Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
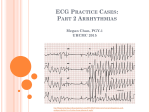
Supraventricular Tachycardia (SVT) Normal Heart The heart is an electrical pump. The SA (sinoatrial node), also known as the heart’s natural pacemaker, controls the heart rate. The SA node sends an electrical impulse and the atria (the top chambers of the heart) contract. The AV (atrioventricular node) then collects this impulse and sends it to the ventricles (the lower chambers of the heart) to contract. SVT SVT, (supra=above, ventricular=heart’s lower chambers, tachycardia=fast heart rate) means an abnormally fast heart rate coming from above the ventricles. In children, the two main types of SVT are accessory pathways and atrioventricular nodal reentrant tachycardia. An accessory pathway is when an impulse has been sent from the atria to the ventricles, through an extra electrical circuit. If this extra pathway is seen on the baseline ECG it is Wolf-Parkinson-White (WPW) syndrome. If this is not seen on the ECG it is called concealed WPW. Another type of SVT is called atrioventricular nodal reentrant tachycardia (AVNRT). This type of tachycardia has two pathways within the AV node: one is fast and one is slow. These two pathways let conduction move in two different directions. Signs and Symptoms Some children with SVT will say that their heart feels like it is racing. They may feel sweaty, short of breath, or dizzy. Infants may have trouble feeding or become lethargic or irritable. Some children have an increase in these symptoms when they have caffeine, are anxious, exercise, or take certain medicines. Testing A member of the health care team will do a complete exam and a health history. An ECG (EKG, or electrocardiogram) will be done to look at the heart’s electrical activity. If the child is having SVT at the time of the ECG, this will be seen on the ECG. A holter monitor may be used to show how often these episodes of rapid heart rate are happening. The monitor keeps recording the heart rhythm for 24 to 48 hours. This is very useful in infants, who can’t say what they are feeling. A 30 day event monitor can often be placed on older children. When the child feels their heart racing, they can press a button, and their heart rhythm is recorded. Treatment If your child has a rapid heart rate, there are things to try at home to stop the rapid heart rate. These are called vagal maneuvers as they increase vagal tone which can stop the fast heart rate (see below). If these maneuvers do not work after about 15 minutes or your child is not feeling or looking well, they need to be taken to the emergency department. In the emergency department an IV medicine may be needed to stop the fast heart rate, this is called Adenosine. Vagal Maneuvers-Older Children Bear down (as if trying to have a bowel movement) Close lips around your thumb and blow Vagal Maneuvers-Infants Check a rectal temperature Fill a small bag with an ice and cold water mixture and hold it on the infant’s face for 5-10 seconds There are many choices for treating SVT. No treatment may be needed if SVT doesn't happen often and if your child isn't upset when it does happen. When SVT happens often or it upsets your child’s everyday activities, medicines such as Digoxin or Propranolol may be used. For older children, an EP (electrophysiology) study and ablation may be done. This can take away the abnormal area of electricity or abnormal pathway. Your child’s cardiology provider will talk about these choices with you. Who Do I Call With Questions? Your child’s doctor, nurse or clinic staff can answer any questions. Our phone number is (608) 263-6420. Your health care team may have given you this information as part of your care. If so, please use it and call if you have any questions. If this information was not given to you as part of your care, please check with your doctor. This is not medical advice. This is not to be used for diagnosis or treatment of any medical condition. Because each person’s health needs are different, you should talk with your doctor or others on your health care team when using this information. If you have an emergency, please call 911. Copyright © 10/2014 University of Wisconsin Hospitals and Clinics Authority. All rights reserved. Produced by the Department of Nursing. HF#7698