Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
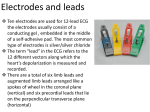
Cardio 6 – Understanding the ECG Anil Chopra 1. Describe how the recordings of the six standard limb leads are obtained from four electrodes attached to the limbs. 4 leads connected, 1 to each limb. Right Foot is used as 0 reference point always. (Connected to 0 volts reference). Right arm, left arm, and left foot are assumed to be part of an equilateral triangle. The heart is in the middle. (Einthoven’s Triangle). These first 3 leads are the STANDARD LIMB LEADS. They are connected with the following as electrodes: Lead 1: Left arm Right arm. Left arm is positive electrode. Lead 2: Left foot right arm Left foot is positive electrode. Lead 3: Left foot left arm Left arm is positive electrode. Another 3 limb leads can be connected up which use one single limb lead as one electrode (the positive (+) one) and another 2 leads connected together to make up the negative (-) electrode. AUGMENTED LIMB LEADS They are connected with the following as electrodes:Augmented Vector Right – Right arm Left Arm & Left Foot Right arm is positive electrode Augmented Vector Left – Left Arm Right Arm & Left Foot Left arm is positive electrode Augmented Vector Foot – Left Foot Right Arm & Left arm Left foot is positive electrode Together they make Hexagonal reference system This provides more angles from which the electrical activity from the heart. 2. Explain briefly the principal underlying the concept of Einthoven’s triangle. The concept simply assumes that the 3 standard limb leads are equidistant and the heart lies in the centre of an equilateral triangle. They can be placed on the shoulders and pubic symphysis, but usually the leads are placed on the wrists and ankles, it does not matter. Another feature is that they all lie in the same (frontal) plane. 3. Appreciate why the magnitude and direction of components of the ECG from lead to lead. When depolarisation moves toward + ve Upward deflection Away from + v Downward deflection Perpendicular to +ve No deflection or biphasic left muscle different AXIS lead will direction deflection. Ion an ECG the movement of charge in the form of depolarisation and repolarisation is measured. Generally the direction of depolarisation is forward the ventricle as it has the largest in its wall. The diagrams shows MEAN FRONTAL PLANE and how much deflection each show. The more parallel the of depolarisation to the electrode, the larger the 4. Know the normal physiological range of the mean frontal plane axis. Generally the mean frontal plane axis is between, -30 and +90 because of the large muscle mass of the left ventricle. It does however depend on : (1) The way the heart lies (2) The amount of muscle in the left ventricle. 5. What is meant by the terms right and left axis deflection and how these conditions may occur. If the mean frontal plane axis lies beyond -30° then it is called LEFT AXIS DEVIATION. This occurs in left ventricular hypertrophy. Significant deflection is –ve in lead II. If the mean frontal plane axis lies beyond +90° then it is RIGHT AXIS DEVIATION. Occurs in right ventricle hypertrophy. Significant deflection is –ve in lead I and +ve in lead III Associated with pulmonary conditions. 6. Describe how the recordings of the six pre-cordial chest leads are obtained. Whereas the limb leads measure depolarisation in the frontal plane, the 6 CHEST LEADS measure depolarisation in the horizontal plane. They are labelled V1 – V6 respectively. Their positions are shown here: all are positive electrodes. V1:Right 4th Intercostal space – parasternal (right ventricle) V2:Left 4th Intercostal space – parasternal (right ventricle) V3:Left between V2 and V4 (septum & anterior wall of left ventricle) V4:Left 5th intercostal space, mid clavicular line (septum and anterior LV) V5:Left anterior axillart line, in line with V4 (anterior & lateral LV) V6:Left mid-axillary line (anterior & lateral LV) 7. State how the information obtained from the chest leads differs from that derived from limb leads. Limb leads are in frontal plane. Chest leads are in horizontal plane. 8. Explain why the magnitude and direction of the components vary as the recording electrode and moves away from V1 – V6. The diagram on the previous page shows how the first part of the heart to depolarise is the septum, then the general direction of depolarisation is the left ventricle. Therefore V1 will have a small upward deflection followed by a large downward one as the small septal depolarisation is toward the electrode and the large left ventricle depolarisation is away from the electrode. V6 will have a small downward deflection followed by a large upward one as the small septal depolarisation is away from the electrode and the large left ventricle depolarisation is toward the electrode. From V2 to V5 the degrees will gradually change. SELF STUDY 1. Describe how depolarisation of cardiac muscle creates a field. - Action potentials move by a constantly moving reversal of membrane potential. This depolarisation of the membrane creates a front which is a boundary between the membrane portion that is depolarising and that which is resting. The excitable cells are arranged in such a way that their charges in electrical potential occur in an orderly manner. When a portion of heart muscle is polarised, the adjacent part is depolarised so a current is generated going through the heart muscle. 2. Describe how the body, acting as a volume conductor makes it possible to detect the electrical field which distant electrodes. The heart is surrounded by fluid containing salts which can therefore conduct electricity. The body therefore acts as a volume conductor. As the impulse travels along the cardiac muscle, it not only depolarises, it reverses polarity. This creates an active zone (where the inside of the cell is +ve and the outside is –ve). This change in electrical potential also occurs in the fluid surrounding the muscle, therefore allowing the changes in current to be picked up. Tissues are very good conductors of electricity, so any small currents that are created can spread through the body. The small changing electrical fields are amplified in the ECG monitor.