Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Gene therapy of the human retina wikipedia , lookup
Focal infection theory wikipedia , lookup
Gene therapy wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Infection control wikipedia , lookup
Clinical trial wikipedia , lookup
Index of HIV/AIDS-related articles wikipedia , lookup
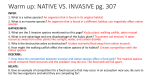
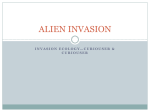
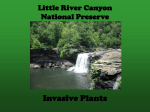
SUPPLEMENT ARTICLE Design of Efficacy Trials of Cytokines in Combination with Antifungal Drugs Bart Jan Kullberg, Astrid M. L. Oude Lashof, and Mihai G. Netea Department of Medicine, Radboud University Medical Center, and Nijmegen University Center for Infectious Diseases, Nijmegen, The Netherlands Resolution of invasive fungal infections is often dependent on recovery from an immunocompromised state, which indicates that host defense mechanisms are extremely important in the clearance of fungal pathogens. Immunotherapy aimed at enhancement of host defense mechanisms may improve clinical outcome of invasive mycoses. The design of trials of immunotherapy against fungal pathogens requires profound knowledge of the host defense mechanisms that are involved in invasive fungal infections. Prospective phase II studies with recombinant granulocyte colony-stimulating factor and interferon-g have been done. Recombinant interferong is a candidate for phase III trials of adjunctive immunotherapy for cryptococcal meningitis, invasive aspergillosis, and candidemia, but the proper design of future trials will be crucial to establish whether immunotherapy is of clinical value in the treatment of invasive fungal infections. Recently, great progress has been made in the development of antifungal therapy. New classes of antifungal drugs have been introduced that show promise for achieving cure from infection and a lower incidence of adverse effects [1–3]. For patients with invasive aspergillosis, therapy with voriconazole—a new triazole antifungal—has significantly increased the survival rate, and other new antifungal agents may have similar benefits [2]. Despite these developments, treatment failure is still a significant problem, occurring in 20%–30% of patients with the most common opportunistic fungal infections [2, 4, 5]. In specific groups of patients, such as those with persistent neutropenia, failure rates are even substantially higher [6]. Resolution of invasive fungal infections is often dependent on recovery from granulocytopenia or restoration of cellular immunity, which indicates that host defense mechanisms are extremely important in the clearance of these pathogens. Therefore, immunotherapy aimed at enhancement of host defense mechanisms may prove extremely useful. The design of trials of immunotherapy against fungal Reprints or correspondence: Dr. Bart Jan Kullberg, Dept. of Medicine (541), Radboud University Medical Center, P.O. Box 9101, 6500 HB Nijmegen, The Netherlands ([email protected]). Clinical Infectious Diseases 2004; 39:S218–23 2004 by the Infectious Diseases Society of America. All rights reserved. 1058-4838/2004/3908S4-0010$15.00 S218 • CID 2004:39 (Suppl 4) • Kullberg et al. pathogens brings about several specific difficulties and requires profound knowledge of the host defense mechanisms involved in invasive fungal infections. HOST DEFENSE MECHANISMS AND TARGETS OF IMMUNOTHERAPY The first step in the host defense is initiated by adhesion of the pathogen to the body surface of the host. Aspergillus conidia are inhaled into the lungs, attach to the alveolar lining, and are subsequently eliminated through phagocytosis by pulmonary alveolar macrophages (figure 1). Conidia that escape the alveolar macrophages eventually germinate into hyphae, which invade and destroy the alveolar epithelium, leading to tissue invasion. Similarly, in disseminated candidiasis, these steps are represented by elimination of the Candida conidia by bloodstream phagocytes or by adhesion of the conidia to the vascular endothelium, hyphal outgrowth, invasion and destruction of the endothelial cells, and tissue invasion (figure 1). Once tissue invasion has developed, the fungal antigenic structures are recognized and ingested by dendritic cells and tissue macrophages, which leads to activation of the innate and acquired hostresponse mechanisms. Mannoprotein constituents of the fungal cell wall are able to induce the production of proinflammatory or Th1 cytokines, such as TNF-a, tions in specific immunocompromised patient groups at risk, it may be feasible to apply immunomodulatory agents as a single drug, without concomitant antifungal prophylaxis. Such strategies aim at specifically restoring the impaired host defense mechanisms against a wide variety of pathogens, ideally rendering antimicrobial prophylaxis redundant. From animal models, a variety of immunomodulatory strategies have been suggested to be most promising, for example, substitution of the recombinant Th1 cytokine IFN-g or IL-18 or blocking of the Th2 cytokine IL-4 or IL-10 with monoclonal antibodies or soluble cytokine receptors [12–15]. Very recently, insight into the early recognition and signal transduction pathways involved in the host defense against invasive fungi has opened new options for immune intervention at the level of the cellular receptors for pathogens, among which the Toll-like receptors (TLRs) are the most important. Figure 1. Initial host defense against invasive fungal pathogens. The first line of defense consists of phagocytosis by pulmonary alveolar macrophages, in the case of inhaled pathogens, or by peripheral blood phagocytes, in the case of bloodstream infection. Microorganisms that evade the first line of defense may germinate into hyphae, penetrate and damage the epithelial lining, and invade the tissues. Immune recognition subsequently leads to both recruitment of polymorphonuclear leukocytes (PMNL) and monocytes and activation of these cells to kill the microorganisms. IL-12, and IFN-g, which are required for the immune response against invasive fungal infection (figure 2). In experimental models, the development of Th1 protective immunity is correlated with resistance to a lethal infection, and neutralization of endogenous TNF-a or IFN-g has deleterious effects on the course of fungal infections [7]. Conversely, production of the Th2 cytokines IL-4 and IL-10 is associated with disease progression in experimental models [8]. Indeed, recent observations have confirmed that high concentrations of IL-10 or low IFN-g/IL-10 production ratios are associated with a poor outcome in patients with aspergillosis [9, 10]. Stem cell transplant recipients, in particular those receiving steroids, have a Th2-biased cytokine response, rendering them susceptible to invasive fungal infections [10]. Ultimately, proper activation of the cytokine network leads to an increasing number of phagocytic cells—that is, polymorphonuclear leukocytes and monocytes or macrophages—at the site of infection and to an activation of these cells to kill the pathogenic fungal organisms more effectively. Immunotherapeutic strategies, therefore, should target modulation of the host response toward a favorable Th1/Th2 balance, leading to enhanced activity of cytokines such as IL-1, TNF-a, IL-18, and IFN-g, which are required for effector cell activation against fungal pathogens [11]. For therapy of established invasive fungal infections, immunomodulatory agents are to be used as adjunctive therapy, in combination with an optimal selection of antifungal agents. In contrast, for prevention of invasive infec- TLRS AS POTENTIAL TARGETS FOR IMMUNOMODULATION TLRs are pattern-recognition receptors that have a central role in the innate immunity to pathogens (figure 3). Initially identified in Drosophila as a gene required for ontogenesis, Toll has been shown to control the expression of the gene encoding for the antifungal peptide drosomycin and to be crucial for the antifungal response of the insect [16]. Because of the homology Figure 2. The cytokine network in host defense against invasive fungal infections. Recognition of antigenic fungal structures leads to release of IL-12, IL-18, and TNF-a, which both stimulate natural killer (NK) cells to produce IFN-g and mount a Th1-type T cell response, further enhancing IFN-g production and subsequently activating oxidative and nonoxidative mechanisms of fungal killing. Stimulation of a Th2-type immune response inhibits IFN-g production through IL-4 and IL-10. G-CSF, granulocyte colony-stimulating factor; GM-CSF, granulocyte-macrophage colony-stimulating factor; PMNL, polymorphonuclear leukocytes; NO, nitric oxide. Antifungal Immunotherapy • CID 2004:39 (Suppl 4) • S219 Figure 3. The role of Toll-like receptors (TLRs) in host defense against invasive candidiasis. Cell-wall constituents of Candida blastoconidia stimulate both TLR2 and TLR4 on host macrophages, leading to intracellular signaling and induction of cytokine mRNA. Whereas TLR4 is the major receptor involved in the stimulation of chemokines, such as IL-8, with subsequent recruitment of inflammatory cells at the site of infection, TLR2-mediated signals stimulate the production of anti-inflammatory cytokines, such as IL-10, and immunosuppressive T-regulatory cells. MD-2, myeloid differentiation; MyD88, myeloid differentiation factor 88; TIR, Toll/interleukin-1 receptor; TRIF, TIR-domain–containing adaptor inducing interferon-beta; TICAM, TIRcontaining adaptor molecule-1; TIRAP, TIR-domain–containing adaptor protein. of the Toll intracellular domain with that of the IL-1 receptor type I, it has been hypothesized that homologues of Toll may also be present in mammalian cells and may be involved in antimicrobial resistance. Indeed, at least 10 human TLRs have been identified to date, some of them with crucial roles in the recognition of pathogen-associated molecular patterns: TLR4 for lipopolysaccharide and lipoteichoic acid; TLR2 for peptidoglycans, lipoarabinomannan, and bacterial lipoproteins; and TLR9 for bacterial DNA [17–19]. Accumulating data have suggested an important role of the TLRs in the mammalian antifungal defense. TLR2 is involved in the recognition of zymosan, a cell-wall particle of the yeast Saccharomyces cerevisiae [20], whereas TLR4 has been suggested to mediate intracellular signaling after stimulation of cells with Cryptococcus neoformans glucuronoxylomannan [21]. We have recently shown that induction of chemokines and leukocyte recruitment at the site of invasive Candida infection is TLR4 dependent [22]. Polymorphisms in the TLR4 gene have been associated with hyporesponsiveness to lipopolysaccharide and with increased risk for gram-negative sepsis [23], and preliminary data from our laboratory suggest similar findings in Candida albicans infection. Interestingly, TLR2 and TLR4 also appear to exert divergent and even opposing functions in the host defense against invasive mycoses [24, 25]. Whereas Aspergillus fumigatus conidia stimulate both TLR2 and TLR4 to induce a Th1 cytokine response, germination of Aspergillus into hyphae leads to the loss of TLR4-mediated Th1 induction, whereas Th2-biased signaling through TLR2 remains intact. This dysbalance leads to S220 • CID 2004:39 (Suppl 4) • Kullberg et al. IL-10 production and impaired host defense against invasive disease through loss of TLR4-mediated signals [25]. Likewise, C. albicans evades the host response through stimulation of TLR2 [24]. Whereas TLR4 is the major receptor involved in the stimulation of chemokines, such as IL-8, with subsequent recruitment of inflammatory cells at the site of infection, TLR2mediated signals stimulate the production of anti-inflammatory cytokines, such as IL-10, and immunosuppressive T-regulatory cells [24]. These observations suggest that modulation of the TLR signaling pathways may be explored as an immune intervention, with the aim of correction of the immunosuppressive properties of invasive hyphal growth and stimulation of a Th1type cytokine response. CURRENT STATUS OF IMMUNOTHERAPY Although case reports have suggested successful application of recombinant IFN-g, granulocyte colony-stimulating factor (GCSF), or macrophage colony-stimulating factor for patients with refractory mycoses, prospective studies of cytokine therapy in patients with invasive fungal infections have begun only very recently. The first randomized placebo-controlled study addressing adjunctive immunotherapy for invasive mycoses compared fluconazole alone with fluconazole and recombinant (r) G-CSF in nonneutropenic patients with disseminated candidiasis [26]. The results of this phase II pilot study indicate that adjunctive therapy with rG-CSF is safe and may be given to patients with invasive candidiasis or candidemia. Although this study was not planned to detect a statistically significant effect of rG-CSF on outcome of infection, a trend toward faster resolution of infection was found—the median time to resolution of infection was 21 days in placebo-treated patients versus 14 days in rG-CSF–treated patients (hazard ratio [HR], 1.88; 95% CI, 0.90–3.92). The HRs suggest that patients treated with rGCSF were about twice as likely to resolve their infection as were placebo-treated patients, and a similar beneficial trend was seen in mortality (HR, 0.49; 95% CI, 0.15–1.63) [26]. A second phase II double-blind, placebo-controlled study has evaluated adjuvant rIFN-g in the treatment of HIV-infected patients with acute cryptococcal meningitis [27]. Patients received rIFN-g or placebo 3 times weekly for 10 weeks plus standard therapy with intravenous amphotericin B followed by fluconazole. At 2 weeks, conversion of the results of cerebrospinal fluid culture for fungi from positive to negative occurred in 38% of rIFNg recipients, compared with 18% of patients receiving only antifungal therapy (P 1 .05). At the end of the study, serum cryptococcal antigen titers had decreased by 50–70-fold in the IFN-g treatment group versus 24-fold in the placebo group. Although the rates of conversion of culture results and survival at week 10 were similar across treatment groups, 62% of subjects showed improved combined mycological and clinical outcome in the active treatment arm, compared with 48% in the placebo arm (P 1 .05). The immunotherapy was well tolerated, with few adverse events and no obvious influence on HIV infection [27]. Whereas these 2 pilot studies provide no proof of the efficacy of antifungal immunotherapy in clinical practice, they have provided valuable information on the safety and applicability of immunomodulators in patients with invasive mycoses, opening ways to do future phase III studies. On the basis of the current insights on host defense mechanisms, it appears that rIFN-g may be a major candidate for further studies on adjunctive immunotherapy. Phase III trials on treatment of cryptococcal meningitis and invasive aspergillosis and a phase II study of patients with candidemia are under way. Future phase I studies may address the use of rIL18 in the treatment of patients with candidemia and the use of anti–IL-4 or anti–IL-10 strategies for patients with invasive aspergillosis. TRIAL DESIGN Clinical trials of potential adjunctive immunotherapeutic agents serve 2 major goals: to demonstrate clinical effectiveness and safety and to generate data that support registration of new agents for the treatment of these potentially lethal conditions. The prospective, randomized, controlled trial remains the reference standard for achieving these goals. However, comparative trials of antifungal therapies pose several problems. First, the large sample size required for randomized, controlled clinical trials is an obstacle to the use of such trials to study a disease that is relatively rare. Second, invasive mycoses usually occur in patients with complex and divergent underlying conditions, which makes the interpretation of the outcome parameters and safety issues extremely complex [28]. Third, the budgets of small biotechnology companies developing immunomodulatory agents are limited, precluding funding of large, sufficiently powered trials in the complex area of invasive mycoses. For any choice of combination therapy, the combination of the 2 drugs should be superior to either drug alone, because it would not be rational to add to a standard treatment regimen a second drug with no additional benefit that would have additional costs and adverse effects. This also applies to the combination of an antifungal drug with an immunomodulator. Thus, combination therapy trials should be designed to demonstrate superiority, rather than equivalence, of the combination. In addition, because any immunotherapeutic agent is likely to be highly expensive, the treatment benefit should be not only statistically significant but also clinically relevant in terms of the resolution of infection or the reduction of mortality. It is highly unlikely that a statistically significant but clinically negligible effect on mortality would lead to clinical use of an expensive immunomodulatory drug. Therefore, as a first step to establish a potential clinical advantage of immunomodulatory adjuvant therapy, a phase II study design aimed at the detection of only very strong effects of immunotherapy (e.g., a 20% improvement of outcome) may be rational. This goal would require fewer patients and resources, and although the vast majority of regimens will fail to demonstrate such strong effects, any positive finding would have a much better chance of becoming an established immunomodulatory strategy in the future. Subsequently, agents selected by this strategy should be further tested in a phase III efficacy trial before being applied in clinical practice. Other, albeit less likely, concerns of combination therapy studies include the possibility that the immunomodulatory agent may influence the pharmacokinetics of the antifungal drug or vice versa. This possibility requires the monitoring of drug concentrations to be incorporated into the study protocol. Finally, whereas conventional antifungal agents have been shown to be active as single agents, before being studied in combination therapy trials, adjuvant immunomodulatory drugs have not been studied as monotherapy for patients with invasive fungal infections. Thus, despite the careful selection of an immunomodulator on the basis of preclinical studies, a theoretical possibility exists that the immunomodulator may worsen the course of infection in the specific patient population under study. Whereas models have been established to predict the best design of clinical combination therapy trials in terms of dose finding [29], interference of an immunomodulator with the complex cytokine network in vivo during clinical disease may not be as predicted, and the study design and safety monitoring should be aimed at detection of such unwanted effects. Antifungal Immunotherapy • CID 2004:39 (Suppl 4) • S221 The two goals of immunotherapy trials—to develop clinical treatment strategies and to license immunomodulatory agents— may require different designs. For registration, trial patient populations usually have to match the wide variety of patient characteristics that are encountered in clinical practice (e.g., age, comorbid disease, concomitant drugs, and neutrophil count). Likewise, trial end points have to reflect clinically relevant outcomes (e.g., microbiological cure and 90-day survival). In contrast, development of new and innovative therapeutic strategies necessitates trial patient populations that do not interfere with the assessment of the potential benefit of immunomodulation. Such confounders may be neutropenia, the use of corticosteroids or other immunomodulators, or the presence of refractory underlying disease. To obtain a proof of principle, patients with such conditions may have to be excluded from phase II immunotherapy trials. Alternatively, study populations may be stratified for a limited number of such factors. To assess the potentially beneficial effects of adjunctive immunomodulatory treatments compared with antifungal therapy alone, standard microbiological and survival end points may not be sensitive enough to identify promising strategies. This problem is magnified by the difficulties of both funding and executing sufficiently large studies and by the presence of comorbid diseases. In overcoming these hurdles, immunomodulatory strategies have the unique property of affecting immunologic parameters that may act as surrogate markers. The Th1/Th2 cytokine balance or the ex vivo fungicidal activity of peripheral blood neutrophils or mononuclear cells are potential candidate surrogate markers in clinical trials, because substantial experimental evidence suggests that these factors correlate with the outcome of infection. Such surrogate markers are likely to be extremely useful for selection of adjuvant strategies and for dose finding in relatively small phase I and II pilot studies of patients with invasive mycoses. In turn, for promising agents that show potential benefits in these initial studies, relevant clinical end points should be used in combination with immunologic markers in subsequent randomized or open-label phase II and III trials, and the licensing of immunomodulatory therapy should be based on sound clinical end points rather than on surrogate markers. In conclusion, whereas the limited interest and budgets of biotechnology companies are a major hurdle in performance of clinical trials, strategies to modulate host defense are expected to be an invaluable addition in the armamentarium against invasive fungal infections. The design of relatively small clinical trials that use alternative patient-inclusion and outcome criteria may accelerate development of new immunotherapeutic therapies. S222 • CID 2004:39 (Suppl 4) • Kullberg et al. Acknowledgment Potential conflicts of interest. B.J.K. is a consultant for Pfizer and Schering-Plough. A.M.L.O.L. and M.G.N.: No conflict. References 1. Walsh TJ, Finberg RW, Arndt C, et al. Liposomal amphotericin B for empirical therapy in patients with persistent fever and neutropenia. N Engl J Med 1999; 340:764–71. 2. Herbrecht R, Denning DW, Patterson TF, et al. Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis. N Engl J Med 2002; 347:408–15. 3. Mora-Duarte J, Betts R, Rotstein C, et al. Comparison of caspofungin and amphotericin B for invasive candidiasis. N Engl J Med 2002; 347: 2020–9. 4. Anaissie EJ, Rex JH, Uzun O, Vartivarian S. Predictors of adverse outcome in cancer patients with candidemia. Am J Med 1998; 104:238–45. 5. Rex JH, Pappas PG, Karchmer AW, et al. A randomized and blinded multicenter trial of high-dose fluconazole plus placebo versus fluconazole plus amphotericin B as therapy for candidemia and its consequences in nonneutropenic subjects. Clin Infect Dis 2003; 36:1221–8. 6. Denning DW. Therapeutic outcome in invasive aspergillosis. Clin Infect Dis 1996; 23:608–15. 7. Netea MG, Van Tits LHJ, Curfs JAHJ, et al. Increased susceptibility of TNF-a/LTa double knockout mice to systemic candidiasis through impaired recruitment of neutrophils and phagocytosis of Candida albicans. J Immunol 1999; 163:1498–505. 8. Cenci E, Mencacci A, Fe d’Ostiani C, et al. Cytokine- and T helper–dependent lung mucosal immunity in mice with invasive pulmonary aspergillosis. J Infect Dis 1998; 178:1750–60. 9. Roilides E, Sein T, Roden M, Schaufele RL, Walsh TJ. Elevated serum concentrations of interleukin-10 in nonneutropenic patients with invasive aspergillosis. J Infect Dis 2001; 183:518–20. 10. Hebart H, Bollinger C, Fisch P, et al. Analysis of T-cell responses to Aspergillus fumigatus antigens in healthy individuals and patients with hematologic malignancies. Blood 2002; 100:4521–8. 11. Kullberg BJ, Anaissie EJ. Cytokines as therapy for opportunistic fungal infections. Res Immunol 1998; 149:478–88. 12. Kullberg BJ, Van ’t Wout JW, Hoogstraten C, Van Furth R. Recombinant interferon-g enhances resistance to acute disseminated Candida albicans infection in mice. J Infect Dis 1993; 168:436–43. 13. Stuyt RJL, Netea MG, Verschueren I, et al. Role of interleukin-18 in host defense against disseminated Candida albicans infection. Infect Immun 2002; 70:3284–6. 14. Puccetti P, Mencacci A, Cenci E, et al. Cure of murine candidiasis by recombinant soluble interleukin-4 receptor. J Infect Dis 1994; 169: 1325–31. 15. Romani L, Puccetti P, Mencacci A, et al. Neutralization of IL-10 upregulates nitric oxide production and protects susceptible mice from challenge with Candida albicans. J Immunol 1994; 152:3514–21. 16. Lemaitre B, Nicolas E, Michaut L, Reichhart JM, Hoffmann JA. The dorsoventral regulatory gene cassette spatzle/Toll/cactus controls the potent antifungal response in Drosophila adults. Cell 1996; 86:973–83. 17. Poltorak A, He X, Smirnova I, et al. Defective LPS signaling in C3H/ HeJ and C57BL/10ScCr mice: mutations in Tlr4 gene. Science 1998; 282:2085–8. 18. Takeuchi O, Hoshino K, Kawai T, et al. Differential roles of TLR2 and TLR4 in recognition of gram-negative and gram-positive bacterial cell wall components. Immunity 1999; 11:443–51. 19. Underhill DM, Ozinsky A. Toll-like receptors: key mediators of microbe detection. Curr Opin Immunol 2002; 14:103–10. 20. Underhill DM, Ozinsky A, Hajjar AM, et al. The Toll-like receptor 2 is recruited to macrophage phagosomes and discriminates between pathogens. Nature 1999; 401:811–5. 21. Shoham S, Huang C, Chen JM, Golenbock DT, Levitz SM. Toll-like receptor 4 mediates intracellular signaling without TNF-a release in response to Cryptococcus neoformans polysaccharide capsule. J Immunol 2001; 166:4620–6. 22. Netea MG, Van der Graaf CAA, Vonk AG, Verschueren C, Van der Meer JWM, Kullberg BJ. The role of Toll-like receptor (TLR) 2 and TLR4 in the host defense against disseminated candidiasis. J Infect Dis 2002; 185:1483–9. 23. Arbour NC, Lorenz E, Schutte BC, et al. TLR4 mutations are associated with endotoxin hyporesponsiveness in humans. Nat Genet 2000; 25: 187–91. 24. Netea MG, Sutmuller R, Hermann C, et al. Toll-like receptor 2 suppresses immunity against Candida albicans through induction of IL10 and regulatory T cells. J Immunol 2004; 172:3712–8. 25. Netea MG, Warris A, Van der meer JWM, et al. Aspergillus fumigatus evades immune recognition during germination through loss of Toll-like receptor-4–mediated signal transduction. J Infect Dis 2003; 188:320–6. 26. Kullberg BJ, Vandewoude K, Herbrecht R, Jacobs F, Aoun M, Kujath P. A double-blind, randomized, placebo-controlled phase II study of filgrastim (recombinant granulocyte colony-stimulating factor) in combination with fluconazole for treatment of invasive candidiasis and candidemia in nonneutropenic patients [abstract J-100]. In: Program and abstracts of the 38th Interscience Conference on Antimicrobial Agents and Chemotherapy (San Diego). Washington, DC: American Society for Microbiology, 1998: 479. 27. Pappas PG, Bustamante B, Ticona E, et al. Recombinant interferon-g 1b as adjunctive therapy for AIDS-related acute cryptococcal meningitis. J Infect Dis 2004; 189:2185–91. 28. Rex JH, Walsh TJ, Nettleman M, et al. Need for alternative trial designs and evaluation strategies for therapeutic studies of invasive mycoses. Clin Infect Dis 2001; 33:95–106. 29. Chou TC, Talalay P. Quantitative analysis of dose-effect relationships: the combined effects of multiple drugs or enzyme inhibitors. Adv Enzyme Regul 1984; 22:27–55. Antifungal Immunotherapy • CID 2004:39 (Suppl 4) • S223