red Sea
66
91
565
280.1
16.6
60.3
Kassala
76
106
466
244.9
17.2
58.3
Al-Gadarif
102
147
564
267.1
17.9
55.9
Khartoum
75
97
389
175.4
16.3
61.4
Gezira
70
111
422
185.8
16.3
61.3
Sinnar
90
205
509
105.6
17.2
58.3
Blue Nile
137
128
578
258.0
20.0
50.1
White Nile
79
128
503
168.5
16.6
60.2
N. Kurdufan
81
114
532
208.0
16.7
59.8
S. Kurdufan
100
143
591
112.4
17.6
56.7
N. Darfur
59
80
618
177.5
15.7
63
W. Darfur
88
125
615
322.2
17.2
58.2
S. Darfur
70
96
581
334.9
16.3
61.4
Source: Central Bureau of Statistics.
3.1.9. Migration trends
Migration is one of the three components of population growth. Any change in the volume and
flow of migration will change the size, growth, and other characteristics of the population both in
sending and receiving areas. Migration within a country does not affect its total size of the
population and growth rate but it affects regional and sub- regional population distribution. But
migration into and/or outside the country does affect the size and the growth of its population.
53
There are two types of migration: internal and internalnational migration. Regarding the internal
migration, people move from region to region or from state to state within the same country. In
international migration people move to outside the country. Those who are moving in a country
are called immigrants and those who are leavening the country are called emigrants.
3.1.9.1 Immigration
Immigration flows are mostly from neighboring countries and represent a typical case of SouthSouth migration. The stock of foreign-born population in 2010 is estimated at around 750,000
people. The informal nature of human mobility from neighboring countries and the existence of
an irregular migration phenomenon in the country mean that the total number of foreign nationals
in Sudan could be much higher. Most the foreigners in Sudan (around 685,000) are recognized
refugees coming mostly from Eritrea, Chad and Ethiopia. These stocks decreased by around half
in the last 20 years due to voluntary and organized repatriations. In addition, a number of asylum
seekers and an unspecified number of irregular migrants from the same neighboring countries are
resident and/or transiting through Sudan, the latter generally spending long periods in the cities
along the main migration routes towards Libya, Egypt and the Red Sea coast. Given the need for
self-maintenance, many refugees and irregular migrants enter into the informal labor market
(IOM, 2011).
A last main category of foreigners is represented by economic migrants coming from the
neighboring countries and other countries such as China, India, Philippines and Turkey – working
in national and international positions, according to the development of the Sudanese labor
market which widely requires, at this stage, the contribution of qualified manpower from abroad.
Overall, young men compose the majority of immigrant population, although families and women
are also present, especially in the case of refugees. Immigrants are mostly located where the
pressure from neighboring countries is higher, i.e. Eastern Sudan, Darfur and Khartoum State
(IOM, 2011).
3.1.9.2 Emigration
Sudan counts between 880,000 and 1,338,000 economic migrants, over half of which are
concentrated in Saudi Arabia, with the rest in other Arab countries and a smaller proportion in
Western countries. Sudanese in Saudi Arabia tend to be mostly male single workers (54%).
Sudanese in Arab countries work prevalently in low-skilled occupations (around 75-80%), white
collar jobs (around 12-15%) and high-skilled occupations (5-10%) including medical specialists,
engineers, university professors, teachers, lawyers, legal advisers, entrepreneurs and managers
suggesting the existence of brain drain in some professional categories such as health
professionals.
54
According to UNESCO, overall approximately 2,900 Sudanese leave abroad for tertiary
education each year to the West as well as other countries such as Malaysia, Egypt, Uganda,
Kenya, India and Pakistan. Anecdotal evidence seems to confirm that one of the preferential
routes to emigration of highly skilled Sudanese is through pursuit of undergraduate and
postgraduate studies abroad (IOM, 2011).
3.1.9.3 Internal migration
The lifetime migrants for the whole country (commonly referred to as inter-state migration) were
3,665,007 representing 9.75% of the total population. The number of migrants increased rapidly
from 0.7 million in 1973 to 1.3 million in 1983, to 3.4 million in 1993 and 3.7 million in 2008. The
sum of the net lifetime gains or net lifetime losses measures the population redistribution due to
lifetime migration for the entire country. Thereby, the amount of lifetime migration, which
accounted for the population redistribution in 2008, was 1,993,171 or 5.31% of the total population.
Khartoum State had 1,952,650 arrivals from interstate, with the majority of people coming from
North Kordufan (310980), Al-Gezira (290888), South Kordufan (219488) and Northern State
(211848). Also 154420 people left Khartoum State for other states with the majority going to AlGazera (23458), Northern State (12242), North Kordufan (12634),Nahr Al-Neel (11730), Northern
Bahr El Ghazal (11056) and South Kordufan (10200).
The current1 migrants for the whole country numbered 304060, and were 0.82% of the total
population. According to the 2008 census data, Al-Gadrif and Kassala had negative net migration
rate (respectively -0.03 and -0.07) and the largest out-migration rate were experienced by Northern
State (-0.93), West Darfur (-0.46) and Al-Gezira (-0.45). Among the states that showed a positive
net migration were Khartoum (0.51%), Blue Nile (0.1) and Red Sea (0.09) Table (7). In Tables (7
and 8), Southern states are still present to keep the figures balanced since an out- migrant of one
state is an in-migrant of anther state.
55
1- Those who had changed their place of residence within the year preceding the census.
Table 3.6: Current In-Migrants, Out-Migrants and Current Net Streams of Migration and
Migration Turn-Over, Sudan: 2008 census
In migrants
Both sex
Northern
Nahr El Nil
Red Sea
Kassala
Al Gedarif
Khartoum
Al Gazira
White Nile
Sinnar
Blue Nile
North Kordofan
South Kordofan
North Darfur
West Darfur
South Darfur
Upper Nile
Jonglei
Unity
Warrap
Northern Bahr El Ghazal
Western Bahr El Ghazal
Lakes
Western Equatoria
Central Equatoria
Eastern Equatoria
Number
4339
5322
4729
3667
4783
73665
10249
11733
5868
5119
10784
7843
3428
2021
11617
17625
17231
6465
23260
18026
16838
4657
8311
12556
13922
Out migrants
Rate
Number
0.65
10559
0.50
8885
0.36
3487
0.21
4955
0.37
5167
1.53
48999
0.30
25596
0.71
14942
0.48
8714
0.66
4361
0.39
16560
0.58
13172
0.17
7964
0.16
7740
0.29
14997
1.98
12293
1.36
9944
1.28
5211
2.59
13256
2.71
7170
5.97
17926
0.81
7213
1.46
9834
1.29
17706
1.67
7409
56
Net migration
Rate
Number
1.56
-6220
0.83
-3563
0.26
1241
0.29
-1287
0.40
-384
1.02
24666
0.74
-15347
0.91
-3210
0.71
-2847
0.56
758
0.59
-5777
0.98
-5329
0.40
-4536
0.62
-5719
0.38
-3379
1.39
5332
0.79
7287
1.03
1254
1.50
10004
1.10
10855
6.34
-1087
1.25
-2555
1.72
-1523
1.81
-5150
0.90
6513
Rate
-0.93
-0.34
0.09
-0.07
-0.03
0.51
-0.45
-0.19
-0.23
0.10
-0.21
-0.40
-0.23
-0.46
-0.09
0.60
0.57
0.25
1.12
1.63
-0.39
-0.44
-0.27
-0.53
0.78
Migration turnover
Number
Rate
14898
2.22
14207
1.34
8216
0.62
8622
0.50
9951
0.78
122664
2.55
35845
1.05
26675
1.62
14582
1.19
9480
1.22
27344
0.98
21015
1.57
11393
0.57
9761
0.79
26614
0.67
29918
3.36
27175
2.14
11676
2.31
36516
4.07
25196
3.79
34764
12.33
11870
2.06
18145
3.19
30262
3.12
21332
2.56
Total
304060
0.82 304060
Source: Central Bureau of Statistics, 2008 census.
0.82
0 0
608119
1.65
3.1.9.4 Sex selectivity of migration
Migration differentials can be based on sex, age and other social and economic characteristics. It is also
well known in the Sudanese culture that households are headed by males and the head of the household
move first and then the rest of the family follows.
For both current and lifetime migration, in 2008, Khartoum, Red Sea, Blue Nile, Unity and Western Bahr
El Ghazal were equally attractive for both males and females. However, Southern states such as Upper
Nile, Jonglei, Warrap, Northern Bahr El Ghazal and Eastern Equatoria have become attractive regarding
the current migration. Unlike the males Al-Gadarif State is attractive to the females; the balance net
migration for the females in Al-Gadarif, thought marginal, is positive compared to the males. On the
whole, the migration turn-over for males was registered as 1.73%, slightly more than their female
counterpart, 1.57 % (Table8).
Table 3.7: Current In-Migrants Out-Migrants and Net Lifetime Streams of Migration and
Migration Turn-Over by sex, Sudan: 2008 census
Current in migrants
Current out
Current net
Current
Usual residence
and previous
migrants
migration
migration Turnresidence
over
Male
Northern
Nahr El Nil
Red Sea
Kassala
Al Gedarif
Khartoum
Al Gazira
White Nile
Sinnar
Blue Nile
North Kordofan
Number
2352
2697
2212
1900
2204
39198
5366
6165
3007
2762
6457
Rate
0.71
0.51
0.30
0.20
0.35
1.55
0.33
0.77
0.51
0.71
0.49
South Kordofan
3927
0.60
6958
1.06
-3031
-0.46 10885
1.67
North Darfur
2107
0.21
4831
0.48
-2724
-0.27 6938
0.69
West Darfur
South Darfur
996
6667
0.17
0.32
4430
8698
0.73
0.42
-3434
-2030
-0.57 5426
-0.10 15365
0.91
0.74
9776
8610
3101
11338
2.08
1.27
1.25
2.66
6892
5460
2636
6967
1.48
0.81
1.07
1.65
2884
3149
466
4371
Upper Nile
Jonglei
Unity
Warrap
Number Rate Number Rate
5088 1.52
-2736 -0.82
4502 0.84
-1805 -0.34
1955 0.26
258 0.03
2511 0.27
-611 -0.06
2667 0.42
-462 -0.07
25747 1.02
13452 0.53
13646 0.83
-8280 -0.50
7844 0.98
-1679 -0.21
4658 0.78
-1651 -0.28
2193 0.57
569 0.15
8485 0.64
-2028 -0.15
57
0.61
0.46
0.19
1.02
Number
7441
7198
4167
4411
4871
64945
19012
14009
7666
4954
14942
16668
14070
5737
18305
Rate
2.24
1.35
0.56
0.47
0.77
2.57
1.16
1.75
1.29
1.28
1.12
3.55
2.07
2.31
4.29
Northern Bahr El
Ghazal
Western Bahr El
Ghazal
Lakes
Western Equatoria
9374
2.98
3602
1.17
5772
1.84 12976
4.13
9309
6.52
9057
6.36
251
0.18 18366
12.87
2281
4315
0.78
1.50
3854
4891
1.31
1.69
-1573
-576
-0.54 6136
-0.20 9207
2.10
3.19
Central Equatoria
7290
1.47
9791
1.96
-2501
-0.50 17081
3.44
Eastern Equatoria
7629
1.81
3679
0.88
3950
0.94 11308
2.68
Total
161042
0.87
161042 0.87
0
0
Current in-migrants
Current outNet migration
migrants
Number
Rate
Number
Rate Number
Rate
1987
0.59
5471 1.60
-3484 -1.03
2625
0.50
4383 0.83
-1758 -0.33
2516
0.43
1533 0.26
984 0.17
1767
0.23
2444 0.31
-677 -0.09
2579
0.40
2500 0.38
79 0.01
34467
1.51
23252 1.02
11214 0.49
4883
0.27
11950 0.67
-7066 -0.40
5568
0.66
7099 0.84
-1531 -0.18
2860
0.45
4056 0.64
-1195 -0.19
2357
0.60
2168 0.55
189 0.05
4326
0.30
8075 0.55
-3749 -0.26
3916
0.57
6214 0.90
-2297 -0.33
1322
0.13
3133 0.32
-1812 -0.18
1025
0.16
3310 0.51
-2285 -0.36
4950
0.26
6299 0.33
-1349 -0.07
7849
1.87
5401 1.29
2448 0.58
8621
1.46
4484 0.77
4138 0.70
3363
1.31
2575 1.00
788 0.31
11922
2.54
6288 1.36
5634 1.20
8652
2.47
3569 1.03
5083 1.45
Female\Total
Northern
Nahr El Nil
Red Sea
Kassala
Al Gedarif
Khartoum
Al Gazira
White Nile
Sinnar
Blue Nile
North Kordofan
South Kordofan
North Darfur
West Darfur
South Darfur
Upper Nile
Jonglei
Unity
Warrap
Northern Bahr El
Ghazal
Western Bahr El
7530
5.41
8868
Ghazal
Lakes
2376
0.84
3358
Western Equatoria
3996
1.42
4942
Central Equatoria
5266
1.11
7915
Eastern Equatoria
6293
1.53
3730
143018
0.79
143018
Total
Source: Central Bureau of Statistics, 2008 census.
3.1.10. Urbanization
58
322084
1.73
Migration Turnover
Number
Rate
7458
2.20
7009
1.33
4049
0.70
4211
0.54
5079
0.78
57719
2.52
16833
0.94
12667
1.50
6916
1.09
4526
1.16
12402
0.85
10130
1.47
4455
0.45
4335
0.67
11249
0.59
13250
3.15
13105
2.22
5938
2.31
18211
3.88
12221
3.49
6.31
-1338
-0.96 16398
1.19
1.75
1.66
0.91
0.79
-983
-947
-2649
2563
0
-0.35
-0.34
-0.56
0.62
5734
8938
13181
10023
286035
11.79
2.03
3.18
2.78
2.43
1.57
Urbanization is generally defined as the convergence process of population to urban areas, and
measured by the indictor of urbanization - level, which is the ratio of urban population to the total
population in a region or a county.
In Sudan, the highest densities are along the river network and more than 70 percent of the population
was rural up to 1973. However, since the mid 1970s, as a response to natural and man-made disasters
and the inequality of resource distribution most of people migrated to Khartoum, where most of Sudan’s
economic capital and social services are concentrated. During the 1980s and 1990s urban growth rate
has been accelerated due to the effects of a wide variety of climatic or political crises Figure (17).
Figure 3.17: Percentage of urban population to the total population
1956-2008
35
30
25
20
15
10
5
0
1956
1973
1983
1993
2008
Source: Central Bureau of Statistics, 2008 census.
Khartoum’s urbanization, however, is pathological; in the sense that people increase in number
without being fully integrated into the urban system. Migrants always set up rural forms of
community; self-help systems to enable them to adapt to new harsh realities. But their economic
survival depends on the lowest-end of the labor market, namely unskilled jobs with long hours
and often far from their homes. Most of people, lost their rural livelihoods before moving to
cities, and were neither empowered to get return to their former livelihoods nor provided with
alternative means of sustainable life in the city.
59
The in-migrants being unintegrated is due to the limited capacities of cities to absorb the masses
of people. In fact, there will be pressure on the already deprived resources and the process is more
likely ruralization of the city.
Misdistribution of population among regions affects development; in that increased population will
swallow any savings in the receiving urban centers and agricultural production will decrease as the
rural areas had lost the skilled and young people. This will end up with impoverishment of the
urban and the rural areas as well. Establishment of city centers in the peripheries, development of
rural areas, rehabilitation of the agricultural schemes, equity in distribution of resources between
states and ensuring security is essential to encourage migrants to return back home.
3.1.11 Population characteristics
3.1.11.1. Marriage
According to the 2008 census, about 49% of the total population (aged 12 years and above), were
married, whereas, 36%, 3% and 2% were respectively unmarried, widowed and divorced. The
percentage of those who had never married among urban population, aged 12 years and above, was
41% compared to 36% and 29% respectively among rural and nomadic population. The unmarried man
to unmarried women ratio in northern Sudan was 120, indicating that for every 100 unmarried women
there were 120 unmarried men. However, it varied by state and ranged from 91 in North Kordufan to
166 in Red Sea. In addition to North Kordufan, there were two states where the unmarried men to
unmarried women ratios were below 100; these states were: Sinnar (98) and Al-Gezira (95).
Table 3.8: Percentage distribution of population by marital status according to age and sex , 2008
census, and percentage never married persons by age and sex, SMS 1999 and 1993 census,
Republic of Sudan
Widowed Divorced
Total
Total
Percent
Age
Never
Currently
Percent number
never
married
married
2008
2008
2008
2008
married
interval
2008
2008
in 1999
12-14
15-19
20-24
25-29
30-34
35-39
40-44
45-49
98.95
96.97
80.98
51.91
29.27
14.82
8.43
5.31
0.96
2.84
18.46
46.89
69.05
83.32
89.13
92.14
0.06
0.09
0.19
0.33
0.52
0.65
0.95
1.05
Males
0.04
0.09
0.37
0.87
1.15
1.21
1.49
1.50
60
100.00
100.00
100.00
100.00
100.00
100.00
100.00
100.00
1067396
1420058
1020564
908960
803217
791428
650993
491850
99.8
98.9
90.1
62.5
31.6
15.5
4.6
3.0
Percent
never
married
in 1993
99.8
98.2
85.9
56.8
32.2
13.5
6.0
3.8
Total,15-49
51.07
47.68
0.44
0.80
100.00
12-14
15-19
20-24
25-29
30-34
35-39
40-44
45-49
Total,15-49
Females
96.61
75.76
39.69
19.70
12.36
7.46
5.41
3.92
29.81
3.20
23.41
57.82
76.76
82.58
86.18
84.64
83.22
65.55
0.09
0.23
0.64
1.06
1.95
2.97
6.01
8.80
2.20
0.10
0.61
1.85
2.48
3.11
3.39
3.95
4.06
2.44
100.00
100.00
100.00
100.00
100.00
100.00
100.00
100.00
100.00
6087070
951254
1429013
1245736
1202099
958766
909968
673574
474800
6893957
53.9
55.2
99.4
84.3
53.9
28.4
15.4
6.7
4.2
1.8
38.1
98.0
79.4
44.6
19.7
10.3
4.0
2.3
1.6
31.9
Source: Central Bureau of Statistics, 2008 census.
The singulate mean age at marriage (SMAM) measures the average number of years a woman
would live as “never married”, if she has the same age specific “risks” of marriage as the
population at large. The measure is based on the assumption that no single person would marry
after his/or her 50th birthday and no one would marry before the age of 15 and measured from
census data. The measure results in an estimate of the
average number of years lived in the single state by those who married before age 50.
In northern Sudan, singulate mean age at marriage was 21.6, compared with mean age at first
marriage for female (22.7) years in the 1993 census. A significant differential in singulate mean
age at marriage by mode of living is evident; (SMAM) in urban areas was 22 years compared to
21 and 19 years in rural and nomadic areas respectively. Figure (18) also depicts the percent of
unmarried women for the groups (15-34) between 1989 and 2008. According to Figure (18), the
percentage of unmarried women, across all age groups, was lower in 2008. This contradicts with
the lower fertility rates discussed before, especially when compared in the context of the low
contraceptive prevalence rate.
61
Figure 3.18: Distribution of never married women by age, SDHS1989, 1993 Census, SMS
1999 and 2008 Census.
90
80
70
60
50
40
30
20
10
0
SDHS
Census 1993
SMS 1999
Census 2008
15-19
20-24
25-29
30-34
Source: Central Bureau of Statistics, 2008 census.
3.1.12. Employment
Economically active population is the fraction of population that is either employed or actively
seeking employment. Economic activity participation rate (calculated as the percentage of
economically active population of the total population) was 26 percent in 2008 census compared
to 30 percent in 1993. This drop may be due to the difference in identification of economically
active population between the two censuses. The refined economic activity participation rate
(excluding children from the total population) was 37% in 2008.
Labor force had increased from 4.5 million in 1983 to 6.5 million in 1993 and to 8 million in
2008. Nevertheless the labor force growth rate decreased from 3.9 percent between 1983 and
1993 to 1.3 percent between 1993 and 2008. The growth in employment rate also decreased from
3 percent to 0.9 percent during same period.
The percent of population employed was 21.6 percent in 2008 and thereby the economic
dependency ratio is 78.4 percent indicating that every working candidate is economically
responsible for other 3.6 persons. In line with these findings, the rate of unemployment increased
from 8 percent in 1983 to 11 percent in 1993 and to 15.9 percent in 2008.
Participation rate in economic activity of males (55%) is by far higher than that of females
(20%). A bout 13 percent of males and 10 percent of females in the age group (10-14) were
engaged in economic activities, putting at stake their education and their normal development to
62
adulthood. The percent of economically employed males for all age groups were higher than that
of their female counterparts (Table, 10).
63
Table 3.9: Percentage distribution of population economically active an employed by sex, Republic of Sudan, 2008
Age
group
Total
population
economicall
y active
Both sexes
Percent of
population
economicall
y active
Percent of
population
economicall
y active
employed
83
69
73
76
80
86
89
90
91
90
90
89
89
88
86
Total
21492517
37
10 -14
3939865
13
15 -19
3239398
23
20 - 24
2729791
35
25 - 29
2367947
46
30 - 34
1921319
52
35 - 39
1809339
54
40 - 44
1404827
56
45 - 49
1013025
57
50 - 54
885371
55
55 - 59
507530
53
60 - 64
569602
46
65 - 69
320732
42
70 - 74
353597
33
75 and
430174
22
over
Source: Central Bureau of Statistics, 2008 census.
Total
population
economica
lly active
Male
Percent of
population
economicall
y active
Percent of
population
economically
active employed
Total
population
economica
lly active
Female
Percent of
population
economicall
y active
Percent of
population
economically
active employed
10779251
2084963
1641443
1305141
1074013
907673
865910
706737
524907
464497
276299
310836
183691
192295
240847
55
16
31
52
72
80
84
84
86
82
80
68
62
49
32
86
71
76
80
85
88
91
91
92
91
91
90
90
89
87
10713266
1854902
1597955
1424650
1293934
1013646
943429
698091
488118
420874
231231
258766
137041
161302
189326
20
10
14
19
25
26
27
28
27
25
21
19
15
13
10
75
66
67
65
71
78
83
84
86
84
86
83
84
83
79
64
More nomad children tend to begin economic activity at an early age compared to rural and
urban ones. Figure (19) shows that 39 percent of those who aged 10-14 years in nomadic
areas and respectively 14 percent and 4 percent of their rural and urban counterparts were
economically active. As nomadic people are pastoralists and most of rural people are
involved in agricultural activities, their children at early age were engaged in animal herding
and agricultural activities, whereas the majority of children in urban areas go to school. This
is also true for the elders (60+) in that, economic activity participation rates for 59 years of
age or above was the lowest in urban areas compared to their counterparts in rural and
nomadic areas, indicating that fewer urban people demand for work after retirement age.
Figure 3.19: Economic activity participation rate in urban, rural and nomadic areas by
age, Republic of Sudan, 2008
70
60
50
40
30
20
10
2
30 9
34
35
39
40
44
45
49
50
54
55
59
60
6
65 4
69
7
75 0
an - 7
d 4
ov
er
-
24
25
-1
9
20
15
10
-1
4
0
Urban
Rural
Source: Central Bureau of Statistics, 2008 census.
65 Nom ad
3.1.4. Summary
In 2008, Republic of Sudan had a population of 30.9 million with an annual growth rate
of 2.4 percent. High adjusted fertility rate of 5.5 and a huge population in the
reproductive age, this will accelerate population doubling in 29 years; However, we need
to increase the percent of population economically active and this can only be achieved
by reducing the young age dependency ratio that need to raise the contraceptive
prevalence rate.
The uneven distribution of population has led to a high disparity in population density in
different states. Khartoum State had the highest density of population as much as 15
times the national average followed by Al-Gazira State.
The absolute volume of inter-state migration increased by 5 times during the last 52
years The volume of life-time migration increased from 3.4 million in 1993 to 3.7
million in 2001. Migration streams were moved towards Khartoum State. Through
ensuring equity in distribution of resources among states, provision of quality heath and
education services in all states, and implementation of rural development strategies we
can mitigate from rural to urban and from state to state migration.
Immigration and net positive migration always show positive signs of development.
Even emigration tends to be beneficial for the country in terms of reducing
unemployment and increasing remittances. Any development strategy in Sudan is bound
to be more successful with a strong component of migration policy integrated with it.
Despite the expansion of education, the proportion of unmarried women in the age
groups (12-14) and (15-19) was lower in 2008 census compared to the 1993 census and
in Safe Motherhood Survey (1999). Identification of a legal age of marriage is needed to
avoid early marriage.
Males formed greater proportions of economically active population than females, also
the percent employed is high among males compared to females; narrowing gender gab
in this regard is recommended.
3.2. SEXUAL AND REPRODUCTIVE HEALTH
This section aims to provide up-to-date information on the current situation in Sudan, and
an integrated appraisal of the reproductive health and HIV/AIDs dynamics, highlighting
the contribution of poverty, inequality and development linkages. It intends to reflect on
66 emerging issues of significance to future planning and the various opportunities and
challenges to development interventions.
3.2.1. Background
The Government of Sudan, through the Federal Ministry of Health, has defined
reproductive health as a high priority to improve family health status; the issue of
HIV/AIDS is also high on the national agenda and is receiving significant, though not
adequate, attention. Nevertheless, the present indicators show that there is a lot to be done
in the country to improve the situation and achieve the set MDG targets, requiring
concerted efforts not only from the FMOH but from all concerned parties and stakeholders.
3.2.2. Sudan health system
According to a health facility mapping conducted in 2008, about one quarter of the
population has absolutely no access to health facilities; moreover, this figure masks the
huge discrepancies between states as well as within the individual states. Physical
accessibility to PHC facilities varies from 1:3,039 people in the Northern State to 1: 20,779
people in South Darfur; the national average is 1:6,816 compared to the planned 1:5,000
population. Disaggregate data also shows that there are 5.2 hospitals and 246 hospital beds
per 100,000 people in the Northern state compared to 0.2 hospitals and 14 beds per
100,000 in South Darfur. The more recent 2010 Health facility mapping reveals that only
19 % of PHC facilities provide the PHC Minimum Package of treatment of common
diseases.
The table below reflects the types and numbers of health, as well as functionality and
population coverage (2009).
Table 3.2.1. Health Facilities by Type and Number
Facility type
Total
Functional
333
318
Rural hospitals
1892
1365
Health centers
2307
2077
PHC units
Source: Heath Facility Mapping, FMOH, 2008
3.2.2.1. Health system support
Population served
100,000 - 250,000
10,000 - 20,000
5000 - 10 000
3.2.2.1.1. Human resources
With a density of medical doctors, nurses and midwives of 1.23 per 1000 population,
Sudan is still within the critical shortage zone according to the WHO benchmark of 2.28
health care professionals per 1000 population (WHO report, 2006). The career structure,
incentives regimen, and mechanism for retention and equitable deployment of health staff
in rural and underserved areas are not well developed; nearly 70 % of health workforce are
living in urban settings, the bias being more acute for specialized cadres.
The Academy of Health Sciences (AHS), a degree awarding body, has been established for
training nurses, medical assistants, midwives and other allied health professions in order to
67 restore the skill mix imbalance in the country. Meanwhile, in-service training is being
addressed through national and state CPDs. A national human resources for health
observatory (NHRHO) was established in 2007, its impact on human resource management
yet to be seen.
The high turnover and low motivation of staff is impacts on the delivery of RH and
HIV/AIDS services, especially in sites outside the major cities resulting in the need for
continuous training of personnel as new staff members are recruited. Unless this is
addressed in earnest, this is likely to affect the strategies proposed for EmONC, PMTCT,
STI, HIV/TB and ART in the RH Roadmap and new HIV/AIDS strategic plan.
3.2.2.1.2. Supply system
The recent RHCS situation analysis (2011) revealed that despite the presence of a budget
line for reproductive health, there is however, no line item for RH commodities, while the
amount budgeted for RH is relatively small. Because the RH component of Sudan’s health
system lacks reliable data on supply, consumption and demand generation efforts, accurate
forecasting for procurement is not possible. With regards to commodities supporting
HIV/AIDS interventions; during the previous year (2010) condom distribution was
seriously affected by out-of-stock incidence. There are also problems related to ensuring
continuity of ART and PMTCT supplies, while reagents needed for STIs laboratory
confirmation constitute a serious challenge. The supply system for SNAP has been
supported through the global fund, while the RH commodity security (RHCS) committee
that was established in 2009 is now actively working to support supply management for
RH commodities. All contraceptives, except female condoms, are included in the national
EDL. UNFPA is considered the sole provider of free FP commodities to Sudan.
3.2.2.1.3. Information system
Like many other countries in sub-Saharan Africa, Sudan does not have a complete, reliable
and accurate vital registration system; the fragmented health information system hardly
caters for data management. This problem has necessitated the use of surveys and
population censuses to collect data on major morbidity and mortality trends. The
introduction of maternal death reviews since 2009 has generated in-depth information on
key determinants of maternal health, but is as yet far from being complete, hindered by
under-reporting of maternal deaths as well as absence of data on live births. The stigma
surrounding HIV/AIDS is reflected in the figures for register HIV patients, far below the
anticipated magnitude.
3.2.3. Reproductive health
3.2.3.1. Reproductive health indicators
The regional disparities in access to RH services impact mostly on the disadvantaged and
vulnerable groups, such as those living in extreme poverty or remote or peri-urban areas.
The current data shows that maternal mortality has reduced to 216 per 100,000 live births;
a promising unforeseen finding but still far from the set target of achieving universal access
to RH services.
68 The following table shows key RH indicators as per the two rounds of the SHHS, 2006 and
2010. However-as mentioned previously- interpretation of the MMR figures should be
undertaken carefully, since the different methodologies and geographical coverage in the
two surveys leave no room for comparison or establishment of trends. On the other hand,
the 2008 Census data has provided an intermediate figure of 448 per 100,000 live births.
Reducing MM necessitates exploring and addressing its real causes. Several international
studies, especially in developing countries have proved that the main causes of MM are
hemorrhage, sepsis, pregnancy induced hypertension, abortions and obstructed labor.
National data on maternal deaths is now being augmented by the findings from maternal
death reviews, its findings (June 2011 Report) showing that the situation in Sudan is not
much different- hemorrhage (19.9 %) is the number one cause, while jaundice materialized
as the commonest indirect cause of death (18 %).
Table 3.2.2.: Reproductive Health Indicators, 2006 and 2010
INDICATOR
SHHS 2006
Maternal Mortality Ratio
638/100,000 LB
Neonatal Mortality Ratio
39/1000 LB
Skilled Birth Attendance
58.1%
Contraceptive Prevalence Rate
8.45%
Unmet
Need for Family
7.02%
Planning
Midwifery Coverage
49% (NRHP report)
Antenatal care
71%
Post natal care
18%
Fertility Rate
5.9
Home Deliveries
76.1%
C/S Rate
4.5%
Sources: SHHS, 2006, 2010 NRHP Annual report 2010.
SHHS 2010
216/ 100.000 LB
33/1000 LB
72.5%
9%
28.9%
58% (NRHP report)
74%
NA
5.7
76%
6.6%
Fertility rate does not seem to have dropped considerably (5.9 to 5.7), despite the census
documenting a very dissimilar figure of 3.9. The risks to young Sudanese girls associated
with early sexual activity and childbearing are evidenced by SHHS 2010 data which shows
that 16.3 % of women age 15-19 have begun childbearing and an additional 1.2 % have
had a live birth before age 15; 14 % of women aged 20-24 have had a live birth before age
18. These early childbearing patterns were significantly more prevalent among rural,
69 uneducated women of low socioeconomic status, being highest in Blue Nile state and
lowest in Northern state.
3.2.3.2. Policy perspectives
As a strategic intervention, and as an evidence of government‘s commitment to maternal
and neonatal health, Sudan recently launched the National Reproductive Health Policy,
2010 which envisions " a quality reproductive and sexual life for all women, men,
adolescent young children and the elderly". The endorsed policy draws on the existing
national policies and strategies, national and international commitments. It also sets an
agenda for health system reforms assuring that reproductive health services are available
not only throughout a woman’s life-cycle- ensuring her the right to survive pregnancy and
childbirth and enjoy a good family life- but also to their partnering men, adolescent and
youth and the elderly. This visualization is in line with the provisions of the national
constitution, as enunciated in article 32(4) as, ‘the State shall provide maternity and child
care and medical care for pregnant women’. It acknowledges the multi-dimensional
perspectives that surround RH issues; the impact of other MDG focus areas, including
poverty and education; and cultural barriers and perceptions that are impacting on
accessibility to services, especially among rural populations. The policy succeeding in
bringing several priority issues into focus; delegation of FP services to midlevel providers
(medical assistants and midwives), and the use of appropriate technology where relevant
(manual vacuum aspiration for post abortion care, magnesium sulphate for eclampsia, and
misoprostol for post partum hemorrhage); however, policy implementation is far from
being institutionalized.
The commitment and responsiveness of the government to RH policies is indicated by:
In 2001, all states ministers of health and the Federal minister signed the Sudan
Declaration as a spotlight country for the Making Pregnancy Safer Initiative, with the
main target of providing a midwife for every village.
A National Higher Committees for Maternal Mortality Reduction, with similar state
bodies, was established in (2007) to support the health planning, decision-making,
policy advocacy and dialogue with Government and partners at all levels. Despite a
strong start, coupled with remarkable achievement on the part of these committees in
some states (Gedarif, White Nile), sustaining engagement and functionality of these
committees has generally not been successful.
The National Road Map for Maternal and Neonatal Mortality Reduction was endorsed
in 2010, aiming at harnessing all resources into one national plan. Recently costed in
2011, the road map provides guidance at both national and state level on the priority
interventions for reducing maternal mortality in Sudan.
A National Strategy for Scaling up Midwifery in Sudan was developed and endorsed
on the International Day of the Midwife (15th May 2009).
70 June 2009 witnessed the issuance of a Ministerial Decree for mandatory notification
and surveillance of maternal death, reflecting an increasing political and resources
commitment to tracking maternal deaths in the country.
In an effort towards reducing barriers to accessing emergency services, Sudan adopted
a free caesarean section policy in 2008 aiming at improving utilization and quality of
care with emphasis on making life-saving care free.
The development of the National RH Communication Strategy, undertaken in 2008,
was considered for addressing the crucial component of appropriate awareness raising
and advocacy for RH.
Advocacy interventions have received great attention over the last few years in terms
of sensitization meetings with various parties; annual celebration of Mother's Day and
Safe Motherhood Day in high mortality states; development and dissemination of
advocacy packages; advocacy meetings at state level to support introduction and
implementation of MDRs. Although successful commitments have been realized in
some states, they are yet to be translated into adequate pooling of the needed
resources.
Production of evidence based data to inform policies and support decision-making has been
given due consideration, but not enough to fill the gap in information. Several national and
sub-national studies have been conducted; including a national EmOC needs assessment
(2005), socio-cultural study on barriers to FP (2009), and RH situational analysis in 7 states
(2008).
3.2.3.3. Reproductive health services
Expansion of quality RH services has been addressed through various interventions
pertaining to the different RH components, detailed below. Issues related to some RH
components, such as youth health, FGM, and early marriage, are addressed elsewhere in
this report.
Great attention has been given to capacity building of the various levels of care providers
to enable them to provide their respective levels of care. Quality of service provision has
also been addressed through the development of service standards and guidelines; the real
challenge however remains in translating them into services reaching the needy women and
children. Intense awareness raising efforts were exerted through the development of IEC
material addressing the various RH issues, as well as via national and local broadcasting
media in the different states, in order to address cultures barriers to RH, and to promote the
role of communities.
3.2.3.3.1. Skilled birth attendance
Global data shows that three quarters of all maternal deaths occur during delivery and the
immediate post-partum period, such that the single most critical intervention for safe
71 motherhood is to ensure a competent health worker with midwifery skills is present at
every birth, complemented by appropriate referral care to cater for emergencies.
Data from SHHS 2010 shows that VMWS have assisted one-half of all births (49.3 %) in
the two years preceding the survey, out of a total 72.5 % delivery assisted by trained
personnel; it is noteworthy that 20.3 % were delivered by traditional birth attendants.
Mothers who were rich, educated, and living in urban areas are more likely than those
living in rural areas to have delivered with the assistance of a trained attendant, figures
being highest in Northern State (96.7 %) and lowest in West Darfur State (33.4 %).
The reopening of midwifery schools across the country during the past ten years has
provided reasonable expansion in the village midwives training programme; yet, more
input is needed to allow these schools to work at their full potential to produce adequate
graduates to cover this vast country. The lack of standardized curricula in these schools has
greatly affected the quality of training provided.
Sudan's unique feature is the presence of these nearly 16,000 village midwives who have
attended these schools and received one year training in midwifery, providing delivery
services at the community level. Assessment of the training curricula used for the training
of these village midwives has revealed that it does not level up to the international standard
required for skilled birth attendants, as per the definitions given by WHO and International
Confederation of Midwives (ICM). However, the preliminary results of the recent VMWs
assessment (October 2011) done by UNFPA has shown that schools are increasingly
attracting younger and more educated women, which will obviously enhance the social
image of midwifery.
Despite the large number of graduate midwives all over the country, they do not achieve
the standard WHO coverage of one midwife for every 2,000 population, let alone Sudan's
target of availing one for every village. The prevailing distribution pattern of midwives in
all states is urban-based, which makes coverage of the rural underserved areas remain low;
SHHS 2010 data shows that 72.5 % of births were attended by a trained care provider, with
76 % of deliveries taking place within the home.
Further development in the curriculum towards achieving skilled birth attendant standards
has been undertaken to improve the quality of midwifery training and service, taking two
paths. The newly developed two-year curriculum is currently being implemented in 7
schools with the vision of its expansion to cover all midwifery schools in Sudan,
functioning through the Academy for Health Science; regrettably, this diploma programme
will graduate VMWs with greater capacities but who are still incapable of providing basic
EmOC.
Another recently initiated midwifery programme is the BSc programme, initiated in
October 2009 in Omdurman Midwifery School, enrolling secondary school graduates.
Since the pre-requisite for admission to the latter training of professional midwives is
possession of a secondary school certificate, again limiting the chances for candidates from
rural areas who most likely do not meet such a criterion for admission. Thus the Ministry
72 aims to gradually phase-out the original one year curriculum, such that all three cadres will
be concomitantly available in the coming phase. Isolated initiatives for midwifery training
have started in some universities, but such schemes require greater coordination with the
AHS and MOHE to succeed.
Despite varying degrees of inputs by donors, almost all schools are still in need of basic
rehabilitation, skills labs, and continuous training of staff in order to implement these new
curricula. Un-clarity of roles on each of the RH programme and AHS, in addition to the
fluctuating national commitment to supporting midwifery training financially, gives no
clue to what extent the government is willing to invest in midwifery. There is thus a need
to establish more partnerships to bridge the technical and resource gap.
In addition to this, the in-service trainings delivered to VMWs on life-saving skills have
greatly contributed to the improvement of community-based midwifery services, but may
need restructuring to give added value. JICA's (Japanese International Cooperation
Agency) Mother Nile Initiative of providing training and regular supportive supervision to
all midwives in Sennar & Darfur is a success story, ready to be replicated.
A key problem related to midwifery is the high proportion of midwives who are not
employed, despite initiates on the part of some states, such as Gedarif, North Darfur, and
Sennar, by absorbing these midwifes in to civil service, or providing them with
consumables to link them with the system. Non-registration of VMWs is also an issue,
despite efforts for establishment of a guiding midwifery association and council over the
last two years. Local initiatives undertaken to address this- as well as to support referral- is
the idea of donkey-driven carts (as a form of local ambulance) in Gedarif and Kassala
states, supported by DKT and UNFPA. However, effectiveness of such innovation is still
to be evaluated, despite showing impact in facilitating referral of complicated cases, and
providing extra income for VMWs and thus retaining them within their communities.
3.2.3.3.2. Emergency obstetric & neonatal care (EmONC)
The importance of facility care in Sudan lies mainly in its complementarity to the homebased delivery care (when the need arises) that is favored by most Sudanese women.
Findings from SHHS 2010 indicate that about 20.5 % of births in Sudan delivered in a
health facility, the vast majority (19.6 % of total) occurring in hospitals, and skewed
towards urban women. Again, women with higher levels of educational attainment and
belonging to the higher wealth quintiles were more likely to deliver in a health facility.
Northern State had the highest proportion of institutional deliveries (50.6 %), followed by
Khartoum State (48.4 %), while North Darfur State has the lowest proportion (6.4 %).
During the period 2008-09, government supported the provision of 108 ambulances and
EmONC equipment to 29 target hospitals, raising EmONC coverage to reach 79 %.
However, the 2010 FMOH mapping suggests that 66 % and 46 % of facilities provide
Basic EmONC and Comprehensive CEmONC respectively. However, this FMOH data
may not have taken WHO standards into account, where one CEmONC facility is needed
for every 500,000 population, and is not expected to be available in each setup. Barriers to
EmONC provision are namely the high turnover in EmONC trained providers; thus despite
73 its 28 medical schools and high number of graduating doctors, Sudan suffers from severe
shortage of doctors capable of providing EmONC at rural levels.
The ministerial decree for implementation of maternal death reviews (MDRs) covers both
hospital and community level maternal deaths. The process is supported by both federal
and state committees to respond to findings with appropriate policy and interventional
measures. A total of 957 maternal deaths were reported in 2010, over 60 % of them deaths
due to direct obstetric causes. Over two thirds (68.6 %) were critically ill at the time
admission suggesting delays in decision making and physical/economic access constraints.
During the first half of 2011, 386 deaths were reported from all over the country, the
reviewing committees classifying 61 % of them as 'avoidable death". However, the
reported figures may well be only the tip of the iceberg due to grossly underreported
maternal deaths and/or those incorrectly attributed and classified due to other causes. The
MDRs results have also shown 3rd stage delay, reflecting inadequacy in EmONC, a fertile
area for intervention.
3.2.3.3.3. Family planning
The RH policy foresees FP as one of the top priorities among its reproductive health issues.
Despite this, the trend in contraceptive prevalence rate is alarming, with a current
Contraceptive Prevalence Rate (CPR) of only 9 % (SHHS 2010). CPR in 2006 was 8.45 %
in the north and 7.7 % nationally, a mere 0.6 % increase from the 1999 figure– and a
decline of almost two %age points since 1989/90.
The most popular method is the pill, used by 6.3 %, followed by injectables (0.9 %) and
IUD (0.5 %). Other methods used include female sterilization, lactational amenorrhea, and
periodic abstinence (0.3 % each), while only 0.1 % used male condom. All in all, about 8.1
% of women reported the use of any modern method while about 0.9 % reported the use of
any traditional method; adolescents were far less likely to use contraception than older
women.
Figure 3.2.1.: Contraceptive Prevalence Rates by state
RH.4: Use of contra ce ption Pe rce nta ge of w ome n a ge 15-49 ye a rs curre ntly
ma rrie d or in union w ho a re using (or w hose pa rtne r is using) a
contra ce ptive me thod, Suda n (North), 2010
21.6
Northe rn
21.3
Kha rtoum
Rive r Nile
16.4
W ite Nile
12.8
9.7
Ge zira
8.7
Ga da rif
Sinna r
7.3
North Kordofa n
6.6
5.8
Re d Se a
4.4
Ka ssa la
W e st Da rfur
4.2
South Kordofa n
3.5
Source: SHHS, 2010
Blue Nile
North Da rfur
South Da rfur
3.0
2.5
2.1
suda n
9.0
.0
5.0
10.0
15.0
20.0
25.0
The 2010 survey shows that the unmet need for contraception is 28.9 %, reflecting poor
access to FP services, especially for rural women; this figure does not even compare with
the previous figure of 7.02 % (SHHS 2006), probably due to greater accuracy in
measurement modalities. Met need for contraception for spacing and limiting were 6.8 %
and 3.3 % respectively, while the %age of demand for contraception satisfied was 25.9 %.
74 All in all, the SHHS 2010 survey data shows that most women who practice family
planning are better-educated, wealthier and urban-based, implying that the needs of poor,
uneducated, rural women are not being met to the same degree. In addition, most women
are being denied ‘choice’, since variety of commodities reported was limited. Given that
rural women have limited access to some contraceptives, and given that there are few
trained personnel with the skills to provide appropriate services, other, longer-term
methods such as the IUD and injectables, need to be made more available and supported.
Additional service delivery problems in the context of FP probably relate to the very
limited spectrum of cadres who provide the services. Doctors in public facilities do not
look upon FP as their role, creating many lost opportunities with clients. There is thus
almost no promotion of service uptake at service delivery channels. The health visitor, who
is counted as the main FP provider, is a cadre that is dying out due to closure of all but one
school that are producing them, and with high numbers going into retirement annually.
Previous policies did not allow midwives to provide the service (only counselling), but the
2010 RH policy gives legitimacy to midwives to provide pills, condoms, and injections.
There is thus a need to benefit from the new roles given to midwives in expanding services
to rural women through these widely available community based-cadres.
On the other hand, facilities providing the service suffer from frequent stock-outs due to
inadequacy of commodities being distributed from the national level, UNFPA being the
only provider of FP commodities to the Ministry of Health with no additional budget line
being provided by the Ministry of Finance. However, expired pills are a common
occurrence in many warehouses across the country. The Sudan family Planning
Association (SFPA) experience of providing subsidized FP commodities does not seem to
have suffered from overstock, thus implying that free distribution is in itself a problem on
underuse. To escalate FP coverage, some states have developed a community-based
distribution modality to increase utilisation of FP services. A rapid assessment done in
Khartoum has reported that IUDs and injectables are not available in most pharmacies. It is
worth mentioning that female condoms are not available (only in Darfur), and emergency
contraception is still unavailable.
Results of the survey that looks into the barriers to FP (2010) has shown that main barriers
to family planning methods plainly articulated by the respondents were pronatalist attitudes
and preference for large families, lack of knowledge and religious beliefs. It also revealed
that the main factors associated with the use of family planning methods are age at first
marriage, education, wealth, husbands’ educational level, knowledge of and attitude
towards family planning methods. Financial barriers accounted for only 18 % of the
population and 40 % lived within walking distance of a service provider. Inadequacy of the
method mix was implied by the lack of diversity in utilized methods, with pills being
preferred by 86 %.
75 3.2.3.3.4. Antenatal & post natal care
According to the Annual Report of the NRHP 2008, antenatal care (ANC) services were
being provided by 45 % of facilities, a substantial increase from the 21 % figure in 2007.
However, there has not been concomitant improvement in the service utilization figures;
the proportion of mothers receiving at least one antenatal care visit has stayed almost static,
not increasing beyond 75 % through the 1990s to 2010 (SHHS). Post-natal care is shown
to have increased from 13 % (SMS1999) to 18 % (SHHS 2006), a proxy indicator from the
%age of women receiving post-partum vitamin A. Ironically, the SHHS 2010 did not
address post natal care, despite it being a crucial intervention for both mother and neonate.
ANC was received at least once by 74.3 % of women aged 15-49 years who gave birth in
the two years preceding the SHHS (2010), being highest in Northern State (88.4 %) and
lowest in Blue Nile State (51.7 %). Antenatal care coverage was higher in urban areas
(84.3 %) than in rural areas (70.4 %), and both the women‘s educational level and
economic level of the household seem to influence the proportion of pregnant women
receiving ANC from qualified personnel. The current provision of specific care provided as
part of the antenatal care package remains quite inadequate, as pertaining to blood pressure
measurement (57.7 %), and blood (55.8 %) and urine testing (56.7 %). SHHS 2010 has for
the first time generated data on the 4 WHO recommended ANC visits; showing that while
almost seven in ten mothers (70 %) receive antenatal care more than once, about half of
mothers received antenatal care at least four times (47.1 %).
3.2.3.3.5. Post abortion care
The concept of post abortion care (PAC) was introduced in Sudan in 2002 to help address
the burden of unsafe abortion on maternal morbidity and mortality. No data is available on
the magnitude and severity of the problem of unsafe abortion; however, complications of
unsafe abortion are seen often in the health facilities and comprise a major proportion of
cases treated. According to the SHHS 2006, 18 % of pregnancies ended in abortion, as
compared to 12.3 % in 1999 (SMS). According to Sudan laws (PC 1991, No. 135- 137),
abortion is allowed only to save a women’s life or within 90 days of pregnancy resulting
from rape. Regardless of legal status, abortions still occur. In Sudan, abortion is a sensitive
issue with religious, cultural and political dimension, and the term PAC, is largely
confused with "provision of illegal abortion" in Sudan. Despite all obstacles, it is being
implemented by the MOH as a key strategy for reducing maternal mortality with the
support of various partners, and major efforts to instill post abortion care (PAC) services
are now underway in Sudan.
PAC started in Sudan as far back as 2002, with development of national guidelines and
protocol for post abortion care. Sporadic trainings were conducted, mainly supported by
UNFPA; however, health facility setup did not support implementation of PAC package.
The NRHP's first experience in establishing a formal public-private partnership was in
favor of PAC implementation, whereby in 2007 an MOU was signed with DKT- a social
marketing company- to support PAC in three states initially. In addition, Sudan Family
76 Planning Association has recently launched an initiative for introducing PAC services into
SFPA clinics into another three states. There is however a need for focus to achieve
success stories and lessons learned prior to expansion to counteract further resistance to
PAC.
Globally, the introduction of a medical treatment option such as misoprostol for PAC has
already been demonstrated to be safe and effective; however, in Sudan, misoprostol is
registered as a controlled drug only for the management of post-partum hemorrhage.
3.2.3.3.6. Obstetric fistula
Obstetric fistula is a common occurrence in rural communities where girls marry at an
early age and where EmONC is inaccessible. The stigma associated with this common RH
morbidity has broken many homes and thrown blameless vulnerable girls into isolation.
Activities in this respect were supported by Abbo Fistula Treatment Centre, the center of
excellence for fistula in Khartoum. Major inputs include rehabilitation and equipping of
Abbo Centre and the establishment of fistula satellite treatment centers in Kassala and
Nyala, in addition to the conduction of fistula campaigns on an almost annual basis.
Indeed, 2009 witnessed the largest ever campaign in Africa whereby 152 cases in Darfur
were managed. Functioning of the fistula centers has been supported via training of
specialist doctors and general practitioners on diagnosis and management of obstetric
fistula, and development of the National Fistula Management Protocol and Guidelines. A
national fistula rehabilitation and social reintegration center has been set up in Khartoum to
house fistula patients and provide counseling and vocational training to survivors.
3.2.4. HIV/AIDS and sexually transmitted infections
With the end of the National HIV/AIDs Strategic Plan 2004-2009, the situation analysis
that was conducted to inform the new planning cycle reflects a new picture of Sudan's
HIV/AIDS epidemic. Likewise, incoming information from the Sudan Household Health
Survey 2010, ANC sentinel sero-surveillance surveys, and bio-behavioural survey among
female sex workers (FSW) and men having sex with men (MSM) have all provided further
clarity to the situation. From a generalized epidemic with prevalence of 1.6 %, the data
now reflects a concentrated/low prevalence epidemic of 0.67 % among the general
population and a more concentrated epidemic among the Most at Risk Population
(MARPs). In line with these findings, SNAP has started placing particular emphasis on
most at risk populations groups, namely FSW, their clients and MSM.
MARPS include FSWs, 85 % of whom are unmarried women, half of them divorced and
having an average of 3.2 dependents. In Gezira state, data showed 52 % of FSWs to be
married, highlighting the risk of HIV transmission within marriage. Their clients come
from different social categories, including armed forces, public officials, businessmen,
youth, truck drivers, migrant workers, and traders. Behavioral data has also shown that
about 25 % of MSMs are married and 50 % have sex with women. The MSM population is
heterogeneous and has a high level of interaction with the general population. Thus the
77 prevention of HIV transmission among the both groups is a key strategy for minimizing the
spread of the virus into the general population.
The main determinants of the spread of HIV/AIDs among the MARPS and vulnerable
groups include the low knowledge regarding the disease, and the risky behavior in which
they indulge. Likewise, the high population movements as a result of the conflicts in the
various parts of the country have contributed to the population vulnerability to HIV
through violence, forced displacement; break down in the rule of law, and economic
destitution, leaving entire populations at risk for HIV.
3.2.4.1. HIV/AIDS indicators
Current data estimate an expected gradual increase in HIV prevalence to reach 1.12 % by
2015; these projections show that an estimated 15,472 will require ART while 5,843
mothers need to be addressed with PMTCT. Data from the estimation and projection for
this reporting period (2009), the total number of adults and children living with HIV was
about 122,216, comprising 117,109 adults, 67,661 women, and 5,107 children (ages 0-14).
There are currently 27,888 AIDS orphans (ages 0-17) living with HIV and AIDS. Thus
despite the low HIV prevalence, the potential for slow growth over the next five years
remains a possibility.
3.2.4.2. HIV/AIDS policy perspectives
The 2010-vision for SNAP "to build HIV/AIDS-free Sudan" will be achieved through
ensuring provision of equitable and high quality services that meet the expectations and
needs of Sudanese people, and by putting HIV/AIDS/STIs interventions among the top
priorities of the country development policy, using the best available evidence and efficient
utilization of resources.
The response to AIDS in Sudan is multi‐sectoral and decentralized, coordinated by Sudan
National AIDS Programme (SNAP), with the involvement of other line ministries (General
education, higher education, defense, interior, guidance and endowment, youth and social
welfare). SNAP has strengthened decentralized response by deploying additional human
resources particularly in the area of surveillance and M&E at the state level and efforts are
being continued to strengthen the response at the lower levels.
Sudan‘s national policy on HIV\AIDS was launched in 2004. The first major effort to
develop a strategic plan based on epidemiological and behavioral grounds was in late 2002
when the Government undertook a comprehensive situation and response analysis. This
formed the basis for an evidenced-based National Strategic Plan for 2003-07, and was
followed by the National Multi-sectoral Strategic Plan 2004-2009. A legislation/Act was
drafted to protect the rights of PLHIV and other vulnerable population groups, but this Act
is still awaiting final approval from Ministry of Justice.
78 SNAP has recently developed and endorsed its second strategic plan for 2010‐14 (NSP II);
while the previous NSP (2004‐9) focused in maintaining the prevalence of HIV at less than
2 % in the general population, the new one prioritizes and targets most‐at‐risk population
by ensuring that HIV interventions are evidence based.
3.2.4.3. HIV/AIDS programming
The main focus of the HIV/AIDS control programme (SNAP) has been on provision of
counseling and testing, PMTCT and ART services, treatment and control services for
sexually transmitted infections (STIs), awareness-raising for communities, advocacy for
involvement of all sectors in the national response, provision of services to MARPs and
Monitoring and Evaluation (M&E). In the area of capacity building, SNAP has trained
service providers, journalists, students, MARPS, and PLHIV on relevant issues.
Mainstreaming efforts are evident in the education sector (both Ministries of General and
Higher Education) where an HIV curriculum has been developed and teachers trained. This
integration is also apparent in the Ministry of Guidance where special modules have been
developed to train religious leaders, delivering messages through sermons and the media.
Efforts to reduce stigma accelerated through sustained advocacy, mass media
communication and legal reform have been led by the Ministry of Justice. In all 15
northern states PLHIV associations have been established; with assistance from SNAP
federal and state programmes and UNDP utilizing Global fund resources.
Priority interventions include prevention programmes targeting general population with
increased number of VCT, and PMTCT sites, condom distribution outlets, and increased
production and distribution of BCC/IEC materials. The most‐at‐risk populations were
reached through outreach services including VCT, peer education, condom distribution and
mapping and bio‐behavioral researches conducted. Care and treatment programme has
expanded in all states with increased number of ART and TB/HIV centers, nutritional
support for PLHIV and their families and empowering PLHIV associations.
Most-at-risk-population modules have been updated and HIV/AIDS guidelines developed
for higher education institutes in collaboration with the Ministry of Higher Education and
Gezira University, with concomitant establishments of 28 AIDS programmes in higher
education institutes and timely training of their coordinators. Likewise, 10 educational
modules on HIV/AIDS for youth have been developed. Despite updating of the homebased care guidelines, the number of achieved annual home visits is fluctuant and still far
from the annual targets.
3.2.4.4. HIV/AIDS services
The overall prevalence still remains low partly due to many factors, namely conservative
cultural norms among communities that contribute to slow the spread of HIV, augmented
by the almost universal male circumcision in Sudan. However, the high population
79 mobility due to rural-urban migration, displacement and armed conflict are few of the
prevailing circumstances that are silently threatening the country of an increasing risk of
HIV/AIDS spread in Sudan.
3.2.4.4.1. HIV/AIDS prevention services
Condom use remains a key measure for HIV prevention. However, condom distribution is
a culturally sensitive issue, thus limiting the availability of condoms and created psychosocial barriers to their use. Even when condoms are available, they are looked upon as a
contraceptive commodity only and not a measure for HIV prevention, while the perception
that condom use reduces sexual pleasure prevails. Data regarding condom use at last high
risk sex is lacking; however, it is noteworthy that more than 5 million condoms were given
out through free distribution in 2008.
The expansion of HIV counseling and testing services over the last five years has shown an
increase from only 34 centers in (2006) to 138 centers nationwide at the end of 2010. 28,758
persons received HIV counseling and testing, out of whom 8.6 % were found to be HIV
positive. In addition, 3995 people received HIV counseling and testing through mobile HCT.
Figure 3.2.2.: Health Facilities Providing Testing & Counseling- 2006-2010
Source: SNAP Annual Report 2010
The vast majority of VCTs are in public facilities, with only 3 being run by NGOs, with
absolutely no involvement of the private sector in VCT service provision. However, the
current utilization rates are very low, the majority being men, highlighting the limited
capacity of women to access information, as well as the socio-cultural norms that relatively
restrict mobility of women, stigma, and the economic difficulties. It is estimated that out of
the 2.5 million people targeted for HIV testing; only 2.8 % have been reached. Provider
Initiated Testing and Counseling (PITC) and outreach counseling and testing, have been
introduced to improve access to counseling and testing services in Sudan.
A communication strategy was developed in 2006, aiming at providing information,
education and communication on HIV to the general population. HIV education activities
have been implemented targeting the media, most-at-risk and vulnerable populations
80 particularly truck drivers, prison inmates, female sex workers and their clients and uniformed
forces. HIV education has also been included in the school curriculum since 2007.
Awareness-raising has also been addressed through the initiation of the HIV/AIDS hotline
and information center, production of various TV spots and documentaries, and production
of a regular newsletter. The SHHS 2010 data shows that less than 60 % of women in child
bearing age know the fact that a woman can transmit the disease to her child, while but only
one tenth of that number have comprehensive knowledge regarding HIV/AIDS. State
experiences have given greater insight and lessons learned; interventions through educating
staff of state radio and TV in delivering messages in local dialects proved to be attractive for
the target audience.
PMTCT in Sudan started as a pilot project in 2005, initially implemented in four states.
Since 2007, PMTCT services have been expanded from 7 sites in 2007 to reach 38 sites
(2010); the aim of this expansion was to increase access of pregnant women to these services
in all states. A total of 194,118 women received general awareness sessions, out of which
47,172 pregnant women were tested for HIV; 110 HIV positive cases were identified, out of
an estimated 7,865 HIV positive pregnant women in need of PMTCT services (1.4 %). The
average HIV prevalence rate among pregnant women attending antenatal care (ANC) in
2007 is 0.19 %- an average of 0.33 % in rural sites; 0.14 % urban sites, 0.26 % among IDPs
pregnant women.
During 2010 major efforts have been made to integrate PMTCT interventions with the RH
programme, with joint revision and updating of the National PMTCT guidelines. However,
the concept of linkage and integration is still new and is challenged by the currently existent
verticality of RH and AIDS programmes. Un-clarity of the roles of the two concerned
programmes in addition to the presence of multiple technical bodies causes duplication,
hindered further by the absence of routine supervision to PMTCT pilot sites and the nonexistent preparedness of the logistic system for integration of services.
3.2.4.4.2 HIV/AIDS treatment services
The first ART adult and pediatrics' guideline were developed in 2006 and updated in 2008;
services have rapidly expanded over the last five years, such that facilities providing ART
services increased from 12 to 32 in all states in 2010, mostly located at tertiary and
secondary hospitals. CD4 machines have been installed in all ART sites and viral load
machines are located in reference laboratories. Training of health personnel in HIV treatment
and care is also on-going against the backdrop of high staff turnover and low motivation of
staff to work in rural areas. The country has adopted a policy of providing free ART services
to PLHIV but the patients have to meet the cost of admission and other HIV/AIDS related
illnesses.
Thus the number of HIV patients ever started on ART increased to 4316, of which 2185 are
currently on ART. This year (2011) 1047 HIV patients have started ART. About 1,996
patients (13.12 %) are currently on ART out of a total of 15,210 PLHIV in need of the
81 service. There is, however, inadequate information on what the programme is doing to
reduce the side effects of these drugs. Blood safety has been targeted through the 375 blood
banks and 9 reference laboratories which undertake mandatory screening for all donated
blood; 2010 reports reflect that out of 56178 blood units donated and screened for HIV, 260
were found to be HIV positive. To reduce the burden of HIV on TB, the two concerned
programmes jointly develop TB/HIV guidelines in 2009. Currently provider initiated
counseling and testing have been intensified in most public health facilities, which have
improved HIV screening among TB patients.
Figure 3.2.3.: Numbers of TB Centers and Patients Tested For HIV 2007-2010
Source: SNAP Annual Report 2010
3.2.4.5. Sexually transmitted infections
Management of STIs has received its share of achievements with updating of STIs
monitoring tools, capacity building of medical staff, and dissemination of 1800 copies of STI
training modules in both Arabic and English languages. A TWG for STIs prevention and
control has been established to provide technical backup.
According to survey conducted by MOH and UNFPA in 2008, the vast majority of assessed
facilities reported practicing syndromic management of STIs (treatment based on
standardized patient signs and symptoms). Services that include diagnosis (syndromic or
laboratory-based) and treatment of STIs were available in 72 % of facilities, and partner
notification was encouraged in 55 % of sites. While condoms were available at 83 % of
facilities and IEC materials in 64 %, promotion of safe sex was not evident.
Current data on syphilis is rather small scale and does not give a clear picture; the overall
prevalence of syphilis has been documented as 3.5 % (2007), while ANC sentinel
surveillance data in Sudan showed alarming Syphilis rates of up to 14 % using RPR kits
during the same period.
82 3.2.5. Challenges in meeting RH & HIV/AIDS targets
RH is a very controversial issue for Sudan, often linked to cultural myths and religious
beliefs, with wide spread misinformation among the general public in regard to RH
options.
Despite both HIV prevention and maternal mortality being high on Sudan's agenda, there
is need for translation of this commitment into the necessary financial and human
resources to implement the high-cost but high-return investments for RH related
strategies and policies currently in place, effectively and efficiently, irrespective of other
competing priorities.
The constraint of the poorly functioning health systems and weak referral systems is more
acutely felt when it comes to obstetric and neonatal emergencies.
Programmeming is not systematically driven by evidence, further compounded by underutilization of survey findings and resistance to introduction of global development issues
and initiation of new effective technologies.
Family planning commodities face frequent stock outs and during the previous year
(2010) SNAP's condom distribution programme was seriously affected by out-of-stock
incidents. Nevertheless, problems related to logistics or management of drugs, family
planning commodities and equipment are all not well captured due to poor information
flow within the system.
Midwifery is hampered by the low literacy level of the enrolled midwives, and the
training process suffers from shortage of educational equipment and supplies in the
midwifery schools, coupled to lack of accredited trainers to teach the new curricula.
The knowledge gap within communities and families is a major challenge in all RH
perspectives and hinders efforts to increase access to services.
The high population mobility due to rural- urban migration, displacement and armed
conflict are major factors that increase the risk of HIV/AIDS spread.
Stigma constitutes the most important obstacle to an effective and efficient HIV/AIDS
programme, while public silence acts as a suitable environment for propagating the virus.
There is very limited data on condom promotion and distribution suggesting that
advocacy and prevention activities remain limited, a factor that further plays down the
seriousness of the epidemic.
Involvement of both national programmes (RH and SNAP) in implementation, despite
their core mandate being coordination of RH interventions and the national HIV response
respectively. This is generally due to the weak capacity of NGOs or state level impending
partners.
Coordination mechanisms both within and outside the health system need to be
strengthened.
3.2.6. Opportunities for RH & HIV/AIDS service expansion
83 Both maternal mortality and HIV/AIDs have risen high on Sudan's development agenda,
an opportunity that should be exploited to the fullest extent possible in order to translate
the commitment into resources.
The availability of updated data on RH and HIV that can effectively guide planning as
well as serving as a tool for advocacy.
There is currently remarkable progress in the efforts for integration between HIV/AIDS
and RH- though not enough- indicated by integrated efforts for PMTCT implementation,
joint production of IEC materials and execution of community related sensitization
seminars.
The establishment of strategic partnerships and networks with community-based
structures (i.e. CBOs and NGOs) across the country working on RH issues can be
instrumental in extending the outreach and nurturing efforts towards awareness-raising
and social change.
Neighboring countries such as Ethiopia have good practices that can be adapted to Sudan
context.
3.2.7. Humanitarian concerns
3.2.7.1. Emergency programmeming
Sudan as a country is inflicted with both acute and chronic emergencies including floods,
spontaneous displacement and returnees, and population movements between North and
South Sudan. These conditions of unsettlement contribute to the RH risks and vulnerability
of affected women.
The Minimum Initial Services Package (MISP), is a package of RH services and equipment
provided in case of emergencies, critical for RH and prevention and response to GBV,
originally initiated in Darfur in 2005. It is designed to prevent excess neonatal and maternal
morbidity and mortality; reduce HIV transmission; prevent and manage the consequences of
sexual violence; and plan for comprehensive reproductive health services. Capacity building
interventions have addressed the establishment of a core team of trainers for MISP and
subsequent state trainings, as well as the training on emergency preparedness which targeted
RH coordinators and health managers across states. Major efforts have been exerted in
annual contingency planning, and procurement and prepositioning emergency RH
equipment, supplies and medicines in the 5 states. RH emergency kits and hygiene/dignity
kits have been delivered timely to border states (White Nile, South Kordofan and Blue Nile)
in preparation for the Sudan Referendum. Transporting commodities to and within states
often faces serious obstacles from local authorities, often delaying delivery of timely
support.
Over the past three years training of health providers on Clinical Management of Rape
(CMR) for survivors has received greater attention, expanding it beyond Darfur to include
other states; however, the complementary dispensing of emergency contraception is not
permitted in these states, despite the fact that care providers all over Sudan are being trained
84 to use them as part of the CMR package. Moreover, work in this respect is greatly hindered
by the issue of Criminal Form 8, which prevents the delivery of prompt service to survivors.
Circular 2, which waives Form 8 and legalizes the delivery of immediate serviceseliminating the need for Form 8- has been operational in Darfur, and after major efforts
expanded to all states removing barriers to services; unfortunately, most care providers are
unaware of the fact.
Challenges also include the non-supportive attitudes of stakeholders and state authorities for
RH interventions especially GBV and FP. The increasing knowledge gap that is now
becoming apparent between IDPs and host communities due to greater focus on the former
group have brought forth issues of inequity, thus highlighting the need to direct attention to
the latter group. There is- as yet- no focus on the 5th MISP component for comprehensive
planning and shift from emergency to recovery; moreover, after the separation, new
additional states, such as Blue Nile and South Kordofan, have emerged as crisis states that
will require direct support as part of the humanitarian response of donor agencies working in
the country.
Prevention of HIV/AIDS as the third objective in MISP for RH in conflict has been
addressed through ensuring universal precaution and infection prevention control in all
facilities (trainings of different categories of staff, and equipping health facilities); condom
distribution; safe blood transfusion (equipping facilities, training relevant cadres, and
renovating blood banks).
3.2.7.2. DDR
The Disarmament, Demobilization and Reintegration (DDR) processes, launched in 2007,
originally came out of the overall CPA implementation process, to support the transition of
ex-combatants (XCs) and associated members from military to productive civilian life,
aimed at ensuring a secure, stable and peaceful Sudan. The National DDR Coordination
Council was established by presidential decree to oversee the DDR process at the highest
policy level, supported by implementation bodies in the north and south. The North Sudan
DDR Commission (NSDDRC) leads the design and implementation of DDR in the seven
central sector non-CPA states as well as in Darfur and the East. Joint DDR Commissions
coordinate work in the three CPA areas of Blue Nile, Southern Kordofan and Abyei and
comprise members of both the North and South Commissions.
The interim DR programme is focused on Special Needs Groups (the disabled, women, and
children associated with armed forces and groups) and community security support to help
create an enabling environment for DDR in receiving communities. Later, the 2009-2012
programmes were initiated to target 18,000 XCs and associated members. To ensure the
durable reintegration of XCs, the programme promotes community security and social
cohesion through capacity development at both local and national levels. Furthermore, a
large number of women have also participated in the war either in a combat role or a support
role.
85 By 31 October 2010, a total of 21,588 XCs had been demobilized in Damazin, Julud,
Kadugli and Kauda, 3,200 of them women. Out of this total, 16,617 XCs are under the
various stages of reintegration. The Eastern States DDR programme started early 2007 and
was based on the Eastern Sudan Peace Agreement, serving 1700 former Eastern Front
fighters, 254 children, and only one woman. Albeit the continuing need, the UN support to
the eastern programme was phased out in May 2011. However, less than half of Sudanese
ex-combatants targeted for DDR have been demobilized, and fewer than 9 % of Northern
forces have completed reintegration training, as of January 2011.
Despite meticulous planning and supervision, the programme has suffered many drawbacks
and challenges. In the Eastern project, a major gap was the time lag between DD phase and
R, it being actually much longer than planned, with little input into the latter component and
minimal interventions on HIV/AIDS, GBV and RH. Neither the NSDDRC in Eastern Sudan
nor beneficiaries and/or receiving communities were part of the planning of the programme;
accordingly the local ownership over the DDR process was poor. Despite the long duration
of the project, no comprehensive evaluation of the programme has been done such that it is
not possible to document success of the reintegration process. Inadequate attention was given
to the traditionally marginalized groups, especially women, the disabled, and dependents.
Youth needs have not been addressed in the DDR programme, and the child DDR sponsored
by UNICEF is working in isolation within this overall process.
From the health perspectives, the prevalence of STIs/STDs amongst the WAAFG appears to
be much higher than amongst the community at large, as per the Small Arms Survey (20052008). The data also reflected a critical gap in knowledge regarding HIV among them,
rendering WAAFG particularly vulnerable to reproductive health problems and HIV/AIDS
infection. An average of 70 % of the WAAFG did not know various HIV modes of
transmission and prevention. Domestic violence, sexual harassment, and psychological
complaints have also been documented.
3.2.8. Recommendations:
The analysis of the RH and HIV/AID situation has confirmed improved political concern
for the critical RH issues indicated in policies and strategies and on-going programmes. For
effective results for RH, the implementation of Sudan's Roadmap for Reducing Maternal &
Neonatal Mortality would be an appropriate starting point, needing further breakdown and
focus. The HIV/AIDs component would again be guided by the new 2012-2016 Strategic
Plan for HIV/AIDS.
3.2.8.1. RH Priority Areas
Midwifery: Continued support to implementation of one year curriculum, while
providing infrastructural support for implementation of the new curricula in terms of
micro-curricula development, capacity building of teaching staff, supporting
organizational structures for midwifery, upgrading and equipping VMWs schools,
86 with continuation of advocacy efforts to institutionalize midwifery - support,
salaries, incentives
Family Planning: Capacity building of potential providers, while enhancing MWs
role in FP. Commodity security should be addressed to ensure availability and
choice, with introduction of new methods of FP linked with advocacy &
diversification of partnerships for RHCS. Greater emphasis should be placed on
demand generation through appropriate awareness-raising.
Maternal death reviews: Utilization of findings in designing relevant, cost effective
interventions, while strengthening functionality of MDRs system- reporting
processes at all levels; monitoring of implementation of recommendations. The need
to broaden the circle of involved bodies (implementation bodies, decision making
bodies for resource allocation) including CBS, with awareness creation on the need
for MDRs.
EmONC: Regular updating of EmONC mapping (S&E based on mapping), and
institutionalize of EmONC training at state levels to sustain EmONC providers; this
can be addressed through pre-service training with medical institutions. Greater
attention can be given to neonatal care.
Health system support for RH with major focus on support for harmonizing national
M&E activities, strengthen routine RH information, operations research
(implementation & utilization), and improve logistic management, forecasting etc.
with inputs in the form of technical assistance where needed.
Emergency programmeming: early preparedness and response as part of regular
programmeming, including MISP and CMR, the expansion of strategic
geographical focus with the new context of conflicts to include emerging conflict
states ( Blue Nile, South Kordofan states), and addressing gender perspectives of
DDR interventions.
3.2.8.2. HIV/AIDS Priority Areas:
Increased focus on targeted interventions for population at risk (FSWs, MSMs)
and other vulnerable population groups (tea sellers, military personnel, and
youths in and out of school, truck drivers and populations of humanitarian
concerns).
Geographical focus on regions with higher HIV prevalence as well as
“hotspots” where FSWs and MSMs and populations of humanitarian concern
should be targeted.
HIV prevention should be prioritized through appropriate awareness raising
interventions, addressing determinants affecting utilization of reproductive health
and HIV-prevention services, and promotion of healthy behaviors. Programmes
should be implemented through communities with focus on prevention in women
87 and girls; condom programmeming; and prevention for young people outside
schools and other vulnerable groups.
Intensive public education backed by strong community leadership to break the
relative silence surrounding the HIV situation in Sudan is critical for eliminating
ignorance about the virus.
Strengthening the health system and programme management with particular
focus on generation of strategic information for focused intervention. Quality
improvement across all services and at coordination, managerial and technical
levels is necessary. Priority areas for capacity building include PSM, HIV
surveillance, health systems strengthening and CSOs capacity development.
Establishment and strengthening of linkages with other programmes both
within and outside the health system to ensure provision of a comprehensive
package of services.
Quality improvement: While the programme is sufficiently scaled up but due to
poor quality interventions the efforts might not yield high impact.
88 SECTION 3.3.: GENDER
3.3.1. Gender Equality and Women Empowerment
Looking back decades, it is evident that Sudanese men and women roles and relationships
are changing. There are remarkable improvements in women public participation and
interactions but still gender inequalities persist. The UNDP-HDR (2007/2008) confirmed
that the gender gap indicators for Sudan are high compared to other world regions. The
categories, adult literacy, gross primary enrolment, gross secondary enrolment and female
economic activity rate, indicated in table 3.3.1., demonstrate that the Sudan's performance
falls below the Arab States, Sub Saharan Africa, low income and least developed countries.
Table 3.3.1.: Gender Related Development Index in Sudan Compared to World
Regions, 2006.
Adult
Literacy (age
15 and older)
1995-2005
Gross
Primary
Enrolment
%
2005
Gross
Secondary
Enrolment
%
2005
Female
Economic
Activity Rate
( age 15 and
over) % 2005
F/M
Rate
%
51.8
69.9
F/M
Rate
%
56
104
F/M\
Rate
%
33
58
F/M
Rate
%
23.7
52.4
F/M
Rate
%
0.73
0.91
F/M
Rate
%
0.87
0.94
F/M
Rate
%
0.94
0.93
F/M
Rate
%
33
64
Sudan
Developin
g
Countries
Least
developed
44.3
0.80
90
0.89
28
0.81
61.8
72
countries
59.4
0.88
88
0.90
65
0.92
26.7
34
Arab
States
51.2
0.84
92
0.89
28
0.79
62.6
73
SubSaharan
Africa
86.5
0.99
110
0.97
78
1.01
57.0
72
Middle
Income
48.8
0.82
99
0.91
41
0.82
45.7
55
Low
income
72.7
0.92
104
0.95
64
0.94
52.5
67
World
UNDP,
HDR
2007/2008,
Table
28:
326-329,
Table
30:
334-337,
Table
31:
338Source:
341
89 This section intends to analyze the progress, challenges and opportunities related to gender
equality and women empowerment in the Sudan. The recommendations for way forward
are considered. The analysis is based on two premises: a) women empowerment is the
most effective strategy for closing the gender gaps and achieving gender equality. “To be
empowered women must not only have equal capabilities (such as education and health)
and equal access to resources and opportunities (such as land and employment) but they
must also have the agency to use those rights and capabilities, resources and opportunities
to make strategic choices and decisions ( such as provided through leadership opportunities
and participation in political institutions). To exercise agency women must live without
fear and free of coercion and violence”36 b) gender inequality and women empowerment
opportunities are primarily shaped/influenced by cultural elements in its dynamics with the
political, economic and social developments. Empowered women would be able to access
the information about risks and means of prevention to their RH, exercise their RR and
take decisions concerning their bodies, fertility, and their daughters RH. Thus, empowered
women have better opportunities to improve their maternal health.
3.3.2. Progress towards gender equality
There are gender equality gains in four major areas in Sudan: women’s rights, education,
labor force and political participation.
Rights Acquired: Full suffrage rights for women were adopted in 1965. The rights of equal
pay for equal work and some mothers’ benefits including maternity leave and lactation
hour have been considered in civil service law since 1974. The Law of the National Civil
Service, 2007 maintained the rights acquired by women during the 1970’s. These
include the right to appeal, the right for training; the right to annual leave, right for leave
without pay and leave without pay to accompany spouse,i.e. similar rights as those given to
males37. The women rights of inheritance, marriage and divorce are stipulated according
to Islam, Christianity or other customary laws. The Child Right Act set important rights for
girls and boys. The 2005 Interim Constitution noted the equal rights for men and women.
A gender quota of 25 % was set in Election Law, 2008.
Sudan is party to several global instruments, agreements and frameworks some of which
are of importance to women’s basic rights. These include the International Covenant on
Economic, Social and Cultural Rights; ILO Treaty on Equality on Payment and
Opportunity; International Covenant on Civil and Political Rights; International
Convention on Elimination of All Forms of Racial Discrimination; Convention on the
Rights of the Child; the First Additional Protocol to the Convention on the Rights of the
36
UN Millennium Project, 2005. Taking actions: Achieving Gender Equality and Empowering
Women. Task Force on Education and Gender Equality. London: Earthscan. P 33.
36 See Labor Law, 1974;
37
See Labor Law, 1974;
90 Child. To some extent these international treaties informed laws providing rights to
women. The government is committed to achieving the goals for the Beijing Platform of
Action and MDGs as framework for policies. The National Women Empowerment Policy
focused on six areas from Beijing Platform of Action to achieve MDG 3.
The progress made towards women rights has transpired over a long period of time and
came as a result of women movement demands for these rights. The international treaties
spurred progress in securing formal rights for women.
Progress in Education: Women outnumber men in literacy classes: It is observed, in Table
3.3.2., that there is an increase in literacy rate for males and females of all ages, in urban
and rural areas in the period of 1993 and 2008. The statistics of FMoE for year 2008-2009
indicated women constitute 82% of participants in adult literacy classes in the Sudan and
this is an important achievement considering that illiteracy is higher among women. The
efforts for women literacy is also evident in Kassala and South Kordofan as women in
adult classes are 66 % and 60 % of participants respectively in 2008-2009.
Table 3.3.2.: Percentages of Literate in Population 10 Years and
Over by Sex and Mode of Living, 1993 and 2008
Percentage of
Percentage of
Mode of living
Literate,1993
Literate, 2008
Male
Females
Male
Females
59
37
62
45
Rural
79
60
84
72
Urban
Source: The Fifth National Population Census, 2008
More girls in schools and more women in universities’ and colleges: The increase in
number of girls in primary schools is evident by increase in number of girls’ schools
especially in the private sector. The progress is notable in higher education as there are
universities for women and in some classes the number of young women is more than men.
Families who afford to pay for their girls schooling and higher education allow their
daughters to move to and live in larger cities for secondary school and university.
The progress in education is promoted by increase in number of schools for girls and boys,
changing attitude of parents towards education and the education policies response to CRC,
EFA and MDGs and more specifically the support of UN agencies and donors.
More women in the labor market: The last two decades have witnessed profound increase
in women labor force participation. Table 3.3.3. illustrates that the increase in of
economically active women between 1993 and 2008 is higher for rural than urban areas..
According to 2008 Census women constitute 78 % of professionals and 88.5 % of those
working in service sectors.
91 Table 3.3.3: Labor Force Rate of Population
Age 10 Years and Over by Sex and Mode of Living
Percentages of
Percentages of
Mode of living
Economically
Economically Active,
Active ,1993
2008
Male
Females
Male
Females
45.5
21.4
62.6
36.1
Rural
47.6
10.1
56.9
23.4
Urban
Source: The Fourth National Population Census 1993; The Fifth Population Census 2008
The improvement is not only in number but in areas of work women are engaged in. In
business, women are in large and middle scale investments in construction, import and
export and in manufacturing of different products but the majority in market are pettytraders. Women are also prominent in the medical field, in teaching, engineering, civil
service, and in managerial and administrative work in public and private sector. On the
Other hand Housewives are engaged in home-production of processed foods, painted
fabrics and handicrafts. In rural areas women’s engagement in production have been
intensified with the increased migration of men to urban areas, and according to 2008
Census 28% of women in rural areas are heading families.
The progress in women/girls economic participation is partly related to the increased
educational opportunities and expansion in urban markets. With increasing economic
hardships, conflicts and out migration of men, women have to work and maintain their
families. But an overall major influencing factor is the change in cultural expectations
related to women economic roles.
There are indicators that the economic participation promotes the women empowerment.
For example, women are leading company executives; some women in urban formal and
informal sectors control decision over the incomes and resources they earn including their
free mobility in the public arena. In addition many of the women elites engaged in civil
society organizations(CSOs) are working women with diverse technical expertise. They
have been and currently are also predominant in political parties.38
Women are in decision making bodies: The social and political engagement of women note
a changing situation. Many women are leading or are active members of CSOs, networks
or community- based organizations. They are engaged in addressing women issues as well
as being proactive in providing education/advocacy and health services.
There has been successful mobilization for quota system with 2008 Election Law, a 25%
gender quota was considered for legislative assemblies at all levels as well as for local
committees. The results are thousands of women candidates and increased representation
38
Badri, et al, 2009.
92 of women in the decision-making bodies. In addition most political parties initiated women
segments in which women are actively engaged in promoting the women agenda. The
number of political parties rose to over 100 and all have women members. Some parties
like the Umm\a party, National Unionist Party and the Eastern Front have put women in
leading positions. Some of the interrelated factors contributing to the progress of political
participation of women are: a) the increase in number of educated women who are able to
use their education and their experiences to press for their rights; b) encouragement and
support of enlightened men; c) the technical and financial support of UN Agencies and
international organizations for capacity building of women in political parties; d) the
increasingly changing values and attitudes approving women public engagement.
3.3.3. Persisting Gender inequality
Despite the progress explained above, the gender gaps are still persisting and constraining
empowerment of women and gender equality.
Rights missing in everyday life: The rights gained in legislations, laws and by laws are not
even considered in practice. There is limited or no awareness of most of the rights by many
including women themselves. The rhythm of daily live is governed by cultural norms and
values rather than by rights. . This is evident as the law enforcement practices are not
informed by rights of men and women. In addition, in formal sector the benefits for
children are given to men and not women. Still the women capacities are stereotyped and
thus their opportunities for decision making posts are limited. Up to this point in time
many laws do not conform to international human rights instruments to which Sudan has
ratified and is a part to. Women groups with different political interests are actively
reviewing the Family Affairs Law and Child Law which challenge girls and women rights.
There is need for legislations to address gender- based violence.
More significantly the basic capabilities rights are not supported by laws. No laws stipulate
rights to education, access to information and services. The reproductive rights are not
recognized and those considered in policies such as those related to family planning remain
dormant. The Sudan has signed but not ratified the African Charter on Human and
People’s Rights and the Optional Protocol of the African Charter on Women’s Rights. The
Sudan is still to ratify CEDAW the most important framework for advancement of women.
Advocacy efforts should continue to influence politicians of importance of such
frameworks for women empowerment.
Laws promoting gender equity in formal sectors employment are not enforced adequately
and in fact challenged by prevalent male bias practices. Majority of women are engaged in
activities which are not supported by legal frameworks so they cannot claim rights for
equity and protection.
93 Gender gaps in education: The 2008 Census data shows a gender gap in literacy rate as 51
% of males and 39 % of females of population 6 years and over are literate. The NBHS,
2009, data indicate that there are more literate people (both men and women) in the age
group 20-24 than that of 25-34 years of age. Thus, illiteracy rate among youth population is
rather high for a country with a long history of education. The low level of education is
noted as one third of those in their 20’ who have never attended school, and over one third
of younger group have not completed primary education. The figures for literacy are lower
for urban areas (15 % for males and 26 % for females) compared to rural areas (36 % for
males and 50 % of females).
As Figure 3.3.1 shows the literacy among females demonstrates the Red Sea, Kassala, and
White Nile as disadvantaged states. The statistics of adult education is not very helpful to
show progress in attendance but the gender issue is how relevant are the adult literacy
curricula to capabilities’ needs of women and men. In fact, there is no information to
evaluate benefits and impact of knowledge acquired in these classes.
Figure 3.3.1. Percentages of Literate People in Population 6 and Over by State and
Sex and Mode of Living
Source: The National Fifth Population Census, 2008
According to 2008 Census, the school enrolment rates in basic education for population
age 6-13 years were 49.5 % of females and 52 % of males. The figures for urban areas are
68 % and 69 % respectively, compared to 50.3 % and 45.3 % for males and females in
rural areas. The gender gap is evident among pastoral population as only 14 % of females
and 17 % of school-aged children (6-13 years) are attending school. The World Bank
Report, 2010, indicated a drop of 33 % of students among nomadic groups, where schools
have only four grades. In the absence of boarding schools many children are forced to
discontinue.
94 The findings of FMOE Baseline Survey 2009 reveal that the overall average gross
enrolment ratio is 71.7 % (77.7 % for boys, 65.7 % girls). Disparities between states are
also evident and ranging between 49.9 % in Kassala and 88.7 % in River Nile state. Gender
disparities are above 12 % in all states except the Northern, Khartoum and River Nile
states. .
As concerning school attainment, the 2008 Census data confirmed that only 3% of both
males and females 6 years of age and over had completed primary level, 4.3% reached
level 6, and only 9% completed level 8 of primary education. For secondary education 11
% of males and 12 % of females in the Sudan completed their secondary schooling. While
for the nomadic group, 23 % of males and 16 % of females completed Khalwa education
(Koranic schools).
Table 3.3.4.School enrolment at basic education and secondary level by sex and mode
of living:
Mode
of
%age population 6-13
%age population 14-16 attending
living
attending basic education
secondary school
school
Male
Female
Male
Female
69.0
68.2
81.0
72.9
Urban
50.3
45.3
78.7
29.9
Rural
17.9
14.8
10.5
7.5
Nomads
Source: 2008 Census {Compiled by Omer, etal, table 11.9, p356}
The FMoE 2009 Survey noted that 54 % boys of displaced groups, mainly in Darfurs, were
in schools during 2006-2007 and there is increase in out-of- school children. For this group
the percentages for secondary school attendance for the year 2006-2007 are 54 % and 44 %
for males and females respectively.
Secondary education attendance also shows disparities between rural and urban areas and
between sexes. Only 10 % of males age 14-16 among pastoral population are in secondary
school. The gender gaps are very wide in rural areas, mainly influenced by cultural
preference for early marriage or restriction of adolescents’ interaction.
The overall Higher Education figures confirm the gender gap as females constitute 48.8 %
of Bachelor Degree students and 44 % of Diploma Students in public and private
universities. The Higher Education statistics show that the number of young men admitted
for bachelor degree in private and government universities are more than women, 60,448
compared to 57,535.
Informal Education: Many NGOs and CSOs are organizing educational and training
classes and sessions on human rights, gender equality, environment and violence and some
95 had been engaged in civic education during election. There is no information on specific
aims, content, results and impact of such educational efforts. But the daily public
interaction and practices in markets, universities, hospitals and health centers indicate that
people as well as service providers miss awareness of human rights, specifically
reproductive rights and responsibilities.
The gender gap is narrowing in urban areas as private sector is expanding in education
services but with increased poverty and costs of education poor households may fail to
keep their children in schools and in case of choice preference is given to boys and young
men. But in rural areas, schools are not easily accessible for boys and girls and education
costs are beyond affordability of rural households and in addition early marriage for girls is
perceived culturally as protection for girls as compared to risks and costs forgone by
allowing boys and girls to go to schools. More significantly, gender gap is likely to
increase as there are no effective strategies for poverty reduction and IPRSP is not gender
sensitive.
3.3.4. Gender gaps in economic participation:
In terms of economic empowerment, the country reports show that although women’s
participation in economic activities has increased, gender differentials still exist, with
majority of women working in rural agriculture, informal sectors and low-paying jobs.
Women are more likely to be among the working poor and without any legal protection.
The NBHS, 2009, shows that compared to males, the female labor force participation is
low for all age groups with levels ranging from 29% for those 35-44 years old to 14% for
those 65 years and over . On the whole, in the 15 states the labor force participation for
persons 15 years and above is 48% with 23% for females and 73% for males. The 2008
Census illustrates that 45% of females in the labor force are engaged in unpaid family
work, 25% of females in labor force are own account workers. The refined activity rate
declined for females from 28% in 1983 to 19 % in 2008 Census.
The rural-urban rift is also evident in women economic participation as percentages for
urban areas are 74.8% and 25.2% for males and females respectively. The gap is smaller in
rural areas, showing 63.7% and 36.3% for males and females. 50.6 % of those employed in
the urban areas are in paid employment and 24.8% are own account workers in contrast to
rural areas as 55.7% are unpaid family workers and 28% are own account workers.
Females constitute 10% of mangers and 44.2 of technicians and related professionals.
The NBHS, 2009, results found that the gender gaps in participation rate are very low in
most states in northern and central Sudan. The eastern states, specifically Kassala, show
lowest rates of participation for women. The labor force participation rate for females is
relatively high in western regions of the country with very minimal variations among the
states. The impact of Darfur conflict on these figures is not known.
96 Figure 3.3.2 Labor force participation rate by states, NBHS, 2009
Source: NBHS, 2009
The unemployment rate for females is 23% and is higher than males for all age groups
ranging from 32% for females 15-24 years old to 14% for females 45-54 years old. The
youngest age group 15-24 years including male and females has the highest total
unemployment with 20 % (NBHS, 2009).
In formal sector, they are relegated to low-paid jobs and their percentages are very small in
decision-making positions. In the market, they are very vulnerable with no legal status and
trying to survive in unfriendly work conditions.
The gender gap and disparities among regions related to economic participation are
manifestation of interrelated factors including: 1) lack of policies for employment or
economic empowerment that are responsive to gender and people needs; 2) the inadequate
educational policies that have failed not only in addressing people needs but in providing
needed skills for economic engagement; 3) shortcomings in legal frameworks related to
economic participation.
3.3.5. Women voices in public are not loud enough: The increased participation of
women in civil society work has not generated a strong CSOs movement for advocating
and monitoring government performance related to poverty reduction, human rights,
women empowerment and gender equality. The CSOs participation is dominated by
educated men and women. There is no information on the social and economic groups/
associations among illiterate or rural or poor women in urban neighborhoods.
The gender issues for political participation and representation are tremendous. The
quality of women participation remained limited as many women have not been exposed to
political socialization. Thus political dialogue and analysis remained dominated by men.
Still, the very few women are in lead positions in political parties.
97 Experiences in elections have shown that representation of women remained generally low
as the percentages in the different parliaments since 1968 have been far less than 10% and
fluctuating at the state level. Even in the appointed parliament that was formed after the
CPA the highest percentage reached was 19%. The quota has brought more women to the
parliament but they are from one political party as most political parties have boycotted
election.
There is a problem with quality of representation as still the women parliamentarians have
not been able to voice priorities for women in parliament. Thus their presence is not yet
sensed by grass root women. The grass-root women specifically those in rural areas
remained isolated from women activism, with no/ limited knowledge on political rights and
their responsibilities for democratic transformation.
The paucity of gender disaggregated data and information on political participation is a
challenge for monitoring progress. There is lack of data on women participation in local
councils and popular committees. In fact there is need to understand the socio-cultural and
economic factors influencing quality participation of women at all levels. In addition there
is no information on young women political participation.
3.3.6. Gender- Based Violence:
Gender Based violence (GBV) is the most extreme manifestation of gender inequality. The
GBV in the Sudan is under-investigated and under- addressed issue and mostly taken from
health perspective and dealt with as if existing only in conflict areas. It is only recently that
there is recognition to the existence of GBV.
The results of 2009 Survey on Violence against Women (VAW), shows that 92.6 % males
and females 89.2%, confirmed prevalence of violence in Sudanese communities and 69%
of males and 77% of females noted that it is an old practice embedded in society. The
respondents identified the types of violence as deprivation of women of their rights and
physical assaults and use of force against women as indicated in Table 3.3.5.
Higher percentages of university students identify VAW as deprivation of rights and bad
treatment while less than 10 % of males and females mentioned rape. The reasons given for
the violent practices are ignorance (45.9 %), traditions and customs, 19.6% and less than
quarter of males and females mentioned low religious awareness, and economic pressures.
More than half of male and female respondents thought that the existing laws and
legislations are not enough for protection of women and children from violence. The
survey results are important although the FGM and early marriage have not been included
in definitions used.
Table 3.3.5.: Percentages of Respondents Definition of Violence Against Women
Concept, by Sex and Education
98 Character
istics
Males
Females
Violence Against Women
Rights
Bad
Cruelty
violati
treatmen
t
on
9.30
26.30
26.30
Beati
ng
Use of
violence
22.4
0
23.2
0
6.30
6.00
10.40
22.00
39.60
Abu
se
Rap
e
15.6
0
12.4
0
8.30
8.00
Secondary
school
education
University
graduates
16.2
0
2.90
11.80
19.10
19.10
13.2
0
2.90
24.8
0
6.00
9.70
24.80
37.80
11.8
0
9.10
Postgradu
ate
35.1
0
10.80
13.50
13.50
18.90
24.3
0
10.8
Source Abu Alyman, 2009, p 8
It is evident that respondents are focusing more on domestic violence. The recognition to
VAW is important as for a long time there has been denial for existence of violence in
Sudanese families. This is because acts of violence such as beating of daughter, sister and
son or depriving them from their rights practiced by elders mostly males, are culturally
approved as acts for disciplining and protecting family members and their honor. This is
how FGM is culturally justified. Therefore the responses of survey respondents indicate a
changing perception and attitude to VAW, and that need to be promoted and further
investigated among illiterate men and women.
3.3.6.1. Early Marriage:
According to the 2008 Census about 2.3% of age group 10-14 years is married and 24.6 %
of those 15-19 are married. The SHHS 2006 results, showed that 12.4 % of women aged
15-48 were married before the age of 15 and 36.6 % were married before the age of 18.
The results noted the link between prevalence of early marriage and low education
attainment of mothers and the economic situation of their households. While 17.9% of
early married cases have mothers with no education, 3.8% have mothers with secondary
education. 16.1 % of those married early are from poorest households, 5.8% are from rich
households. It is very difficult to generalize on these linkages as socio-economic contexts
are changing. Recently poverty is forcing households to depend on economic contributions
of its male and female adolescents and early marriage means loss of income for such
households.
Early marriage though it is violation of girls’ right, it is stipulated by law. It is preferred in
rural areas for girls as value for women is related to her fertility. The earlier she is married
99 the more children she can have. This perception ignores the reproductive health
complications of early marriage. Therefore the cultural base should be the concern in
identifying the practice as GBV.
3.3.6.2. Female Genital Mutilation: Challenging Success
Female Genital Mutilation (FGM/C) is the operation of cutting and removal of the tissues
of genitalia of young girls of age 8-14 years. The 1990 Sudan Demographic and Health
Survey, the 1999 Sudan Safe Motherhood Survey, and the 2006 Sudan National health
Household Survey (89%) showed that the practice is still widespread with very minor
change in prevalence, being in the range of 89-90 % among women age 15-49 in the
Northern part of the country. However, the prevalence is lower in West Darfur (54%) and
Blue Nile (73%). The rates are somewhat similar in rural and urban areas and among
women with different educational background. The practice is non-existent among some
groups in Kordofan and Darfur. Most of the existing prevalence rates are based on selfreports of respondents to surveys and their ability to reflect the real situation on the ground
is questionable.
FGM is a social practice, culturally believed by women and men to protect girls’ virginity,
maintain cleanness/ purity, chastity, reduce girls’ sexual desires, and thus preserve family
honor, ensure mariageability, morality, fidelity, and enjoyment of men for sex. Supporters
have tried to relate it to religion. Decision makers for the operation are the women
specifically grandmothers, men are supporters, but sometimes demand come from the girls
themselves when pressured by school peers for it. FGM is also a source of income,
privilege and power for the operators who are mostly the midwives, (very rarely that
doctors are involved in the operation).
Efforts against FGM/C started in the 1946, when the colonial administration added an
article in the Sudan Penal Code banning the practice. This however, found opposition from
the political leaders and the article remained dormant until removed in 1991.
It is evident that the practice has its social, cultural, economic, and political and health
perspectives.
Progress in fighting FGM: It is only in the late 1970’s that few NNGOs identified the
practice as harmful and started working in advocacy and raising awareness for its
eradication with support of the international partners. The number of NNGOs interested in
banning the practice started to increase and in 2004, 42 organizations established a network
aiming to end the practice.
Anti- FGM approaches evolving: Several approaches have been used in addressing FGM.
These include health risk framework, de-linking FGM/C from religion, human rights
approach, village/community empowerment programmes and ‘Saleema’ approach.
100 Recently, an integrated rights-based and culturally sensitive approach to promote behavior
change has been introduced and its impact still to be seen.
Some results/successes: Although the practice is still prevalent but some important
results/success from different interventions are evident. These include: a) Advocacy: There
are loud voices against a taboo issue. Some young uncircumcised women and some men,
academicians, activists and youth are involved in the advocacy. There are as well debates
on the human rights perspective of the practice and it has been labeled as violence against
women. b) Knowledge on FGM/C types, prevalence, and attitudes related to FGM/C; some
health hazards related to FGM/C identified; publications by notable religious (regional and
national) men delinking FGM/C from religion specifically Islam. c) Policies, Strategies
and Laws: National Strategy for Eradication of FGM, 2008-2018; Law banning the practice
in five states; Sudan signing regional declarations for banning the practice39; the Sudan
Medical Council recommendation for banning the doctors from undertaking the operation
and the attempt of the Council to raise/deal with the involvement of one of the doctors in
the operation; the NCCW and its state level committees are engaged in coordinating the
eradication activities; Number of NNGOs and an Anti-FGM/C Network with accumulated
experience in eradication programmes; d) Positive Community Responses: Notable political
leaders such Umma Party and the NCP support anti-FGM/C movement; some communities
in villages/ neighborhoods in urban areas have declared publically their stoppage of the
practice. d) Partnership: There are experiences of collaboration among local CSOs and
between CSOs and government institutions in formulation of law and anti-FGM strategy.
The experiences of partnership/collaborative activities between the international
organizations and UN Agencies on the one hand and the government institutions,
specifically NCCW, and NNGOs, have generated learning processes and contributed to the
improvement of anti-FGM approaches.
Why GBV is persistent? Generally, GBV is primarily supported by cultural factors which
are not easy to deal with and needs change of mindset. In addition, the recognition for
prevalence of GBV/VAW is very recent and need to be visualized from a gender and
human rights perspectives. In relation to FGM, some of anti-FGM/C approaches are not
addressing adequately the root- causes of the practice. Still the health messages has not
considered the contributions to the male and female sexual problems related to FGM/C and
the link between infertility and FGM/C and all these negate the marriage-related motives
for FGM/C. Still the medical community voices are not strong on the gynecological
complications that result from the female FGM/C and can become particularly serious
during and after childbirth, and include fistula.
39
Such as: ‘The Rabat Declaration on the Children Issues, 2005, for member countries of the Islamic
Congress; ‘The Khartoum Declaration of the Islamic Congress for Ministers Responsible for
Childhood 2009’ for the member counties of the Islamic Congress.
101 Challenges:
VAW Strategy focuses on legal perspective and while most types of violence are
culturally- based and linked to gender power relations.
The Government commitment for eradication is still has not adequately institutionalized,
not sustained and remained personalized and unclear. The government is committed to
CRC, regional declarations and national strategies for eradication and at the same time
denied the approval of the article in Child Law, 2008, banning FGM/C. Still anti-FGM/C
activities are funded by the international communities and thus dependency and no local
ownership.
There is contradiction in criminal law in taking rape as adultery/zina and that means
women are losers by being raped and by law would be punished as participants in crime.
Emergence of religious supporters/ advocates for the mild type of the practice and their
attempt for its medicalization is a challenge.
The anti-FGM programmes are not adequately coordinated and different communities in
the same area are exposed to different approaches from the different active organizations.
Many Sudanese women have been widening their spaces, and challenging the cultural
boundaries taking new roles, changing attitudes, economic and political roles and
remaining silent on FGM. In addition, many women have been able to influence decisions
of the family for girls’ education but have not been able to take decisions to protect their
daughters from the practice.
Opportunities
Failure to pass law against FGM has not discouraged anti-FGM advocates from
government as still their voices are high
There are experiences in neighboring countries for addressing GBV.
3.3.7. Women leadership in conflict context: building the momentum for development
The civil war, conflicts and environmental hazards have led to the emergence of
communities of internally displacement people(IDPs) in urban and in some rural areas. The
main IDPs camps are in Khartoum and Darfur. The lesson learned from IDPs in Khartoum
is that: IDPs men and women are agency as many of them have been able to overcome the
constraints of poverty and bridge the cultural and social differences to ensure economic and
social security for their families.40
The Darfur conflict since 2003 has been characterized by widespread human rights
violation including murder, abduction and rape. Many of Darfur women and men have
been forced to leave their villages and are living as IDPs in camps or hosted by some
communities in villages and urban areas. They are experiencing vulnerability as conflicts
are recurrent. The majority in camps are women who have to adapt to new context and
adjust their roles and relationship as they lost all sources of their livelihood and traditional
40
See Al Nager, 2011.
102 support systems and mechanisms. In addition they have to experience and manage ethnic/
cultural diversity in everyday interaction. Those in camps near the towns, such as in Kalma
Camp, have been engaged in construction work, tea selling and housework and thus they
are competing with town women for the limited jobs available. The educated women in
camps, organized classes for children, encouraged and supported by the local/national and
international organizations active in displaced Darfur. In many villages hosting displaced
people, the displaced women survival strategies have put them in competition for resources
with host communities. The majority of women displaced in Khartoum and other areas,
continued to support their men in the struggle to overcome poverty and maintain livelihood
of their families despite the lack of the majority of them to the relevant skills.
The response rate to the help received from Development Agencies is high among IDPs
women. In the camps women are exposed to knowledge on: gender equality,
human/women rights, reproductive rights, family planning and prevention from violence.
Many were trained to promote or learn new production skills, use new technology, sell
products in camp or urban markets and earn and control incomes. Women have also been
encouraged to work in groups, to participate in decision-making and to adapt new values
for social participation and management of diversity. They learned to engage with
diversified groups to undertake responsibilities which are different from those traditional
roles of food preparation they do in ‘nafeer’41 gatherings. They learned to manage water
points and centers for women activities and some organized classes for children. Some
women have been trained in mediation and conflict transformation, and have been
encouraged to work in conflict prevention and management if needed in IDPs camps.
The local organizations and Development Partners provided basic services in the camps.
Specifically to be noted are the services for survivors of violence, for delivery by trained
birth attendants, and for accessing EmONC. Knowledge on HIV/AIDs is also provided and
some women are encouraged to assist in raising awareness of their communities on the
issue.
Recognized leaders: The native administration (NA) has been recognized as governance
structure for managing resources and activities within the camps. Despite that NA is
dominated by men, Women Shaikas and Hakamas42 have been recognized as leaders and
have taken responsibilities for identifying women needs and participating in meetings
between NA and service- providers.
41 Nafeer is a word used in Arabic (Sudan, etc.) to describe a collection of individuals in a village or
neighborhood who join voluntarily to undertake collectively specific activities. 42 Hakama is used locally in Darfur to refer to the woman leader who compose songs praising or
mocking men and women
103 Gender inequality is still persisting. Despite the effective participation of IDPs women,
their roles remained ‘invisible’ and practices of women marginalization are prevalent.
Gender equality in hiring for casual labour especially for building work was never
accomplished. While consideration is given to hire equal numbers of women and men as
local staff, women generally had the lowest level staff positions. The justifications given
for these inequalities are: women lack of language skills, and/or generally lower
educational levels; women are shy and do not prove competence in interviews. It is evident
that the Development Partners’ approaches contribute to prevalence of gender inequality.
The interventions are not built on gender analysis to understand and deal with cultural
constraints to women participation.
Again, the prevalence of cultural factors sustaining dominance of men in gender power
relations limits role of women leaders. In the meeting of NA with service providers, the
Sheikas ‘would not talk because they were not allowed and it was generally because they
were not asked. This raises the ongoing issue of women needing ‘permission’ rather than
exercising the freedom and right to speak as desired’43
Challenges:
One challenge is how to ensure that the implementation of new Peace Agreement is built
on the achievements and new experiences learned in camps.
The women leaders in camps have been exposed to contexts of decision-making without
being empowered with needed skills to address the challenges of ‘gendered’ views and
spaces promoted by male native administration leaders.
The great challenge is how to shift from humanitarian to development perspective and help
women to consolidate the new skills they learned in the camps so that they sustain it in resettlement contexts.
Many rural women living in camps have been exposed to knowledge on and accessed RH
services. The challenge is how to integrate into reconstruction plans the priority of RH
services to enable women in resettlement context to exercise similar rights.
Opportunities:
The implementation of New Peace Agreement which includes reference to some
women rights is under consideration.
Concerns, interest and expected support from international communities to the peacebuilding in Darfur are still keeping momentum.
In current IDPs contexts there are initiatives for dealing with the structural challenges
to gender equality, including gender awareness-raising activities for all staff and
English lessons for lower level national staff (mainly women). Some activities
43
See De La Puenete p375
104 included women in training for non-traditional activities such as masonry and latrine
construction and men were motivated to participate in cleaning campaigns44.
3.3.8.. Efforts to address the gender gaps /issues
The last two decades witnessed increased concern and interest in gender equality and
women empowerment and commitment to MDGs helped in building a momentum for
addressing some of the gender gaps. The gender mainstreaming (GM) was adopted by
government and some CSOs as a strategy for promoting gender equality and women
empowerment. The national women machineries at the federal and state levels have taken
responsibilities for GM with support of UN agencies. The efforts for GM have included
building capacities of staff and institutions responsible for gender mainstreaming,
supporting advocacy for GM among decision makers to create political will and secure
needed support from government institutions. As the public spending on education, health
and capacity building for development is very limited, gender budgeting has been
discussed by concerned women machineries to try to avail resources for some priority
issues related to women empowerment. The outcomes of such processes are plans,
strategies and legal frameworks and institutions enhancing capabilities, responsiveness and
accountability to gender equality and women empowerment.
Policies and legislative measures: There are a number of policies and decrees and laws that
have been formulated to promote women empowerment. These include the National Policy
for Women Empowerment has been issued by the Council of Ministers in its (9) Ninth
Session of 4 March 2007 which encompasses six main thematic areas for the empowerment
of women; b) the detailed action plan formulated for implementation of policy and this
was included in the Five Year Strategy for the years 2007-2011; c) The formulation of a
Five-Year Strategy for Child Welfare 2007-2011 in partnership with ministries of concern
with children as a comprehensive and integrated strategy; d) The Strategy for Combating
HIV/AIDS among women with full support from National programme combating
HIV/AIDS and UNAIDS and civil society.
The specific legal measures related to empowerment of women is the Central Bank of
Sudan decree No. 18/2007 for the organization and development of the banking system to
contribute to poverty-alleviation. The specialized financing ceiling for social development
was increased from 10% to 12%. Moreover, the decree No. 18/2007 stated that 30% out the
fund ceiling is for women and 70% out of the 30% is for rural women.
Institutional Arrangements: There are a wide range of institutional arrangements put in
place to promote advancement of women. The main national women’s machinery in
Sudan is the General Directorate of Women and Family Affairs (GDoWFA) which is
44
See De La Puenete, 2011
105 housed in the Ministry of Social Welfare and Social Security (MoWSS)45. The Directorate
is charged with mainstreaming gender concerns into policies and plans for empowerment
of women.
A number of Women and Gender Units have been created in the Sectoral Ministries
including Health, Justice, Foreign Affairs, Labor, Education, Agriculture, Finance, Industry
and the Central Statistical Bureau. The sectoral-level initiatives include in addition, the
Unit to Combat Violence against Women, in the Ministry of Cabinet and the Family and
Child Desks in the Police Stations. These Units are focal points and coordinating
mechanisms for mainstreaming gender in the sectoral plans and strategies.
At the state level the women and gender units and the coordinating committees at the
Ministries of Social Affairs are considered the mechanisms charged with the
implementation of the National Policy at the States' level. These are responsible for
monitoring progress of women empowerment processes.
The Micro-finance Unit in the Central Bank of Sudan was established in 2007 and has
mandated 30% of the micro-finance for poor women. There are nine Women Development
Departments within the financial and banking institutions.
Challenges:
The gender law reviews have not been put in action. This means that the legislative
framework in the country still needs to address some of the most pressing issues, including
sexual violence towards and abuse of children, early marriage, rape, and the legal position
of women in the informal sector. In addition there is need to challenge the current focus on
marginal issues such as women’s dress and public appearance. Legislation in place that
does promote women’s empowerment is often not enforced, or is overridden by other laws,
such as Public Order Law.
There is shortage of sex-disaggregated and age-disaggregated data and analytical studies
which give insight into the root causes of discrimination and the differences in
opportunities and benefits for different groups specifically for rural women and men.
The limitation in quality of education, economic and political participation constrained
women empowerment thus many women are still not aware of their rights specifically RR,
not taking decisions concerning their bodies, and accessibility to RH services and are
maintaining harmful practices.
The VAW Unit prepared a plan that considers the enactment of a law for ending violence
against women and promoting protection. The challenge now is how the Unit will
operationalize the plan for effective results, and coordinate the on-going collaborative
initiatives with CSOs and relevant government institutions
45
This Directorate was founded in 1993.
106 The private sector is demonstrating interest in social development but there is no clear
strategy to use private sector effectively.
The CSOs divisions and limited capacities hinder its affective role in scrutinizing gender
sensitivity of policies, plans and budgets of public and government institutions and hold
them to account.
Opportunities:
Despite the challenges mentioned above, there are opportunities for promoting gender
mainstreaming.
A rural women programme integrating rural women concerns and needs is now under
formulation. The programmeme would be funded from local resources of banks, Zaka
in collaboration with UN Women. The implementation of the programme is an
opportunity for testing capacities of women machineries’ staff at federal and state
level, GB experience and functionality/effectiveness of monitoring system. The
programmeme is multi-sectoral and thus if realized would reach rural women with
culturally sensitive RH services.
UN Women is expanding as independent partner and is investing on gender
mainstreaming and GB.
3.3.9. Concluding remarks:
The gender analysis confirmed that there is important progress in aspects of women
empowerment and in addressing gender gaps. Gender gap in education is decreasing, more
women are economically active. The women political participation and representation in
decision-making bodies witnessed a boost. It is important to mention that international
consensus on women rights and frameworks for their advancement and support provided
by Development Partners have helped in promoting commitment of successive
governments and CSOs in Sudan for women development. But despite that the gender gap
persists. This is because absence of democracy, conflicts and inadequate development
policies generated resistance and drawbacks to commitments and initiatives for women
empowerment and gender equality.
The women movement kept obstructed momentum as the women issues have been
politicized in a context of political instability and conflicts.
There is no consensus on harmful traditional practices which violate women rights. That is
why the progress and improvements happening are halfhearted.
Still many laws are not gender-sensitive and policies are not gender-responsive.
The main challenge for gender analysis, mainstreaming and programmeming is lack of
gender-sensitive data and knowledge on everyday lives and challenges of rural
107 communities. Actually it is very difficult to present the gender issue at the state and locality
levels as no statistics and no studies are accessible.
The persistence of gender gaps is also related to the limitations in programmeming
approaches and conceptualization. Despite that activities aiming for ‘capacity building’ for
GM are done still needed expertise for gender- sensitive programmeming is lacking in
government. This is because what is done is training without mentoring and monitoring for
impacts on practices. The training by time turns to be theoretical exercise.
In conclusion it is evident that many women specifically in rural areas are not empowered
because they do not have needed capabilities to access resources, opportunities and
control decisions related to their basic rights and needs. Thus, many women still lack
agency to protect their maternal health. Accordingly, the prospects for achieving gender
equality are limited.
3.3.10. Recommendations:
The current analysis shows that gender gaps are persistent in rural areas and among
nomads and poor groups. Accordingly the focus should shift to these areas and vulnerable
groups. That needs effective advocacy and campaign for considering targets of MDG 3 and
5 with focus on rural women but considering involvement of men. This focus entails
gender-sensitive surveys and comprehensive gender responsive and pro-poor integrated
programmes. Such programmes then require engagement with locality authorities, CBOs,
popular committees, rural men and women. Log for lessons learned and good practices
should be institutionalized in programmes.
It is important to recommend that progress noted should be assessed to draw lessons and
promote agency of women and men to sustain cultural changes that supports equal gender
rights and spaces. One way of doing that is by forming a representative consultative ‘watch
dog’ committee from CSOs with main responsibility of monitoring accountability to
MDGs 3 and 5 and 6.
The priority efforts for GBV are the law review for ensuring protection of rights of girls
and women.
There is need for more surveys to identify GBV understanding among grass-root women
and revise the VAW Strategy accordingly. GBV issues should be integrated in training and
awareness raising activities.
With new Peace Agreements women in IDPs should be oriented with impact of Agreement
and their role in protecting their rights in implementation processes. That may entail
coordination among active Development Partners in the camps and urban areas to help
women consult and have a strategy for resettlement.
108 Gender–sensitive partnership with research centers and universities should be considered in
all development programmes. Participation and consultation with gender expert in all
research stages should be basic principles and conditional approach for good quality
gender-sensitive surveys and research.
Policy dialogue and consultation processes at federal, state and locality levels, are
important to create commitment for GM and specific gender issues and build consensus on
women rights and on critical gender issues. In addition the consultation should aim to
manage diversity of actors and bridge their differences for women empowerment and
gender equality.
The national and international development partners need to come together to review the
short comings in understanding of concepts ‘capacity building’, ‘capacity development’
and agree not only on what concepts mean but what is relevant to Sudanese conflict and
post conflict contexts and what is most relevant for development and peace-building. There
are voices against training workshops and calling for long-term and in-service capacity
building. That is a call for new approaches.
Many development practitioners are aware of importance of coordination but it remained
missing and contributing to weak results. Coordination can be realized only if we consider
it as a value and principle and a cultural element to be central to development work. It has
also to be started by practice at the start of planning programmes. While planning any
development programme it is essential to investigate what others are doing and build on
coordinated activities. That would serve many purposes, bridging existing gaps between
government and CSOs and among sectoral ministries and among CSOs.
109 SECTION 3.4.: YOUTH AND ADOLESCENTS: THE FORGOTTEN
CATEGORIES
Youth remained an important category among the Sudanese population and their role in
social and political life have been well recognized as indicated by the recognition of
student unions/associations, youth centers’ and the presence of a Ministry of Youth for
decades. However, despite the apparent recognition, their specific needs and rights are not
yet considered a priority.
There is no consensus on age group representing youth. The Ministry of Youth, Culture
and Sports identify youth as those between 15 and 35 years of age. Recently there has been
concern to consider the adolescents age 10-19 as a group with different needs from
children and other young people. This is followed in current analysis.
As noted in Population Dynamics Section the adolescents and youth constitute a substantial
percentage of population, with slight gender differences. The profile of this group as
represented by NBHS, 2009, shows more young women in rural areas than urban areas and
as rural areas are disadvantaged in development programmes and services, then those most
vulnerable are rural young women.
3.4.1. Marital Status:
The marital status of adolescents is becoming a critical issue as 5.5% of girls and boys in
age groups 12-14 and about one fifth of those aged 15-19 years are married with a higher
percentage of married adolescents in pastoral communities. To add to the above-mentioned
adverse effects, early marriage constrains girls chances to promote their capabilities and
thus they would be the mothers who maintain the gender inequality culture and related
practices.
Table 3.4.1 Percentage of married among males and females population by age and
mode of living
Age
Total
Urban
Rural
Nomad
grou
p
Mal
Femal
Mal
Femal
Mal
Femal
Mal
Femal
e
e
e
e
e
e
e
e
1.7
3.8
1.5
2.9
1.9
3.9
1.2
5.8
12-14
3.6
22.3
2.2
16.0
4.0
24.1
5.7
34.0
15-19
16.2
53.9
9.3
41.7
18.9
58.9
28.8
68.2
20-24
42.0
74.0
29.2
65.3
48.3
77.1
58.7
84.4
25-29
63.4
80.1
52.4
74.0
68.8
82.1
73.3
87.5
34-34
Source: CBS, 2008 Fifth National Population Census
110 According to 2008 Census about three quarter of females in age group 25-29 are married,
with higher percentages in rural areas and among pastoral communities. Percentages of
married women tend to be lower with younger ages. This is because more women are in
universities. Generally the economic situation is constraining many youth from marriage
and formation of families. Delayed marriage age for youth means prevalence of sex
relationships outside marriage institution. With the discouragement to use of family
planning methods, this is likely to increase the number of abandoned children and exposes
youth to RH risks.
3.4.2. Education:
The section on gender inequality confirms the existence of gender gaps and regional
disparities in school education. It is also shown that rural youth specifically females are
disadvantaged compared to those urban areas. The issues for adolescents and youth
education are the poor quality of education which does not empower them with knowledge
and skills needed for protecting their reproductive health. Education is not responsive to
labor market and does help in career development for youth.
3.4.3. Economic participation:
As Sudan is committed to the CRC, ICPD, MDGs and other global frameworks,
adolescents age 10-19 should still be in educational institutions but the reality denotes a
different situation. The 2008 Population Census data shows that adolescent males are
economically active in urban areas more than females and that economic participation rates
for age groups 10-14 and 15-19 years are higher in rural than urban areas. In addition,
63.5% of males and 37% of females in age group 10-14 and 74% of males and 26% of
females in age group 15-19 are heads of households. Thus, adolescents assume heavy
responsibilities which may expose them to risks at an age when they need to cope with
changes in their bodies, feelings and cultural restrictions imposed on them.
The figures for labor force participation show wide gender gap for all age groups between
20-34 years specifically in rural areas. However the gender gap tends to decrease with
younger ages in urban areas. This is expected with proliferation of young women in urban
labor market and increased number of employed women in public and private sector. The
gender gaps are higher for urban areas than rural areas for group 20-24 years as indicated
by Table 3.4.2. We need to go beyond these figures to understand reality of youth
situation. The majority of youth are working in the urban informal sector in petty trade and
domestic services. In rural areas they are in agriculture and animal husbandry but mostly
unpaid family laborers. All these activities are not protected by the law and local cultures
restricts youth from claiming any rights in rural areas. Therefore, the issue of youth is not
only income poverty but human poverty as well, which means that youth economic
engagement does not necessarily lead to economic empowerment.
111 Table 3.4.2. Age specific activity rates by mode of living, 2008
Age group
Urban
Rural
Nomad
Male
Female
Male
Female
Male
Female
5.0
2.7
15.7
11.8
47.3
23.4
10-14
21.3
6.4
32.5
17.1
58.6
26.0
15-19
44.1
14.7
55.7
21.5
70.2
24.5
20-24
68.0
23.3
74.3
25.8
79.6
23.2
25-29
77.2
26.2
80.8
27.0
83.9
24.1
30-34
Source: 2008 Census; {Compiled by Mahmouud, table, 14, p15}
Unemployment remains the major problem as there are no strategies for career
development for youth. In addition, there is limited access to reliable information on
employment opportunities. Almahdi, 2011, on the youth employment in Blue Nile, North
and South Kordofan conformed that for all types of jobs whether in private or public
sector, youth depend on informal contact with relatives and/or friends. But still some h
resort to the labor office in their pursuit of employment (43% of those interviewed in Blue
Nile State). 46
3.4.4. Poverty:
The poverty status of rural youth tends to be high as compared to urban youth. NBHS
(2009) shows that one quarter of youth in urban areas and half of those in rural are poor. A
study on youth in Kassala and Gedaref states pointed to the high unemployment rates and
temporary jobs (Table 3.3.3.). Youth monthly incomes are very below SGD 400. Over
three quarters of youth surveyed in both states considered the income they earn as
inadequate. About 40% of the surveyed youth in the two states are suffering financial
constraints, which impacted negatively on their education and on their families’ survival.
Table 3.4.3. Poverty Aspects of Youth in Kassala
and Gadaref States
Poverty Aspects
Kassala
Gadaref
Employment Status
Employed
38.8
Unemployed
61.2
Permanent Job
43.3
Temporary Job
56.7
Sources: Elias, 2008 (a) and Elias, 2008(b).
35.2
64.8
36.9
63.1
The public efforts for poverty-reduction among youth included Productive Student
Programme, and Grant projects, mainly implemented within universities. The Graduate
46
Almahdi, 2011.
112 Employment Project is implemented by the Ministry of Human Resource Development.
The latter has had a 4-year strategy (2005-2008) and has reached some 297,050
graduates47, but the project is facing problems and most of small graduate projects have
been sterilized.48 Other programmes for youth capacity building have been established
such as National Center for Youth Training but these are weak in capacities and also suffer
funding problems.49
3.4.5. Adolescents and Youth Reproductive Health Profile:
Adolescent health, as addressed under the 2010 RH policy, covers the transition period
between childhood and adulthood and seeks to guide young adults manage physical and
physiological changes during this transition. Special attention is paid to the prevention of
sexually transmitted diseases including HIV/AIDS and unsafe or unwanted pregnancies
and the management of fistula related to early pregnancy.
The relatively high percentage of married females under 20 years would contribute to high
level of fertility in Sudan as their actual reproductive lives are extended to longer periods.
They also become exposed to the risks of early pregnancy and related morbidities,
including obstetric fistulas as 95% of married adolescents are not using contraceptive and
over 46% of them deliver with assistance of TBA, friends or relative (SHHS, 2006). Data
shows that 36 % of abortions in 2008 were from group 10-24 years, i.e. including
adolescents.50
The FMOH /RH Adolescents' Survey, 2010, undertaken in five states points to some
important issues that need to be taken in consideration, (data is not sex-disaggregated). As
Table 3.4.4 shows the adolescents are involved in sex relations and suffer STIs, but they do
not have the adequate knowledge and services to protect themselves. They are also
engaged in harmful practices such as drug abuse and some are victims of violence.
According to FMoH, 2010, the violence is from teachers, from peers and the violence
includes sexual harassment. The study also shows that adolescents’ peers are main source
of knowledge.
Table 3.4.4. Adolescents’ Reproductive Health, Knowledge and Practices
Variable
%
Knowledge about methods of prevention
Knowledge that HIV/ AIDS is
transmitted by sexual intercourse
Involvement in sexual relations
47
See Youth National Strategy, 2007-2031
ibid
49 ibid
50 FMOH, 2010,
48
113 84.0
25.6
11.0
Reported STIs
Drug use
Violence: rape
Violence: Physical abuse sometimes
Sources: FMoH, 2010
3.0
2.3
4.4
52.0
With paucity of data the profile is based on SHHS, 2006, focusing mostly on women. The
data demonstrates that above one third of age groups 20-24 and 25-29 are married before
age of 18 years. The problem is that substantial percentage of those who marry young do
not take good care of their health during pregnancy as more than half of those less than 30
years have not taken all doses for tetanus prevention, one quarter have no ANC services
and many are assisted in birth by TBA or relatives and friends. Again the data shows risks
of frequent pregnancies as small percentages use family planning. The efforts for raising
awareness of the young women on HIV/AIDS are evident as substantial % of them know
how the disease is transmitted but still knowledge available is limited as very few know all
methods of transmission.
According to the National Survey for Children and Youth, 2007, 22% of those surveyed
from age group 12-24 years have not heard about STIs and 74% who heard about it, have
not been able to identify any STIs symptom or ways of getting infected with diseases.
While Sudan National AIDS Control Programme data, 2009, indicated that 0.67% of youth
are HIV/AIDS positive, 0.5% of them males and 1.24% females, with prevalence of .33%
in rural areas and 1.14% among IDPs.
Table 3.4.5.A -Youth Reproductive Health Profile from SHHS, 2006
(Knowledge Attitude and Behavior)
Variable/Age
152019 y
24y
% of married women before age 15 years
6.9
11.5
% of married women before age 18 years
34.0
% of mothers who received at least 2 doses for
43.2
46.9
protection against tetanus
% of women who heard about STDs
73.3
72.8
% of women who know all ways of prevention from
2.4
4.1
AIDS
% of women who had any FGM form
% of women who intend to circumcise their daughters
% of women who do not intend to circumcise their
daughters.
% who think practice should continue
2529y
14.6
37.0
47.6
3034y
14.7
36.9
52.2
68.9
5.1
68.8
4.9
76.4
58.8
35.4
86.6
55.5
41.8
89.1
54.8
42.3
89.0
54.2
42.6
58.3
55.1
52.3
540.5
% who think practice should NOT continue
39.2
44.6
45.4
46.3
Source: Adapted from SHHS, 2006, tables, 9.2 (p134); 11.2(p172)13.3(192;13.5(192)
114 Table 3.4.5. B -Youth Reproductive Health Profile from SHHS, 2006
(Services Provided)
Women/%
15202519y
24y
29y
Personnel providing ANC
Medical doctor
34.7
36.0
36.1
Nurse midwife
14.5
12.1
12.8
No ANC
22.4
23.6
24.8
Personnel assisting in
Auxiliary
27.6
24.4
24.7
delivery
midwife
TBA
26.7
19.7
22.1
Relative/ friend
15.6
16.6
16.1
Contraceptive use
Pill
61.4
49.7
53.3
LAN
21.0
20.6
26.8
3034y
39.3
13.0
23.6
27.0
17.5
16.1
54.6
18.8
Traditional
35.0
35.4
30.0
32.5
methods
Source: Adapted from SHHS, 2006, tables, 10.1(p 144; 10.7(154); 10.4(p149);10.5 (151))
The studies of youth in Kassala and Gadaref show the following: 38.75% and 68.8% from
Gadaref and Kassala respectively know of one methods of prevention from HIV/AIDS;
94.5% and 46.1% know that disease is transmissible; and 38.7 % and 65.4% know one
means of transmission. The impact of efforts for raising awareness on the disease is evident
but still the knowledge acquired is not adequate and needs to be consolidated.
3.4.5.1. Harmful practices:
The risk and violation to women health is evident in very high prevalence of FGM, noted
above in GBV section. The challenge in fact is that according to the SHHS, 2006, more
than half of young mothers surveyed intend to circumcise their daughters. According to
Elias 2008 (a) (b), 79.6% and only 33.4% of youth surveyed in Gadaref and Kassala
respectively oppose the practice. Therefore it is evident that there are future parents
approving the practice which means the future generations of girls are at risk.
Drug addiction is noted to be widespread among youth. According to the Directorate of
Combating Drugs, 96% of those arrested for drug dealing are less than 18 years and above
50 years51. Elias, 2008, noted that 99% of youth in Kassala, smoke cigarettes and use
tobacco and the figure for Gadref is similar. It should be noted that the group surveyed
include young women and in conservative communities of the east the spread of these
practices means that young girls are breaking cultural barriers but going the wrong
direction.
51
See National Youth Strategy, 2007-2031, p13
115 3.4.5.2. Social and political participation:
Adolescents are seldom recognized as a social category and thus no specific arrangements
are made by the government or by community for their social activities and entertainment.
Boys may have the alternatives of using playgrounds in the neighborhood for playing or
interacting with peers and they enjoy some freedom in social interaction, e.g. watching
football matches and other public activities. Most girls can only play in school and at
home, if they finish their house chores, although in urban areas some parents do recognize
adolescents’ need for social interaction and entertainment and those who can afford it, may
take their adolescent girls to public gardens or clubs.
There is very little information on social participation of youth. Elias indicated that 57.4%
of youth in Gadaref and 47.0% in Kassala are engaged in public social activities such as
environmental health programmes (cleaning), construction and tree planting. This indicates
the great potential for youth if mobilized and empowered for social participation.
Historically educated youth played a critical role in political transformation of Sudan and
were engaged in politics in universities. However, during last two decades violence among
students distorted that type of experience. But university students represent a small
pecentage of total youth population; the majority of them have been considered first time
voters in 2008 Election. After 1998, with political parties’ resumption of the activities,
some of them established youth sector. In some parties the youth have become a strong
group with a loud voice, but again youth political participation is largely urban-centered
and male dominated. Generally, there is lack of statistics and information on political
participation in rural areas, but in view of the high illiteracy rates, cultural restriction and
limited political functions in rural areas, and particularly pastoralists’ areas, youth
engagement in politics is expected to be limited.
One of the major developments concerning youth has been their heavy involvement in nongovernmental organizations and several youth groups have formed their own organizations.
However, youth work in many of the organizations is on voluntary basis to gain
experiences. The youth organizations are active in different areas such as raising awareness
on human rights, HIV/ AIDS and many have been involved in monitoring of election.
Table 3.4.6. Views of Youth in Kassala and Gedaref on Women Rights
Youth Views ( %) on
Kassala State
Gedaref State
Support
Oppose
Support
Oppose
91.8
6.8
94.4
Girls’ education
4.2
67.4
28.4
69.8
Women econ. Participation
24.4
5.4
93.2
4.8
Female marriage without consent of
93.0
parents
Suitable age for women marriage
116 27.4
36.0
14.8
40.6
20-23 years
23.8
Source: Compiled from Elias, 2008 (a) and Elias, 2008(b)
28.6
12-15 years
16-19 years
How youth view women rights is a critical indicator that reveals level of awareness and the
impact of their interaction within CSOs and with INGOs. Results of the youth study in
Gedarif and Kassala states, show significant changes as communities of the eastern Sudan
are known to be among the most conservative in the country in relation to women public
roles (Table 3.4.6.). The majority of youth surveyed in the two states support rights of
women for education and work, but still the majority opposes marriage without parents
consent and prefers early marriage for women. Thus, there is need to raise awareness of
youth as future leaders to change their perceptions and attitudes if the goals for women
empowerment and development are to be realized.
3.4.5.3. Policies, Strategies and Institutional Structures:
Historically governments’ programmes for youth focused on sports, vocational training,
and cultural activities. But youth issues have gained recognition from government and
development partners and these culminated in efforts to address some of the problems of
the youth sector. Interventions helped in the formulation of a strategic plan for youth
development, in addition to some capacity building and dialogue programmes.
Youth National Strategy (YNS) was formulated in 2007 and revised in 2010 to
accommodate changes in socio-economic context of the country. The strategy was based
on a survey on youth and consultations with different youth groups to determine priorities.
The objectives of YNS include:
a. capacity building in skills and knowledge as a means of empowering youth;
b. changing values among youth.
c. raising awareness of youth on politics, economics, environment and socioeconomic issues; d) enhancing youth participation in political, economic and social
activities; and
d. strengthening the capacity of Youth General Directorate.
There is a Five-Year Strategic Plan, 2007-2012, for youth but remains yet to be
implemented, mainly because of funding problems.
One important institution dealing with youth is the Youth Directorate, which has the
responsibilities of formulating strategies and coordination of Youth work between different
ministries. It has recently succeeded in facilitating and coordinating consultation for Youth
Strategy and Fiver-Year Strategic Plan. However, the Directorate is challenged by the
limited resources to undertake any major for development programme.
117 Other institutions for youth include: a) the Higher Councils for Youth and Sports were
established at the state levels by the MoCYS to oversee a number of programmes and
projects that target youth; b) These Higher Councils established Youth Parliaments whose
role is to develop policies and address challenges facing various programmeming in
relation to youth; c) Youth Centers and Boys’ Scouts and Girls’ Guides and all are
functioning in few areas and utilized by few groups of youth.
3.4.5.4. Programmeming for Youth:
From a programmematic perspective, it is worth mentioning the attempts for introducing
youth friendly services in some states, such as the White Nile and South Kordofan states
are yet to be realized. Standards for provision of youth friendly services have been printed
and disseminated. Observation and feedback from states that have attempted
implementation has shown many obstacles, including the lack of the appropriate set-up that
help to reach and mobilize youth- both male and female- as well as stigma related to youth
utilizing RH services.
The UN Agencies implemented a joint programme for creation and provision of small
financial grants to address the problem of youth unemployment. The intervention was
based on a survey on youth employment.
There has been consultation and surveys for formulation of YNS and worked extensively
with youth in five priority states supporting institutional capacity building, youth dialogue
forums and media advocacy for RH and HIV/AIDS issues.
Apparently any development for youth has to address macro-level contextual issues as well
as micro-level issues. The above mentioned programmemes have started a momentum
which needs to be strengthened and coordinated with an understanding of the socioeconomic and cultural constraints generating inequalities among youth.
3.4.5.5. Concluding Remarks:
Viewing youth situation from the perspective of human rights and human development is
strategic in thinking and supporting youth as potential leaders. With such perspective and
considering the above indicators of inequalities it is apparent that the majority of
adolescents and youth in Sudan are deprived from basic human rights and in all, even the
privileged, live stages when they are not given choices. Education does provide them with
skills and knowledge relevant to their life and needs; but does not help in creating critical
minded youth and independent thinking. Also, many adolescents and young men and
women are forced to drop education for family economic conditions of for lack of needed
educational facilities and services and those who continue do not choose the type of
education as these again are determined by limiting surrounding conditions. Most
adolescents and young men and women are forced to marry or are restricted in spouse
118 selection by families. Adolescents and young people are not informed about reproductive
rights and thus cannot claim it. If young people get married, they have to have children or
would be forced to divorce and remarry.
As most adolescents and youth, particularly in rural and nomadic areas, are not in
educational institutions and not participating in social life, they do not have opportunities
for accessing knowledge, using technology, experiencing dialogue or being exposed to
other cultures and life styles. Those who get to higher education may have such
opportunities; the challenge is how to provide such opportunities to the majority outside
educational institutions.
Historically there have been no strategies for social development of adolescents and youth
and the existing youth institutions are under-resourced, mostly not functional and not
accessible to all youth specifically in rural areas. Thus most of the youth lack awareness
and opportunities for social participation.
The interface of generational and gender inequalities is manifested by dynamics of
historical political, social and economic developments. It is important to note that
traditionally people acknowledge passage from childhood to manhood and womanhood,
thus generational differences among adolescents, youth and adults are not well recognized
or defined. This is evidenced by historical neglect to women and youth issues as well as
dominance by adult and males on all processes. These dynamics have constrained and
delayed momentum of youth movement.
Challenges:
There is lack of consensus on age of adolescents and youth and hence information on their
situation.
The heavy domestic responsibilities shouldered by adolescents and youth, particularly
females, constrain their opportunities for building their capabilities and accessing resources
and skills and opportunities that empower them.
The constraints to RR and RH are interrelated, the challenge is how to address adolescents
and youth poverty and help them to empower themselves to identify their cultural
boundaries and work for challenging related stigma, silence and exercise their RR.
An important challenge is how can youth bridge their political socio-economic and cultural
differences for developing common agenda for youth empowerment? How can youth work
for gender equality and women empowerment and also help in adolescents’ empowerment?
The existing institutions, such as student associations and youth parliaments, are essential
for addressing some of above problems and needs but the challenge is how to make them
inclusive and representative? Do youth living in nomadic areas know of these parliaments
or have they participated in electing parliamentarians? How many rural areas were reached
to ensure representation in youth parliaments? How many political parties are represented
in these parliaments?
119 Other challenges are: how to make youth centers and sports clubs educational institutions
filling gaps in health education, values related to rule of law and disciplined behavior, and
for fighting social diseases and mal-practices; and how to promote successful experiences
of using local media by youth to promote knowledge on reproductive and human rights and
the responsibilities of youth in community life.
Opportunities:
There are children and youth programmes in media which may be used to reach out to
adolescents
The active CSOs and CBOs may be oriented and mobilized to engage in addressing
adolescents issues
The available data can be utilized for advocacy.
Processes of legal reforms that can help in considering some rights for adolescents
and youth specifically for accessing RH services
Ministry of General Education is discussing reforms and this will be an opportunity
for revising population and reproductive health components in education curricula.
Initiatives among youth in Khartoum to organize themselves to promote youth civic
engagement
Some Development Partners may be interested to support youth development,
Youth development experiences exist in many neighboring countries.
Youth movements in neighboring countries developed political and social recognition
to strategic roles of youth in changing lives of their communities.
3.4.6. Recommendations:
Organize advocacy sessions and forums among adolescents and youth groups to identify
priority issues and their vision for addressing their needs to achieve social development.
Advocate among policy makers in all relevant areas for RR of youth and adolescents.
Involve in advocacy religious people from countries with good practices in youth RR and
RH.
Target faith-based groups by capacity building to advocate for youth RR and RH services
.
Evaluate youth situation and initiatives at community level and support their social/civic
engagement.
Support researches on youth in rural areas to provide information on diversity and poverty
of youth specifically in conflict areas. The information should be availed for youth to help
them understand their situations and responsibilities. The knowledge produced would also
be used advocacy, planning and programmeming.
120 For the time being, the establishment of Youth Friendly Services and centers should remain
a focus as pilot project in order to draw lessons and ensure community acceptance and
sustainability before further expansion.
Organize consultation with adolescents on different social issues through parents’ councils
in schools, the popular committees in villages and urban neighborhood and the sports’
clubs to gain trust and build confidence among adolescents and to help communities and
institutions to recognize them as a group. Select potential leaders among adolescents and
link them with youth groups working on RR, HIV/AIDS and RH to encourage them for
peer education.
121 SECTION FOUR:
PRIORITIES FOR UNFPA STRATEGIC INTERVENTIONS
UNFPA refined its strategic focus and accordingly the goal is: to achieve universal access
to RH (including family planning), to promote RR and reduce maternal mortality, and to
accelerate progress on ICPD agenda and MDG 5 (A and B) in order to empower and
improve the lives of underserved populations, especially women and young people
(including adolescents), enabled by an understanding of population dynamics, human
rights, and gender equality, and driven by country needs and tailored contexts.
The analysis has identified three interrelated critical problems for Sudan: high maternal
mortality, gender inequalities including marginalization of youth and adolescents and
prevalence of GBV. The three problems are caused by multiple inter-related factors
including: human rights and the laws, aligned to it, are not recognized/enforced in every
day practices and relationship and existence of discriminatory laws; prevalence of gender
inequality and male/elders’ dominance over decisions related to women and youth bodies,
fertility and choices; stereotypes and stigma related to adolescents and youth RH;
politicization of RH/RR and gender issues and resistance to programmes responsive to
women and youth needs; GBV practices such as FGM and early marriage, culturally
approved; priorities of government public spending and non-functional decentralization
limit locality resources directed to education and health; recurrent conflict and increased
vulnerability of women and youth to violence and deprivation; the culture is the most
influential factor on gender/generational inequality and negligence to RR and RH needs of
women adolescents and youth.
Taking in consideration the focus of UNFPA and the on-going programmes of UNFPA in
Sudan, the general guidelines for way forward are:
Build on strengths of previous programme and continue on supporting policy
formulation and dialogue at federal and state level;
Work to build culture of coordination and for integrated programming approaches
within UNFPA Sudan;
Focus on provision of data and analysis on population issues and dynamics
Take men in consideration when addressing youth and women priorities;
Shift programmes from state level to community level prioritizing the neglected
rural women and youth
Focus on partnership with CBOs and CSOs in delivering services and ensure
accountability to community and not government and that entails recognizing and
strengthening local ownership principle.
Gradually work in Darfur to shift to recovery and development considering
sustaining of women acquired skills and practices.
122 4.1. To put above guidelines in practice we suggest the following:
Pilot an integrated programme focusing on early marriage as priority issue linked to MM
and violation of rights of men and women and youth. The integrated activities include
policy and law reform, advocacy for FP and services for women including youth; raising
awareness for HIV/AIDS, provision of information and analysis on implications and
complications of early marriage and building capacities of youth for taking the lead of
advocacy. The proposed activities entail coordination within UNFPA programme units as
well as government sectors.
4.2. Maintain Reproductive Health and HIV/AIDS programme activities with new
focus and approach:
The recommendation in this connection is to continue working on strengthening
current initiatives for MM reduction, with result-oriented approach, while at the
same time exploring how to integrate RH and HIV/AIDs with empowerment of
women and youth. This can be done by piloting in one community in a state with
strong partnership to reach neglected groups.
Specific strategic consideration for improved RH and HIV/AIDS services:
Family Planning: Capacity building of potential providers, while enhancing MWs
role in FP.
Maternal death reviews: The need to broaden the circle of involved bodies
(implementation bodies, decision making bodies for resource allocation) including
CBS, with awareness creation on the need for MDRs.
EmONC: Pre-service training with medical institutions. Greater attention can be
given to neonatal care.
Health system support for RH: Support for harmonizing national monitoring and
evaluation activities,
Breaking the relative silence surrounding the HIV situation in Sudan; intensive
public education backed by strong community leadership is critical for eliminating
ignorance about the virus and sustaining the cult of silence.
Increased focus on targeted interventions for population at risk (FSWs, MSMs) and
other vulnerable population groups (tea sellers, military personnel, youth in and out
of school, truck drivers and populations of humanitarian concerns).
HIV prevention should be prioritized through appropriate awareness raising
interventions. Programmes should be implemented through communities with
focus on prevention in women and girls; condom programmeming; and prevention
for young people outside schools and other vulnerable groups.
4.2. Women Empowerment: Put in practice GM initiatives:
123 The strategic priorities for promoting empowerment of women/adolescent girls:
Gender-sensitive data for advocacy for empowerment of women /adolescent girls UNFPA
will contribute to provision of relevant gender-disaggregated data on rural women for
poverty analysis and identification of women empowerment deficit in different rural/
nomadic contexts taking the RR/RH as focus. Information produced should be used to
advocate for pro-poor gender sensitive plans and programmes for empowerment of women
and involvement of men, women and youth in poverty reduction processes at state/locality
level. GBV/ FGM should be core issues in advocacy.
Leadership committed to gender equality and reproductive well-being: UNFPA should
reconsider partnership with its local partners to strengthen their linkages to rural areas and
before that should ensure their commitment to women empowerment and reproductive
health improvement.
Culturally-relevant and gender-sensitive RH services: Assess capacities of existing RH
institutions and human resources and using information and assist locality to
enhance/reform its RH services to contribute to improved maternal health.
4.3. Adolescents and Youth:
Considering youth poverty situation and UNFPA on-going initiatives for youth and
mandates, the priority area for UNFPA programmeming is the empowerment of youth to
be agencies and leadership to pressure for changing their situation with a focus on their RR
and RH.
Young People’s Leadership and Participation: UNFPA will pay special attention to
working “with” young people through youth-adult partnerships. UNFPA will assess the
existing institutional mechanisms to identify partners for incorporating young people’s
input into policy and programmeming processes (including planning, implementation,
monitoring, and evaluation). It will continue investing in capacity building and leadership
skills of young people to make them advocates for their own rights and development
issues. UNFPA will promote peer educators as agents for transmitting safe RH messages,
linking peers with services, and allying with young people’s networks and coalitions.
UNFPA will tap into the dynamism of youth movements and their communication
networks for advocacy and action on issues of concern, such as, HIV/AIDS and early
marriage.
Gender-Sensitive, Life-Skills-Based Sexual and Reproductive Health Education: The focus
will be on inclusion of RH education in formal and informal education programme within
context of education reform and poverty reduction strategies.
124 Start by activating the pilot Centers established at the state level with support of UNFPA
with focus on social and civic engagement and gradually encourage the youth to break their
silence and demand the knowledge and service related to their RH needs
4.3. Build capacity of IDPS women for peace-building:
In collaboration with other Development Partners in Darfur and other conflict areas
consider strengthening on-going RH services, intensifying raising awareness campaigns on
RR and GBV.
Take initiative for starting a women leadership programmeme in IDPs camps.
Consider arranging consultations on how to sustain skills and practices learned in
resettlement context and if needed consider giving support for women to raise their voice
with their demands for new context.
4.4. Capacity Development:
The limitations of institutional and human resources capacities have been noted by analysis
as well as MTR as constraints for planning, programmeming and service delivery related to
RH, women and youth empowerment and population development. The limitations are
persistent despite that UNFPA and other Development Partners have been exerting
tremendous efforts for capacity development because: a) it is taken in its narrowest
perspective as training; b) it is not planned for achievements of results; c) most
interventions are not locally owned so people do not take responsibilities to monitor and
sustain results of training.
Accordingly there is need for a better understanding and approach to capacity
development52 if it is to be effective, result oriented and sustainable. Capacity
development is the process by which individual, groups, organizations, institutions and
societies increase their abilities to: a) perform core functions, solve problems and deal with
their development needs in a broad context and in sustainable manner. It is evident it is a
continual process of improvement within an individual, organizations or institutions not
one-time event. The aim is to build capacity to cope with change and to inculcate
integrated and holistic approach.
With this understanding, the approach is to plan capacity development to be responsive to
needs, result- oriented and sustainable. This can be achieved only if the programmemes’
processes are locally owned. The later can be built and maintained through intensifying
local consultations for need assessment and priorities’ identifications. The results of
capacity development must be specified and monitored by indicators.
52
Capacity development and capacity building are taken to have similar meaning and thus used
interchangeably.
125 In addition, capacity development must be planned with consideration to the external and
internal factors and dynamism. This means that the capacity development for family
planning must consider not only technical knowledge but political resistance, cultural
barriers and stereotypes related to different types of contraceptives. Training for RH health
of youth must tackle cultural sensitivities related to youth access and utilization of RH and
stigma related to STIs.
There is need to reconsider workshop training modality to be more result-oriented one. The
two relevant modalities are: a) in-house advisor to help in learning by doing; b) intensive
short training courses with built-in monitoring mechanisms. A complementary modality
for sustainability is long term training for expertise. These modalities should be done in
partnership with universities.
4.5. Coordination
Coordination emerges as a key strategic direction for appropriate implementation of all RH
interventions. Although some coordination mechanisms are in place within both national
programmes (NRHP and SNAP), execution is as yet inadequate to provide the full blown
support for timely achievement of the set targets.
Despite major integration efforts, RH and HIV/AIDS activities are being implemented in
isolation, due to the presence of two separate national structures, having different funding
mechanisms from their respective donors which render systematic and operational linkages
between RH and HIV/AIDS difficult to achieve. There is a need for greater integration of
RH and HIV/AIDS within UNFPA in terms of planning, coordination, implementation,
monitoring and evaluation. Likewise, the integration of RH, PD and gender dynamics as
well as coordination of humanitarian and development interventions emerges as a priority
in the coming phase.
Greater coordination with prospective partners and donors for more resource generation to
support RH programmemes is needed. This entails mapping of potential collaborators such
as NGOs, CBOs, faith-based organizations, academia, professional associations, and
private sector; all prospects for sectoral approach need to be explored. Civil society is one
of the key actors in implementation at ground level and there is a need to identify means of
involving civil society in a more coherent and coordinated manner due to its greater
acceptance within communities. The private sector functions autonomously and has not
been adequately tapped as a source of funding for RH interventions, despite its huge
potential in this respect.
In addition to the shortcomings in RH and HIV coordination, the gender and youth
components need to be coordinated with RH programmes for better results and effective
use of resources. The UNFPA MTR emphasized the importance of coordination of
programmeme components internally within UNFPA. The coordination among government
126 sectors is imperative for integration of population and gender issues and for addressing the
socio-cultural factors related to RH.
One major constraint for limited coordination is that it is not taken a guiding principle in
programmeming by government or by Development Partners although it is a basic
principle for aid.
To improve coordination UNFPA we suggest the following:
-UNFPA Sudan has to reconsider its structures and programmeming culture. First
coordination should be a core value monitored and staff hold accountable for it; secondly
the mandate of monitoring and evaluation unit should be extended to include coordination
and if needed capacity of unit should be enhanced to take additional responsibilities.
-Coordination should start at the level of need assessment and mapping undertaken for
different components to learn how it works at local level and identify the expected
constraints.
-In programme formulation, areas of coordination and related results should be identified
marked by indicators for monitoring.
-There is need to consider that coordination must be for activities within one component
and among components. Task Force or two from relevant ministries can be tried as
mechanism.
-At the state level the NPPP capacities must be enhanced for monitoring of coordination of
RH, PD, gender and youth issues. But technical assistance must given to her/him by
advisors (gender, youth and PD) appointed by UNFPA on retain contract basis for 20 days
in the year. They are to be responsible for preparing checklist for coordinated activities and
assisting in ensuring quality of results or in resolving any emerging problems. They are to
be in close contact with NPPP and to meet quarterly and participate in mid-term review
meetings. The Advisors and NPPP at state level should be working in close collaboration
with state authorities. As the coordination is not in culture of sectoral ministries, some
resistance may be met and this has to be anticipated and addressed by advocacy.
Partnership for coordination should also be tried to involve the CSOs and CBOs in
interventions. However, the Directorate of RH can lead coordination of RH activities by
formation of Task Force of two technical staff who are to work/coordinate with other
sectors. The coordination should be part of their official responsibilities for RH
Directorate. Task Force should be given needed training on coordination, indicators and
monitoring modality and should own the coordinated activities.,
-Sharing of results of needed assessment or mapping with other Development Partners in
important preliminary step for coordination. While consultation on programmeme content
should be undertaken with relevant UN Agencies or international organization to identify
127 areas of coordination and responsibilities and shared resources. The output of such
collaboration may be resisted by government ministries and institutions as there is
dependence on aid resources and to some officials coordination may reduce these
resources. .
128 REFERENCES
Abu Al Yaman, S.H., 2009, Final Analysis for Data of National Survey on Violence
against Women and Children. Sudan: Ministry of Justice, Unit of Ending Violence against
Women and Children.
Badri, etal, 2009, Survey of Women’s Political Participation in Eastern Sudan (Red Sea,
Kasala Gadanf). Report submitted to UN Women and Partners in Development Services,
Khartoum, Sudan.
De La Puente, 2011, ‘Women Leadership in Camps in Darfur, West Sudan’. Oxford
University Press and Community Development Journal, p365-377.
Elias, A.H., 2008 (a), Research Report on Youth Issues and Needs in the Sudan (Case
Study: Kasala state). Sudan: UNFPA
Elias, A.H., 2008 (b) Research Report on: Youth Issues and Needs in the Sudan (Case
Study Gadaref State). Sudan: UNFPA.
El Mahdi, A.R, 2011, Youth and Employment in Sudan. A consolidated report on labor
market survey findings from three Northern States: Blue Nile, North Kordofan and South
Kordofan States. Sudan: UNDP.
El Nager, elal, 2010, Gender Mainstreaming in National Development Policies and Plans:
North and South Sudan Country Studies. UNIFEM, East and Horn of Africa.
ElNager, Samia, 2011, Should I stay ? or should I go? Decision Time for Southern Sudan
People in Khartoum. Paper presented to the Regional Institute of Gender, Diversity, Peace
and Human Rights, Ahfad University for Women, Sudan.
General Directorate of Youth, Five-year Plan. 2012-2016 Khartoum: Ministry of Youth
and Sports.
Government of National Unity and Government of Southern Sudan, 2007, Sudan
Household Health Survey 2006.
Inclusive Security: Women Waging Peace, 2009, Addressing the Crisis in Darfur.
Mahmoud, M.M, 2009, Population growth and the state of Labour Force in Northern
Sudan. Data Dissemination Conference; The Fifth National Population Census. Sudan:
Ministry of Cabinet, Central Bureau of Statistics.
Mohamed, E. M..A., 2009, National study on Youth Issues and Challenges. Khartoum:
National Population Council and UNFPA
Okonji, G, 2011, Defending and Securing the Human Rights of Women and Girls in the
Humanitarian Crisis, South Darfur, Sudan – July 2008- July 2010. End of Programme
129 Evaluation of the UN Women and Unitarian Universalist Service Committee Funded
Programme.
Omer, S.KE., 2009, Gender Gap Analysis. Sudan: Central Bureau of Statistics.
Sahl, Ibramhim M.G., etal. 2011, Country Programme Mid-term Review 2009-2010.
Khartoum: UNFPA.
Sayed, M. and Elgaali, M., 2009, Literacy and Education, Sudan: Central Bureau of
statistics.
Sudan Federal Ministry of Health, 2010, Adolescents Health: Situation Analysis and Policy
Issues.
Sudan, Ministry of Finance, 2011, Sudan, Interim Poverty Reduction Strategy.
Sudan: Central Bureau of Statistics, 2008, The Fifth National Population Census, 2008
Sudan: Central Bureau of Statistics, 2009, Key Findings: National Baseline Household
survey 2009, Northern Sudan. Sudan: Ministry of Council of Ministers, Central Bureau of
Statistics and Ministry of Finance.
Sudan: Ministry of General Education, Statistical Year Book 2005-2006; 2007-2008; 20082009.
Sudan: Ministry of Youth and Sports, 2011, The National Youth Strategy 2007-2031
Sudan, Federal Ministry of General Education, Directorate General of Educational
Planning, 2008, Baseline Survey on Basic Education in the Northern States Final Report
June 2008
In Partnership with the Ministry of International Cooperation, European Commission (EC),
UNICEF and WFP
The IRIS Center, University of Maryland, 2010, Women’s Human Rights in Sudan: A
Gender Based Review and Analysis of the Sudanese Legal Framework.
UN Millennium Project, 2005, Taking Actions: Achieving Gender Equality and
Empowering Women. Task Force on Education and Gender Equality. UK and USA: Earth
scan.
UNDP, 2008, Human Development Report, 2007-2008.
World Bank, 2001, Northern Sudan Education Sector status Report.
Zahariadakis, S. 2007. Women Issues in Darfur. Report prepared for STAND, Canada.
130 World Health Organization, Department of Making Pregnancy Safer, Sudan Health Profile,
2009. www.who.int . Accessed September 2011
UNFPA, Strategic Plan 2008-2011; Accelerating Progress and National Ownership of the
ICPD PoA, 2007
UNFPA, Sudan Annual Report, 2008
Sudan Government of National Unity, FMOH, National Health Policy 2007
Sudan, FMOH, National Reproductive Health Policy, May 2010
Sudan, FMOH, Sudan Household Health Survey, 2010
Ministry of Welfare and Social Security, National Population Council general Secretariat,
Sudan Millennium Development Goals Progress Report, 2010
Sudan, National AIDs Council, National Strategic Plan and sectoral Plans on HIV/AIDs,
2004-2009
UNFPA, Technical Division, Population Situation Analysis Conceptual and
Methodological Guide, 2010
UNFPA, Midterm Review of 2008-2013 Strategic Plan, July 2011
UNFPA, Country Programme Midterm Review, Executive Report, 2009-2010
WHO, UNICEF, UNFPA, & WB, Maternal Mortality Trends 1990-2008, mdgs website,
accessed November 2011
Umbelli T.A, National Maternal Deaths Registration Office, Maternal death Reviews
Report, January- June 2011
Umbelli T. A., National Maternal Deaths Registration Office, Maternal death Reviews
Report, 2010
Sudan, FMOH/ UNDP/ GF/HSS/JICA, Sudan Primary Health Care Facility Survey,
December 2010
FMOH, NRHP, Sudan Maternal Mortality Reduction Proposal, 2008
FMOH/UNFPA, Barriers to Family Planning Survey, 2008
World Bank, Global Monitoring Report, MDGs and the Environment, 2008
Algaddal A.H., RH Needs Assessment (EmONC and MISP) in 5 states, 2011
UNFPA, Sudan Country programme Document, 2009-2012
131 United Nations, The Millennium Development Goals Report, 2011
Friel P. et al, Reproductive Health Commodity Security (RHCS) Status Assessment in
Sudan, June 2011
FMOH, Sudan National Health Sector Strategic Plan (draft) 2012-2016
FMOH & WB, Sudan Health Sector Report, June 2011
Azzat O. et al, Sudan National Health Accounts Country Report, 2008
Sudan, FMOH, Road map for Reducing Maternal and Newborn Mortality, 2010-2015
Sudan, DDR Commission Newsletter, November 2010
UNDP, DDR Fact Sheet, Dec 2008
Nicholas R. DDR in Sudan:; Too Little? Too late?, February 2011
Elmardi S., The price of Silence: HIV/AIDs Control in Sudan, December 2008
FMOH, SNAP, National HIV and AIDS Strategic Plan, 2010-2014
FMOH, SNAP, United Nations General Assembly Special Session on HIV/AIDS
(UNGASS) Report, 2008 – 2009
WHO/UNAIDS/ UNICEF, Epidemiological Fact Sheet on HIV and AIDS, September
2008
SNAP, Multi Sectoral HIV/AIDS Response Annual Report, 2010
Abdalla N. et al, Assessment of village Midwives in 5 states, 2011
FMOH, NRHP, National Midwifery assessment 2007
FMOH, NRHP, National EmOC Needs Assessment report, 2005
FMOH/UNICEF, NRHP, RH Communication Strategy, 2008
U.S Census Bureau, “The Method and Materials of Demography” Henry S. Shryock, Jacob
S. Siegel, and Associate. Fourth printing (rev), U.S Government printing office, Washington,
D.C. 1980
General Secretariat, National Population council, “Population Characteristics and Dynamics
in Sudan” 2007.
Central Bureau of Statistics, “Sudan Household Health Survey”1996.
132 Saif Al-Nasir, I. A. “Technical analytical report 2008” Unpublished paper, presented in the
Conference for dissemination of the 2008 census data, held by the Central Bureau of
Statisticsl 2011.
133