Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
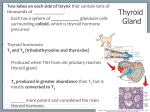
Chapter 26 Cancer of the Lung A D B C Table 26-1. Cancer of the lung. A, Squamous (epidermoid) cell carcinoma. B, Small-cell (oat-cell) carcinoma. C, Adenocarcinoma. D, Large-cell carcinoma. Slide 1 Copyright © 2006 by Mosby, Inc. Anatomic Alterations of the Lungs Inflammation, swelling, and destruction of the bronchial airways and alveoli Excessive mucus production Tracheobronchial mucus accumulation and plugging Airway obstruction Slide 2 Blood Mucus accumulation Tumor projecting into a bronchus Atelectasis Alveolar consolidation Cavity formation Pleural effusion Copyright © 2006 by Mosby, Inc. Etiology Slide 3 Lung cancer is the leading cause of cancer deaths in the United States More than 160,000 new cases are reported in the United States annually About 90,000 in males About 70,000 in females Copyright © 2006 by Mosby, Inc. Epidemiology Slide 4 In 2006, there were ~175,000 new cases of lung cancer in the United States. Second most common type of cancer in men and women WHO estimates ~2 million cases of lung cancer per year. It is the leading cause of cancer-related death. 85–90% of patients have a smoking history. Mosby items and derived items © 4 Copyright © 2006 by Mosby, Inc. Etiology Slide 5 The mortality rate for lung cancer in men recently has leveled off In women, however, the mortality rate is still rising—primarily because of the increased rate of cigarette smoking among women Among women, the lung cancer death rate is now higher than the death rate of any other cancer—including breast cancer Copyright © 2006 by Mosby, Inc. Etiology Slide 6 Cigarette smoking is the most common cause of lung cancer Heavy smokers are about 25% more likely to develop lung cancer than nonsmokers It is estimated that cigarette smoke contains about 4000 different chemicals—many of which have proved to be carcinogens Passive, or secondhand, smoking is associated with as much as a 30% increase in the risk of cancer Copyright © 2006 by Mosby, Inc. Epidemiology (cont.) Slide 7 Mosby items and derived items © 7 Copyright © 2006 by Mosby, Inc. Etiology Types of Cancers Small-cell lung cancer Slide 8 Small-cell (or oat cell carcinoma) Non–small-cell cancer Squamous cell carcinoma Adenocarcinoma Large-cell carcinoma Copyright © 2006 by Mosby, Inc. Lung Cancer Classification Classified as small cell or non–small cell carcinoma Non–small cell lung carcinoma (NSCLC) consists of Slide 9 Adenocarcinoma: most common type, ~40% of all lung cancers in United States Squamous cell carcinoma: 2nd most common type Large cell carcinoma: rarest form of lung cancer Small cell lung carcinoma (SCLC): ~20% of U.S. cases Mosby items and derived items © 9 Copyright © 2006 by Mosby, Inc. Table 26-1. Slide 10 Copyright © 2006 by Mosby, Inc. Pathophysiology Poorly understood Genetic material in lung cells damaged secondary to exposure to carcinogens, i.e., those in tobacco smoke There may be a genetic predisposition. The more genetic activation of the following pathways occurs; more likely, lung cancer’s growth is Slide 11 Stimulation of cell growth, differentiation, apoptosis, angiogenesis, tumor progression, immune regulation Mosby items and derived items © 11 Copyright © 2006 by Mosby, Inc. Clinical Features Slide 12 Mosby items and derived items © 12 Copyright © 2006 by Mosby, Inc. Diagnosis Slide 13 ~85% of patients will be symptomatic (see Box 28-2). Remainder detected by radiographic evaluation Chest radiograph and CT scan initial evaluation Will show nodules (<3 cm) and masses (>3 cm) Other findings: enlarged lymph nodes, effusions If radiograph, symptoms, history are very suggestive of malignancy may move straight to surgery If unsure if malignant or benign, further testing indicated Mosby items and derived items © 13 Copyright © 2006 by Mosby, Inc. Screening and Diagnosis Slide 14 Routine chest x-ray is the most common Computed tomography (CT) scan Positron emission tomography (PET) scan View a tissue sample (biopsy) under a microscope—used for a definitive diagnosis Copyright © 2006 by Mosby, Inc. Diagnosis (cont.) Adjunct imaging PET scan • Malignant cells are very metabolically active, take up radioactive glucose, scan reveals spots Slide 15 SPECT and contrast-enhanced CT used less often Nonsurgical tissue biopsy obtained by: Flexible bronchoscopy (FB): large airway growths • Saline washings, brushings, needle or forceps biopsy Transthoracic needle biopsy: peripheral masses • Shielded needle guided by fluoroscopy or CT Mosby items and derived items © 15 Copyright © 2006 by Mosby, Inc. Screening and Diagnosis Slide 16 Procedures used to obtain a tissue biopsy Bronchoscopy Mediastinoscopy Transbronchial needle biopsy Open-lung biopsy Sputum cytology Thoracentesis Video thoracoscopy Copyright © 2006 by Mosby, Inc. Staging of Lung Cancer Slide 17 Staging is the process of classifying information about cancer Cancer type Size of the tumor Level of lymph node involvement The extent to which the cancer has spread The patient’s prognosis and treatment depend on the staging results Copyright © 2006 by Mosby, Inc. Staging of Lung Cancer System most often used for staging lung cancer Slide 18 TNM classification T represents the extent of the primary tumor N denotes the lymph node involvement M indicates the extent of metastasis Roman numerals are used to identify stages 0 being the least advanced IV being the most advanced Copyright © 2006 by Mosby, Inc. Symbol Definition Primary tumor (T) T0 No evidence of tumor Tx Tumor that cannot be assessed Lymph nodes (N) Nx Regional lymph nodes cannot be assessed N0 Absence of regional lymph involvement Distant metastasis (M) Mx Metastasis cannot be assessed M0 Absence of distant metastasis Table 26-2. 1997 Revised International System for Staging Lung Cancer—Excerpts. Modified from Mountain CF: Revisions in the international system for staging lung cancer, Chest 111(6):1710, 1997. Slide 19 Copyright © 2006 by Mosby, Inc. Staging The staging of NSCLC is based on the TNM staging system (T: tumor, N: lymph node, M: metastases) “T” component of staging (extent of primary tumor) T1: 3 cm without invading local tissue T2: >3 cm may invade pleura or extend into bronchus, may cause segmental or lobar atelectasis T3: any size extends into surrounding structures, excluding main mediastinal structures. T4: any size invading mediastinal structures or presence of malignant pericardial or pleural effusion Slide 20 Mosby items and derived items © 20 Copyright © 2006 by Mosby, Inc. Staging (cont.) “N” component of staging (regional lymph node involvement) N0: no demonstrable involvement of nodes N1: ipsilateral nodal involvement N2: ipsilateral mediastinal lymph nodes N3: contralateral mediastinal or hilar nodal involvement, either sides involvement of scalene or supraclavicular lymph nodes “M” component of staging (metastases) M0: no metastases; M1: metastases present Slide 21 Mosby items and derived items © 21 Copyright © 2006 by Mosby, Inc. Staging (cont.) Staging of NSCLC Slide 22 Mosby items and derived items © 22 Copyright © 2006 by Mosby, Inc. Figure 26-2. Staging of lung cancer by the TNM classification system. (From McCance KL, Huether SE: Pathophysiology: The biologic basis for disease in adults and children, ed 4, St. Louis, 2002, Mosby.) Slide 23 Copyright © 2006 by Mosby, Inc. Staging (cont.) Staging of SCLC Divided into two groups Limited: cancer is confined to one hemithorax. • Includes ipsilateral mediastinal and supraclavicular nodes Slide 24 Extensive: cancer has spread beyond the original hemithorax. As staging guides therapy, it is important to determine the correct stage. Mosby items and derived items © 24 Copyright © 2006 by Mosby, Inc. Staging (cont.) Slide 25 Determination of staging for all lung cancers: CT of chest and upper abdomen is ordered for all. MRI only superior to CT scan for a Pancoast tumor FDG-PET best to determine staging of mediastinal nodes FB with transbronchial needle aspiration help for mediastinal staging Gold standard remains surgical resection and mediastinal dissection. Patient performance status is important in determining prognosis and ability to tolerate surgery. Mosby items and derived items © 25 Copyright © 2006 by Mosby, Inc. Overview of the Cardiopulmonary Clinical Manifestations Associated with CANCER OF THE LUNG The following clinical manifestations result from the pathophysiologic mechanisms caused (or activated) by Atelctasis (see Figure 9-7), Alveolar Consolidation (see Figure 9-8), and Excessive Bronchial Secretions (see Figure 9-11)—the major anatomic alterations of the lungs associated with cancer of the lung (see Figure 26-1). Slide 26 Copyright © 2006 by Mosby, Inc. Figure 9-7. Atelectasis clinical scenario. Slide 27 Copyright © 2006 by Mosby, Inc. Figure 9-8. Alveolar consolidation clinical scenario. Slide 28 Copyright © 2006 by Mosby, Inc. Figure 9-11. Excessive bronchial secretions clinical scenario. Slide 29 Copyright © 2006 by Mosby, Inc. Clinical Data Obtained at the Patient’s Bedside Vital signs Slide 30 Increased respiratory rate Increased heart rate, cardiac output, blood pressure Copyright © 2006 by Mosby, Inc. Clinical Data Obtained at the Patient’s Bedside Slide 31 Cyanosis Cough, sputum production, and hemoptysis Chest assessment findings Crackles Rhonchi Wheezing Copyright © 2006 by Mosby, Inc. Clinical Data Obtained from Laboratory Tests and Special Procedures Slide 32 Copyright © 2006 by Mosby, Inc. Pulmonary Function Study: Expiratory Maneuver Findings FVC FEVT N or FEF25%-75% N or FEF200-1200 N PEFR MVV FEF50% FEV1% N Slide 33 N or N N or Copyright © 2006 by Mosby, Inc. Pulmonary Function Study: Lung Volume and Capacity Findings VT Slide 34 RV FRC TLC N or VC IC ERV RV/TLC% N Copyright © 2006 by Mosby, Inc. Arterial Blood Gases Localized (e.g., Lobar) Lung Cancer pH Slide 35 Acute alveolar hyperventilation with hypoxemia PaCO2 HCO3 (Slightly) PaO2 Copyright © 2006 by Mosby, Inc. Time and Progression of Disease Disease Onset Alveolar Hyperventilation 100 90 PaO2 or PaCO2 80 Point at which PaO2 declines enough to stimulate peripheral oxygen receptors 70 60 PaO2 50 40 30 20 10 0 Figure 4-2. PaO2 and PaCO2 trends during acute alveolar hyperventilation. Slide 36 Copyright © 2006 by Mosby, Inc. Arterial Blood Gases Extensive or Widespread Lung Cancer Acute ventilatory failure with hypoxemia pH Slide 37 PaCO2 HCO3 (Slightly) PaO2 Copyright © 2006 by Mosby, Inc. Time and Progression of Disease Disease Onset Alveolar Hyperventilation Acute Ventilatory Failure 100 90 Pa02 or PaC02 80 70 Point at which PaO2 declines enough to stimulate peripheral oxygen receptors Point at which disease becomes severe and patient begins to become fatigued 60 50 40 30 20 10 0 Figure 4-7. PaO2 and PaCO2 trends during acute ventilatory failure. Slide 38 Copyright © 2006 by Mosby, Inc. Oxygenation Indices QS/QT DO2 VO2 Normal O2ER Slide 39 C(a-v)O2 Normal SvO2 Copyright © 2006 by Mosby, Inc. Hemodynamic Indices (When hypoxemia and acidemia are present, or when a tumor invades the mediastinum and compresses the superior vena cava) Slide 40 CVP RAP PA PCWP CO SV SVI CI RVSWI LVSWI PVR SVR Normal Copyright © 2006 by Mosby, Inc. Radiologic Findings Chest radiograph Slide 41 Small oval or coin lesion Large irregular mass Alveolar consolidation Atelectasis Pleural effusion Involvement of the mediastinum or diaphragm Copyright © 2006 by Mosby, Inc. Figure 26-3. Posteroanterior chest radiograph showing a large mass in the right upper lobe (arrows). Note the nodular density in the left lung field (circle). (From Rau JL, Jr., Pearce DJ: Understanding chest radiographs, Denver, 1984, Multi-Media Publishing.) Slide 42 Copyright © 2006 by Mosby, Inc. A B Figure 8-12. Chest radiograph identifying two suspicious findings: in the right upper lobe (A) and in the left lower lobe (B), just behind the heart (see white arrows). Slide 43 Copyright © 2006 by Mosby, Inc. A CT scan, upper right lobe B Chest radiograph CT scan, upper right lobe Figure 8-13. Same chest radiograph as shown in Figure 8-12. Note the CT scan also identifies the suspicious nodules and their precise location. Slide 44 Copyright © 2006 by Mosby, Inc. Coronal View Figure 8-14. PET scan: coronal views. The last three views show a “hot spot” in left lower lung lobe. Slide 45 Copyright © 2006 by Mosby, Inc. Figure 8-15. PET scan: sagittal views. The encircled images show a “hot spot” in the lower left lobe. Slide 46 Copyright © 2006 by Mosby, Inc. Axial View Figure 8-16. PET scan: axial view. A “hot spot” is further confirmed in left lower lung lobe. Slide 47 Copyright © 2006 by Mosby, Inc. Axial View No hot spot seen Figure 8-17. PET scan: axial view. This image confirms that the small nodule identified in the upper right lobe in the chest radiograph and CT scan is benign (i.e., no “hot spot” is evident). Slide 48 Copyright © 2006 by Mosby, Inc. CT Scan CT/PET Fusion PET Scan Axial View Coronal View Figure 8-18. CT/PET scan (center). CT scan, CT/PET fusion, and PET scan, all showing the same malignant nodule in right upper lobe (see white arrow). Note: The CT/PET fusion is normally presented in color (e.g., red, blue, yellow). Slide 49 Copyright © 2006 by Mosby, Inc. Figure 26-4. Bronchoscopic view of a tumor protruding into the right mainstem bronchus. A wire stent is in place to help hold the airway open. Slide 50 Copyright © 2006 by Mosby, Inc. Common Nonrespiratory Clinical Manifestations Hoarseness Difficulty in swallowing Superior vena cava syndrome Weakness Slide 51 Distention of the neck veins Neck and facial edema Electrolyte abnormalities Copyright © 2006 by Mosby, Inc. General Management of Cancer of the Lung Small-cell lung cancer Slide 52 Chemotherapy Radiation therapy Comfort (supportive) care Copyright © 2006 by Mosby, Inc. General Management of Cancer of the Lung Non–small-cell lung cancer Stage I and stage II Slide 53 Surgery is usually the treatment of choice Stage III Usually not good candidate for surgery May benefit from both radiation and chemotherapy Stage IV Chemotherapy alone Or no therapy, with comfort care Copyright © 2006 by Mosby, Inc. General Management of Cancer of the Lung Respiratory care treatment protocols Slide 54 Oxygen therapy protocol Bronchopulmonary hygiene therapy protocol Hyperinflation therapy protocol Aerosolized medication protocol Copyright © 2006 by Mosby, Inc. General Management of Cancer of the Lung BRONCHOSCOPY Slide 55 In addition to its role in diagnosis and staging, bronchoscopy may be used as part of: Photodynamic therapy Laser therapy Brachytherapy Placement of airway stents Copyright © 2006 by Mosby, Inc. Screening for Lung Cancer Slide 56 Due to the high proportion of patients who present with advanced lung cancer and its associated mortality, screening is very attractive. Techniques Chest radiograph and/or sputum exam • Studies did not support beneficial outcome. Low-dose CT imaging • No proof it is of any benefit • May be useful in high-risk individuals Mosby items and derived items © 56 Copyright © 2006 by Mosby, Inc. Treatment and Outcomes Slide 57 Mosby items and derived items © 57 Copyright © 2006 by Mosby, Inc. Prognosis for NSCLC Slide 58 Mosby items and derived items © 58 Copyright © 2006 by Mosby, Inc. Figure 26-5. Chest X-ray of a 66-year-old man with cancer of the lungs. Slide 59 Copyright © 2006 by Mosby, Inc.