Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
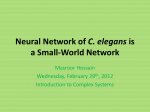
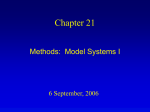
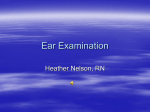
70 Journal of The Association of Physicians of India ■ Vol. 64 ■ February 2016 Skull Base Osteomyelitis Caused by an Elegant Fungus Sharafine Stephen1, Beula Subashini2, Regi Thomas3, Ajay Philip4, Rajan Sundaresan5 Abstract Malignant otitIs externa (skull base osteomyelitis) is predominantly caused by bacteria while fungal etiology is rare. We report a middle aged diabetic gentleman who succumbed to invasive skull base infection due to Apophysomyces elegans a fungus belonging to Zygomycetes which causes only skin and soft tissue infections. Mortality and invasive infections due to this genus is rarely reported, especially in the ear. Introduction S kull osteomyelitis (SBOM) secondary to fungal infection is a rare entity, SBOM caused by Mucrales- Apophysomyces elegans is even more rarer. 1 This is a case report of invasive skull base infection caused by Apophysomyces elegans belonging to the Saksenaeaceae family, under the order Mucorales. Case Report A 50 years old gentleman from south India, known diabetic for 1 year, noncompliant with medications presented with history of left ear pain of 1 week duration. The pain was sudden in onset and excruciating. He was evaluated for the same by a general practitioner who examined and cleaned his ear following which he developed mucoid discharge which persisted and became mucopurulent. Later he developed weakness on the right side of his face, inability to close his eye and a deviated angle of mouth which prompted him to take further medical attention in our hospital. On examination, he had left lower motor neuron facial nerve palsy (House Brackmann, Grade 5). Examination of his left ear revealed a tender tragus with copious amount of otomycotic debris in the left external auditory canal with florid pus and granulations involving the cartilaginous and bony external auditory canal. Pus from external auditory canal was sent for smear and culture. Examination of other systems, nose and oral cavity were normal. High Resolution contrast CT of temporal bone revealed soft tissue density within the middle ear with subtle erosion of the tegmen plate and dehiscent facial canal (Figure 1). A working diagnosis of left fungal otitis externa with skull base osteomyelitis was considered and modified radical mastoidectomy was performed, intraoperatively the middle ear revealed extensive necrotic granulations involving the canal and the mastoid (Figure 2). Canal wall down mastoidectomy (Figure 3) with debridement of the necrotic regions was performed and granulations were sent for routine and fungal cultures besides histopathology. Pus from the ear and necrotic tissue on direct microscopy showed broad aseptate fungal hyphae. Culture from both the sources grew A p o p h y s o m y c e s e l e g a n s w h i c h wa s identified based on characteristic distinctive microscopic morphology of filamentous, broad, aseptate fungal hyphae with sporangiophores hyperpigmented and thickened below the apophysis and funnel-shaped enlargement of sporangiophore below the columella, a characteristic feature of Apophysomyces elegans.2 Histopathology showed acute inflammatory exudate and granulation tissue. Patient was started on Liposomal Amphotericin-B and anticoagulants (Enoxaparin sodium) along with broad spectrum antibiotics. Three days later patient developed a swelling around the ear which on MRI revealed thrombosis of his left transverse-sigmoidojugular complex (Figure 4). He deteriorated with involvement of the contralateral side, left pontine infarct with sepsis and succumbed to the infection. Discussion in northern India. 3 It is distributed in tropical and subtropical climates, with cases reported across from va r i o u s p a r t s o f I n d i a . 4 T h e m o s t common infections of Apophysomyces elegans infections include cutaneous and subcutaneous involvement. In comparison with infections caused by other mucormycetes the frequency of Apophysomyces elegans infection in patients with underlying disorders of uncontrolled diabetes mellitus like in our case is low and is underreported. 5 Though percutaneous inoculation of the pathogen following trauma is the most common mode of Apophysomyces elegans infection, contamination of burn wounds, inoculation by insect stings or spider bite, intramuscular or subcutaneous injections are also described. 6 Currently our patient, uncontrolled diabetic had history of self-cleaning. The suction cleaning and syringing could have probably traumatized the ear canal and served a portal of entry for the organism. The angioinvasive nature of the fungus and the rapid d e t e r i o r a t i o n o f t h e p a t i e n t we r e evident from the MRI findings. Surgical intervention, antifungal therapy, and correction of the underlying risk factors are management modalities to treat Apophysomyces elegans, for strains with resistant profile which could have been a possibility as in our case, posaconazole would have served as a better option. A search on PubMed with the words “temporal bone apophysomyces, case reports” did not reveal any previous case reports. In conclusion high clinical suspicion o f i n va s i ve f u n g a l d i s e a s e d u e t o apophysomyces elegans should be borne in mind as a differential in patients suspected to have malignant otitis externa and in unresolving otomycosis of the temporal bone. Apophysomyces elegans has been isolated in 1979 from soil samples 1 PG Registrar, 3Associate Professor, 4Assistant Professor, 5Assistant Professor, Dept. of ENT, 2Assistant Professor, Dept. of Microbiology, Christian Medical College and Hospital, Vellore, Tamil Nadu Received: 10.03.2014; Revised: 18.11.2014; Accepted: 19.11.2014 Journal of The Association of Physicians of India ■ Vol. 64 ■ February 2016 Fig. 1: CT –Temporal bone (coronal and axial cuts) depicting soft tissue density in the middle ear with erosion of the tegmen plate 71 Fig. 4: MRI (T2 weighted coronal) scan revealing thrombosis of left transverse sigmoidojugular complex References Fig. 2: Granulations involving the canal and the mastoid Fig. 3: Post-operative canal wall down mastoidectomy cavity 1. Blyth CC, Gomes L, Sorrell TC, da Cruz M, Sud A, Chen SCA. Skull-base osteomyelitis: fungal vs. bacterial infection. Clin Microbiol Infect 2011; 17:306–311. 2. Brandt, Rinaldi MG, Nolte FS, Langston A, Ferguson SMTD, Schniederjan SD, Dionne-Odom JME. Posaconazole treatment for Apophysomyces elegans rhino-orbital zygomycosis following trauma for a male with wellcontrolled diabetes. J Clin Microbiol Reviews 2007; 45:1648. 3. Misra PC, Srivastva KJ, Lata K. Apophysomyces, a new genus of the Mucorales. Mycotaxon 1979; 8:377–382. 4. Chakrabarti A, et al. Apophysomyces elegans: an emerging zygomycete in India. J Clin Microbiol 2003; 41:783–788. 5. G oya l A , Tya gi I , Sya l R , M a ra k R S , S i n g h J. Apophysomyceselegans causing acute otogenic cervicofacial zygomycosis involving salivaryglands. Med Mycol 2007; 45:457–461. 6. Chander JK, Attri A, Mohan H. Primary cutaneous zygomycosis from a tertiary care centre in north-west India. Indian J Med Res 2010; 131:765–770.