Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
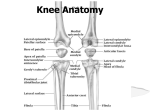
Knee Joint Articular surfaces : It is a large and complicated joint which includes 3 articulations : 1- between 2 condyles of femur / and upper surfaces of 2 tibial condyles. 2- between the patella / and patellar surface of femur. Type : 1-between the condyles of femur & tibia: is synovial hinge joint. 2-between the patella & femur : is synovial joint of plane gliding type. Capsule of Knee Joint Anteriorly : it is absent, replaced by pouching of synovial membrane upward beneath the quadriceps tendon, forming the suprapatellar bursa. On each side of patella : It is Lateral view strengthened by expansions from tendons of vastus lateralis & medialis. Posteriorly : 1- the capsule is strengthened by expansion of semimembranosus ms. called oblique popliteal ligament. 2- the capsule is pierced by popliteus tendon opposite the back of lateral condyle of tibia. Ligaments of knee Joint Extracapsular Ligaments : 1- Ligamentum patellae : -above, it is attached to lower border of patella./and below to tibial tuberosity. -it is a continuation of common tendon of quadriceps femoris ms. 2- lateral collateral ligament : -it is cordlike, attached above to lateral condyle of femur./and below to the head of fibula. -this ligament is not firmly adherent to the capsule. -It is separated from lateral meniscus by the tendon of popliteus ms. 3-Medial collateral ligament : -it is a flat band, attached above to medial condyle of femur./and below to medial surface of shaft of tibia. -it is firmly attached to medial lemniscus. 4- Oblique popliteal ligament -is a tendinous expansion of semimembranosus ms. -it strengthens the posterior aspect of the capsule. Ligaments of Knee Joint Intracapsular ligaments : 1-anterior cruciate ligament : Anterior veiw -inferiorly : it is attached to the anterior part of intercondylar area of tibia. -superiorly : attached to posterior part of medial surface of lateral condyle of femur. -it prevents posterior displacement of femur on tibia. With knee joint flexed, it prevents tibia from being pulled anteriorly. 2-posterior cruciate ligament : -inferiorly : it is attached to posterior part of intercondylar area of tibia. -superiorly : attached to anterior part of lateral surface of medial condyle of femur. -it prevents anterior displacement of femur on tibia. With knee joint flexed, it prevents tibia from being pulled posterioly. Posterior veiw 3- Two menesci : --are c-shaped sheets of fibrocartilage, placed between condyles of femur & tibia. --the peripheral border is thick and attached to the capsule, while the inner border is thin and concave and forms a free edge. Upper end of tibia --each meniscus is attached to upper surface of tibia by anterior & posterior horns. --because the medial meniscus is also attached to medial collateral ligament, it is relatively immobile. --Their function : 1- is to deepen the upper articular surfaces of tibial condyles to receive the convex femoral condyles. 2- they serve as cushions between the two condyles. Posterior aspect Synovial Membrane It lines the capsule and attached to the articular margins. On front and above the joint : it forms a pouch extending up beneath quadriceps femoris ms. for about 3 fingerbreadth above the patella, forming suprapatellar bursa., which helds in position by the attachement of a small portion of vastus intermedius, called articularis genu ms. At the anterior part of the joint : it is reflected from the back of ligamentum patellae to form infrapatellar fold ,/ the free borders of the fold is called, alar folds. /It encloses infrapatellar pad of fat. Synovial Membrane At the back of the lateral meniscus : it forms a pouch medial to popliteus tendon and separates the tendon from lateral meniscus & lateral femoral condyle. At the back of medial meniscus : -it forms the semimembranosus bursa -it may communicate with synovial cavity of the joint. At the back of the capsule : -It is reflected forward from the posterior part of the capsule around the front of cruciate ligaments, so cruciate ligaments lie behind the synovial membrane and not communicate with the synovial cavity (extrasynovial). Bursae of Knee Joint They are found wherever skin, ms. Or tendon rubs against bone. 4 are located in front of joint (anterior) / and 6 behind the joint (posterior). Suprapatellar bursa + popliteal bursa always communicate with the joint. / semimembranosus bursa may communicate with joint. Bursae of Knee Joint Anterior bursae : 1-suprapatellar bursa : lies beneath quadriceps ms. And communicates with joint cavity. 2-prepatellar bursa : lies in subcutaneous tissue between skin & front of lower part of patella + upper part of ligamentum patellae. 3-superficial infrapatellar bursa : lies in subcutaneous tissue between skin and front of lower part of ligamentum patellae. 4-deep infrapatellar bursa : lies between back of ligamentum patellae and tibia. Bursae of Knee Joint Posterior bursae : 1-popliteal bursa : lies in association with the tendon of popliteus and communicates with the joint cavity. 2-semimembranosus bursa : is found related to insertion of semimembranosus ms. And may communicate with joint cavity. 3- the remaining 4 bursae : are found related to : tendon of insertion of biceps + related to tendons of insertion of sartorius, gracilis, and semitendinosus muscles, lying beneath lateral & medial heads of gastrocnemius. Relations and Nerve Supply of Knee Joint Anteriorly : prepatellar bursa. Posteriorly : -popliteal vessels + L.Ns. -tibial N. + common peroneal N. -boundaries of popliteal fossa : upward & medially : semimembranosus & semitendinosus. Upward & laterally : biceps femoris. Downward & medially : medial head of gastrocnemius. Downward & laterally : lateral head of gastrocnemius. N.supply : 1-femoral N. 2-Obturator N. 3-Common peroneal N. 4-Tibial N. Medially : sartorius, gracilis, and semitendinosus. Laterally : biceps + common peroneal N. Movements of Knee joint 1- Extension : -It is produced by : quadriceps femoris. -It is accompanied by slight lateral rotation of tibia (or medial rotation of femur), because the medial condyle of femur is curved from before backwards, while the lateral condyle is straight. 2- Flexion : -by hamstring ms. : biceps, semitendinosus, and semimembranosus. -Assisted by : sartorius, gracilis, and popliteus. 3- Medial rotation : by sartorius, gracilis, and semitendinosus. 4- Lateral rotation : by biceps femoris. Meniscal injury of knee joint Injury of medial meniscus is injury of medial meniscus on more common than the lateral playing football. one, because of its strong attachment to the medial collateral ligament, which restricts the mobility of medial meniscus. The injury occurs when femur is suddenly rotated medially on tibia, with semiflexed knee joint specially in foot-ball players. The tibia is usually abducted on femur and medial meniscus is pulled into abnormal Tearing of medial meniscus of knee joint position between femoral & tibial condyles. Complete bucket handle tear Tearing of posterior part Tearing of peripheral part Tearing of anterior part Strength of Knee joint /and injury of its ligaments : The strength and stability of the joint depends largely on the strength of quadriceps femoris ms. + integrity of the ligaments that bind femur to tibia. Medial collateral ligament injury : -It is more common than the lateral one. -Partial tearing of the ligament can result from forced abduction of tibia on femur. -Sprains of medial collateral lig. result in tenderness over femoral or tibial attachments of ligament. Lateral collateral ligament injury : -it is less common than medial collateral lig. -it can result from forced adduction of tibia on femur. Strength of Knee joint /and injury of its ligaments : Cruciate ligaments injury : B, test for integrity of anterior cruciate ligament. C, test for integrity of posterior cruciate ligament. -Tears of anterior cruciate ligament are common than the posterior cruciate ligament. -it is accompanied by damage to other structures : collateral ligaments are commonly torn./ or the joint cavity fills with blood (hemarthrosis) and is swollen. -In ruptured anterior cruciate lig., tibia can be pulled excessively forward on the femur. –In ruptured posterior cruciate lig., tibia can be moved excessively backward on the femur. Joints of Foot : Subtalar (Talo-calcanean) Joint Articulation : : 1-inferior surface of body of talus. 2-facet on middle of upper surface of calcaneum. Type : plane synovial joint. Ligaments : medial, lateral talo-calcaneal ligaments + interosseous strong (talocalcaneal) ligament between sulcus tali & sulcus calcanei. Movements : Gliding and rotatory. Talo-calcaneonavicular Joint Articulation : 1-rounded head of talus. 2-upper surface of sustentaculum tali. 3-concave surface of navicular bone. Type : ball and socket synovial. Ligaments : plantar calcaneo-navicular ligament (Spring ligament) : -strong, between sustentaculum tali posteriorly & tuberosity of navicular bone anteriorly. Calcaneo-cuboid joint Articulation : 1-anterior end of calcaneum. 2-posterior surface of cuboid. Type : plane synovial. Ligaments : 1-bifurcated ligament : -strong y-shaped, lying on upper surface of joint. -stem : is attached to upper surface of anterior part of calcaneum. -lateral limb : attached to upper surface of cuboid bone. -medial limb : attached to upper surface of navicular bone. Lateral view Calcaneo-cuboid joint 2-Long plantar ligament : -strong ligament lying on the lower surface of joint. -between : undersurface of calcaneum & undersurface of cuboid + bases of 2nd , 3rd and 4th metatarsal bones. -it bridges over the groove for peroneus longus tendon, coverting it into a tunnel. 3-short plantar ligament : - strong ligament between undersurface of calcaneum and cuboid bones. Movements in Subtalar, Talo-calcaneonavicular, and Calcaneo-cuboid Joints : Talo-calcaneonavicular + calcaneo-cuboid joints are referred to as midtarsal or transverse tarsal joints. Inversion + eversion of foot take place in subtalar + transverse tarsal joints. Inversion is performed by : tibialis anterior, tibialis posterior, extensor H.L + medial tendons of extensor D.L. Eversion is performed by : peroneus longus, peroneus brevis, and peroneus tertius. Lateral tendons of extensor digitorum longus assist. Femoral nerve injury (L2,3,4) Causes : By stab or gunshot wounds, but a complete division is rare. Motor changes : 1-quadriceps femoris muscle is paralyzed and knee cannot be extended. In walking, This is compansated for to some extend by the action of adductor ms. Sensory changes : 1- loss of skin sensation over anterior & medial sides of thigh. ( intermediate + medial cutaneous N. of the thigh injury). 2-loss of sensation over medial side of leg + medial border of foot as far as the ball of big toe. (saphenous N. injury) Sciatic nerve injury (L4,5/S1,2,3) Causes : 1-penetrating wounds. 2-fractures of pelvis or dislocation of hip joint. 3-wrong injections into gluteus maximus or medius ( upper outer quadrant of the buttock is the best site). In 90% of cases, common peroneal part of the sciatic N. is the most affected because its fibres lie most superficial in sciatic N. Motor changes : 1-paralysis of hamstring ms., but weak flexion of knee is possible by the action of sartorius (Femoral N.) + gracilis (obturator N.). 2-paralysis of extensors of the leg, leading to foot drop. Sciatic nerve injury Sensory changes : (L4,5/S1,2,3)