Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
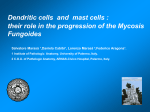
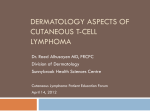
RUNNING HEAD: Mycosis Fungoides MYCOSIS FUNGOIDES Cutaneous T-Cell Lymphoma (CTCL) SAMANTHA CROWELL GRAND VALLEY STATE UNIVERSITY 0 Mycosis Fungoides 1 Presenting Signs & Symptoms of Patient Chief Complaint This patient is a white 52 year old female with the diagnosis of Mycosis fungoides, cutaneous T-cell lymphoma with a symptomatic lesion on her forehead and neck. She had noticed in the spring of 2015 that her skin nodules had increased in size and she developed new lesions on her forehead and left eyebrow. She then had a PCP performed biopsy that showed inflammation. After having a biopsy on the in early October of 2015, her pathology was consistent with atypical dermal and folliculotropic CTCL with TCR gene arrangement. On a repeat biopsy 6 days later, it documented to show mycosis fungoides with negative TCR gene arrangement, stage IVB. She had multiple erythematous tumors measuring approximately 1-3 cm located across her right forehead for combined length of 10 cm. The lateral left eyelid was erythematous and enlarged. On her left supraclavicular fossa, there were 2 raised lesions less than 1 cm wide. Multiple lesions were present on her back and trunk including a 4 cm plaque on her mid-back. Erythematous patches were present on both forearms and legs. She had already started UV therapy and had seen improvement on most of her lesions. She presented to radiation oncology to discuss having radiation treatment. Medical History The patient has a history with previous cancer. She was previously treated for a diagnosis of T1cpN0, grade 3, invasive ductal carcinoma of the left breast in 2009. She underwent a lumpectomy and sentinel node biopsy. Her tumor was ER, PR and HER-2/neu negative. She was treated with 5040 cGy to the left breast, followed by a boost to the tumor bed for a total dose of 6040 cGy. She also had chemotherapy during this time. These treatments were completed by December of 2009. She has had UV therapy for her current condition, but was seeking additional Mycosis Fungoides 2 treatment. This patient also has a long history with eczema which has been treated with Clobetasol cream. She began menstruating at the age of 13. This patient has had 1 pregnancy along with 1 birth. Family History Mother has experienced head and neck cancer. Sister has experienced cervical cancer. Maternal grandmother is deceased having experienced uterine cancer. Maternal grandfather is deceased having experienced bone cancer. Social History Patient is currently an every day smoker. She smokes a half pack per day and has done so for 30 years (15.0 pack years). Patient does not have a history of drinking. Epidemiology Cutaneous lymphomas signify about 3.9% of all non-Hodgkin lymphomas. Mycosis fungoides accounts for most of these incidences. The occurrence of cutaneous T-cell lymphoma in the United States has gone up since 1973, going from a yearly incidence rate of 6.4 events per million to 9.6 events per million people. Mycosis fungoides usually occurs in older people having a median age at time of diagnosis of 55-60 years. Although, the disease can be found in some young aged people as well. The incidence is also skewed between sexes with a male to female ratio of 2:1. About 70% of patients with mycosis fungoides in the US are white in race. Patients who are Black, Hispanic, and Asian in race account for approximately 14%, 9%, and 7% of the mycosis fungoides cases in the US. T-cell lymphoma in adults is common in areas with a high occurrence of HTLV-1 infection. These areas include southwest Japan, the Caribbean islands, South America, and parts of central Africa. Having mycosis fungoides significantly increases a patient’s risk of developing a second lymphoma, especially risks of the cutaneous T- Mycosis Fungoides 3 cell lymphoma subtype lymphomatoid papulosis and nonhematologic malignancies. The most common locations for mycosis fungoides to develop are the upper thighs and groin, breasts, armpits, and the crook of the elbow. (Jewad, S., et al., 2014 & Medscape, 2016) Etiology The primary sources for cutaneous T-cell lymphoma mycosis fungoides have not been discovered yet. However, there is evidence that mycosis fungoides could be in relation to a chronic inflammatory skin disease which is directed by T-cells. (Medscape, 2016) In addition, mycosis fungoides has been thought to stem from a chronic antigenic stimulation. This condition leads to an uncontrolled clonal development which creates a buildup of lymphatic T-cells within the skin. Researchers have found that in early mycosis fungoides tumors there an increased numbers of dendritic cells present. There is also evidence supporting the idea that neoplastic Tcells can release APC ligands. This would propose the idea of T-cell buildups being caused by some sort of self-stimulation. If a patient has HIV or has had a type of immunosuppression done to their system prior to an organ transplant this could increase their risk of developing a cutaneous T-cell lymphoma. Other occupational exposures have been researched, however, there is not enough evidence to support their involvement with mycosis fungoides either way. (Jawed, S., et al., 2014) Comparison of Patient to the Typical This patient seems to be somewhat typical for this disease. This patient is white in race which is very typical for this disease. She is a middle aged which is most common, however, she is a female and this disease is less common in females than it is in males. The patient also was diagnosed with the disease when it was already in a late stage. This is atypical because around Mycosis Fungoides 4 70% of patients at the time of diagnosis are still in the early stage of disease. (Jawed, S., et al., 2014) Patient Work-Up Information Date Procedure Results Spring of 2015 Chief Complaint Patient noted that her skin nodules had increased in size. She also noticed new lesions on forehead and left eyebrow. October 6, 2015 Biopsy at Dermatologist Pathology was consistent with atypical dermal and folliculotropic CTCL with TCR gene arrangement. October 12, 2015 Repeat Biopsy Pathology showed mycosis fungoides with negative TCR gene arrangement. November 2015 Dermatologist in Another Clinic Patient was seen by an experienced dermatologist and discussed at tumor board. December 2015 Radiation Oncologist in Another Clinic Physician recommended treatment to lesions of her forehead, left eyelid, and left supraclavicular regions. December 2015 Patient Began UV Therapy for Her Lesions Patient noticed improvement in most of her lesions. December 2015 Patient Examined by New Radiation Oncologist Discussed additional treatment options and decided on a course of palliative radiation therapy. January 19, 2016 Simulation for Radiation Therapy N/A Anatomy Discussion The lymphatic system is made up of a clear fluid called lymph, lymphoid tissue, and lymph vessels. The lymphoid tissue is composed from multiple different immune system cells that help the entire body fight off infections together. The majority of these cells are a type of white blood cell called lymphocytes. Lymphocytes are housed within the lymph nodes and other Mycosis Fungoides 5 lymphoid tissues such as the spleen, skin, bone marrow, thymus, adenoids, tonsils, digestive tract and other organs. There are two main types of lymphocytes called B-cells and T-cells, as shown in Figure 1. The B-cells make proteins called antibodies which help to protect the body against bacteria and viruses by attaching themselves and marking them for destruction. T-cells also protect the body against germs, but also can release material called cytokines which draw in other white blood cells to digest the diseased cells. The T-cells can also slow down or speed up the actions of other immune system cells. Lymphoma is a neoplasm that starts in the body’s immune system from these lymphocytes. There are two main types of lymphomas which are Hodgkin’s lymphoma and nonHodgkin’s lymphoma. If a lymphoma originates on the skin, it is a skin lymphoma. Skin lymphomas are a non-Hodgkin’s lymphoma. Lymphoma cells can develop from both B-cells and T-cells, however, they are more commonly arisen from T-cells when referencing to the skin. (American Cancer Society) Mycosis fungoides is a neoplasia of a malignant lymphatic T-cell. (Boulos, S., et al., 2014) This type of neoplasia has been categorized as a cutaneous T-cell lymphoma because of their initial presentation as skin involvement. In Figure 2, it is shown how mycosis fungoides originate from lymphatic T-cells and can make their involvement within the skin. (National Cancer Institute) Regional Lymphatic Drainage The involvement of the lymph system is huge with cutaneous T-cell lymphoma because the patient’s cancer originated from lymph cells. This patient has lesions on her forehead, eyelid, supraclavicular fossa, back, trunk, her forearms and legs. This means that the cancer has already spread throughout her entire lymphatic system. Figure 3 presents the lymphatic system is huge and covers the entire body. Mycosis Fungoides 6 Anatomy & Lymphatic Graphics FIGURE 1. Mycosis Fungoides and the Sézary Syndrome Treatment. (n.d.). National Cancer Institute. Retrieved February 15, 2016, from http://www.cancer.gov/types/lymphoma/patient/mycosis-fungoides-treatment-pdq Mycosis Fungoides 7 FIGURE 2. Compton, C. (2012). Primary Cutaneous Lymphomas. In AJCC Cancer Staging Atlas: A Companion to the Seventh Editions of the AJCC Cancer Staging Manual and Handbook (2nd ed., pp. 619-626). New York, NY: Springer. Retrieved February 18, 2016, from GVSU Online Library. Mycosis Fungoides 8 FIGURE 3. Hilmers Studios, Medical Illustrations. (n.d.). Retrieved February 20, 2016, from http://www.hilmersstudios.com/medical#anchor_lymphatic-system_ Pathology The histologic diagnosis of mycosis fungoides is not easy to figure out when in the earlier stages of development. Even pathologists with a lot of experience usually need to view several biopsies before making a diagnosis. The National Cancer Institute states “A definitive diagnosis from a skin biopsy requires the presence of MF/SS cells (convoluted lymphocytes), a band-like upper dermal infiltrate, and epidermal infiltrations with Pautrier abscesses (collections of neoplastic lymphocytes)”. All of the information needed to make a proper diagnosis may not be available in a single biopsy alone. It is important to note that even though skin cells are highly involved with this cancer, the actual skin cells themselves are not cancerous. (National Cancer Mycosis Fungoides 9 Institute) Sézary Syndrome is very similar to Mycosis fungoides and is often thought to be an advanced stage of it. It is an aggressive and cutaneous T-cell lymphoma, which is identified by “circulating atypical T cells (Sézary cells), diffuse erythema (erythroderma), and severely disabling pruritus with or without lymphadenopathy” (Jawed, S., et al., 2014). It is often thought that Sézary Syndrome is not associated with mycosis fungoides, however, sometimes it is presented after a patient had mycosis fungoides. The debate continues on whether they are related or not. (Jawed, S., et al., 2014) Staging As a standard way of classifying the degree of a patient’s cancer, the American Joint Committee on Cancer (AJCC) created the TNM staging system. This staging system can be applied to staging of Mycosis fungoides and Sézary Syndrome. TNM usually uses four key concepts which include the T which refers to the location, size, how far it has spread within the skin and nearby tissues; the N which describes how much the cancer has spread to nearby lymph nodes; the M which indicates whether the cancer has metastasized. With staging these T-cell lymphomas, the TNM system also added the category of peripheral blood involvement, B. Each of these four categories have their own staging guide. When all four of them are determined, they are combined in a process called stage grouping to assign an overall stage for the tumor. Having accurate staging is vital to allow the patient to have the correct treatment and prognosis. The following tables were created to show the staging process of Mycosis fungoides and Sézary Syndrome and all of the different components involved in it. All of the staging information in the following tables was taken from the AJCC handbook. Primary Tumor (T) TNM Categories Description Mycosis Fungoides 10 Limited patches, *papules, and/or plaques **covering less than 10% of the skin surface. T1 *For skin, patch indicates any size skin lesion without significant elevation or induration. Presence/absence of hypo- or hyperpigmentation, scale, crusting, and/or poikiloderma should be noted. **For skin, plaque indicates any size skin lesion that is elevated or indurated. Presence or absence of scale, crusting, and/or poikiloderma should be noted. Histologic features such as folliculotropism or large-cell transformation (>25% large cells), CD30+ or CD30–, and clinical features such as ulceration are important to document T1a Patch only T1b Plaque ± patch T2 Patches, papules or plaques covering 10% or more of the skin surface. T2a Patch only T2b Plaque ± patch One or more tumors ***(1≥-cm diameter) T3 T4 ***For skin, tumor indicates at least one 1-cm diameter solid or nodular lesion with evidence of depth and/or vertical growth. Note total number of lesions, total volume of lesions, largest size lesion, and region of body involved. Also note if histologic evidence of large-cell transformation has occurred. Phenotyping for CD30 is encouraged Confluence of erythema covering 80% or more of body surface area Lymph Nodes Involvement (N) TNM Categories Description Clinically abnormal peripheral lymph nodes****; no histologic confirmation NX N0 ****For node, abnormal peripheral lymph node(s) indicates any palpable peripheral node that on physical examination is firm, irregular, clustered, fixed or 1.5cm or larger in diameter. Node groups examined on physical examination include cervical, supraclavicular, epitrochlear, axillary, and inguinal. Central nodes, which are not generally amenable to pathologic assessment, are not currently considered in the nodal classification unless used to establish N3 histopathologically No clinically abnormal peripheral lymph nodes; biopsy not required Mycosis Fungoides 11 Clinically abnormal peripheral lymph nodes; histopathology N1 Dutch grade 1 or NCI LN0-2 Clone negative***** N1a *****A T-cell clone is defined by PCR or Southern blot analysis of the T-cell receptor gene. Clone positive***** N1b *****A T-cell clone is defined by PCR or Southern blot analysis of the T-cell receptor gene. Clinically abnormal peripheral lymph nodes; histopathology N2 Dutch grade 2 or NCI LN3 Clone negative***** N2a *****A T-cell clone is defined by PCR or Southern blot analysis of the T-cell receptor gene. Clone positive***** N2b *****A T-cell clone is defined by PCR or Southern blot analysis of the T-cell receptor gene. Clinically abnormal peripheral lymph nodes; histopathology N3 Dutch grades 3–4 or NCI LN4; clone positive or negative Visceral Metastasis (M) TNM Categories Description M0 No visceral organ involvement M1 Visceral involvement (must have pathology confirmation^ and organ involved should be specified) ^ For viscera, spleen and liver may be diagnosed by imaging criteria. Peripheral Blood Involvement TNM Categories B0 Description Absence of significant blood involvement: 5% or less of peripheral blood lymphocytes are atypical (Sézary) cells^^ ^^ For blood, Sézary cells are defined as lymphocytes with hyperconvoluted cerebriform nuclei. If Sézary cells are not able to be used to determine tumor burden for B2, then one of Mycosis Fungoides 12 the following modified ISCL criteria along with a positive clonal rearrangement of the TCR may be used instead: (1) expanded CD4+ or CD3+ cells with CD4/CD8 ratio of 10 or more, (2) expanded CD4+ cells with abnormal immunophenotype including loss of CD7 or CD26. Clone negative***** B0a *****A T-cell clone is defined by PCR or Southern blot analysis of the T-cell receptor gene. Clone positive***** B0b *****A T-cell clone is defined by PCR or Southern blot analysis of the T-cell receptor gene. B1 Low blood tumor burden: more than 5% of peripheral blood lymphocytes are atypical (Sézary) cells but does not meet the criteria of B2 Clone negative***** B1a *****A T-cell clone is defined by PCR or Southern blot analysis of the T-cell receptor gene. Clone positive***** B1b *****A T-cell clone is defined by PCR or Southern blot analysis of the T-cell receptor gene. B2 High blood tumor burden: 1000/ mL Sézary cells^^ or more with positive clone *****A T-cell clone is defined by PCR or Southern blot analysis of the T-cell receptor gene. Anatomic Stage/Prognostic Groups TNM Stages T N M Peripheral Blood Involvement Stage IA 1 0 0 0, 1 Stage IB 2 0 0 0, 1 Stage IIA 1, 2 1, 2 0 0, 1 Stage IIB 3 0-2 0 0, 1 Stage III 4 0-2 0 0, 1 Stage IIIA 4 0-2 0 0 Stage IIIB 4 0-2 0 1 Stage IVA1 1-4 0-2 0 2 Stage IVA2 1-4 3 0 0-2 Mycosis Fungoides 13 Stage IVB 1-4 0-3 1 0-2 Compton, C. (2012). Primary Cutaneous Lymphomas. In AJCC Cancer Staging Atlas: A Companion to the Seventh Editions of the AJCC Cancer Staging Manual and Handbook (2nd ed., pp. 619-626). New York, NY: Springer. Retrieved February 18, 2016, from GVSU Online Library. This patient has Stage IVB cutaneous T-cell lymphoma mycosis fungoides. From the tables above, it is shown that this means the patient could have any type of primary tumor presentation, lymph node involvement, or peripheral blood involvement. The specifics were not documented in her charts. However, this patient does have visceral metastasis. She has the most progressive stage of mycosis fungoides. Grading There currently is not a grading system for Mycosis fungoides. However, there is research supporting that use of a grading system would improve the diagnosis of mycosis fungoides substantially. A study published in 2001 tested a new system for interpreting and reporting biopsies suspicious for MF. The process was centered on a grading system revealing the level of diagnostic certainty from the pathologist. The researchers found that the agreement percentage on histological diagnosis of mycosis fibrosis among the pathologists improved from 48% to 76% when using the grading system. Additional research is needed in this area for future improvement. (Guitart, J. et al., 2001) Patients Pathology, Stage & Grade She then had a PCP performed biopsy that showed inflammation. After having a biopsy on the in early October of 2015, her pathology was consistent with atypical dermal and Mycosis Fungoides 14 folliculotropic CTCL with TCR gene arrangement. On a repeat biopsy 6 days later, it documented to show mycosis fungoides with negative TCR gene arrangement. Her formal diagnosis was noted as cutaneous T-cell lymphoma, mycosis fungoides, stage IVB, with positive lymph nodes in multiple sites. Grade is not assessed for this condition. Radiation Therapy Treatment Plan & Rx for Patient The patient was prescribed to 2400 cGy to the right forehead, temple, and supraclavicular neck. This was to be delivered in 12 fractions of 200 cGy each with electrons. The doctor decided not to treat the left eyelid because it had decreased and due to its location and proximity to the eye. Radiation Therapy Treatment Information & Patient Set-Up Simulation for the patient took place on January 19, 2016. She was to lie head first on the table in a supine position with an IMRT headboard and open faced IMRT mask. Under her head was a size ‘B’ headrest and her hands were to be at her sides to keep her arms out of the field. She also had a large knee sponge under her legs to keep her comfortable and in place. There were marks drawn on the mask from the doctor to create a matching electron cutout light field. For treatment she was to be clinically set-up matching the light field to the outlines on the mask. Her SSD needed to be set to 100cm on her forehead and 110cm for her supraclavicular field. This patient was prescribed to 2 different electron fields. A 1cm bolus is required for each field daily. Radiation Therapy Treatment Type & Delivery Field Name Gantry Angle Collimator Angle Couch Angle Planned SSD Forehead 303.0 35 335 100.0 cm Planned Energy MU Cone Size Bolus (cm) 198 MU 15X15 1.0 9 MeV Mycosis Fungoides Lt Sclv 60.0 15 75 75 110.0 cm 246 MU 9 MeV 15X15 1.0 Radiation Therapy Complications, Side Effects & Treatment This patient had a few complications from her radiation therapy treatments. After 10 Gy in 5 fractions, she had complained of fatigue. She denied having lack of appetite and fever. The patient also complained of dry skin. The areas to her right forehead, left clavicle, and back were red but the patient seemed to think they were improving because they were getting smaller. The physician stated that at this point her lesions were flattening out. She also complained of having migraines. When her treatment reached 18 Gy in 9 fractions, the patient had very similar complaints and complications. The only addition is the migraines have been more frequent and she complained about a pressure in her head. Once the patient completed her treatment of 24 Gy in 12 fractions, her lesions were not gone but looked more flat and smooth. She has been instructed to follow up in a month to see the progress. Adjuvant Therapies, Complications, Side Effects & Treatment Six types of standard treatment are used: Photodynamic therapy, Radiation therapy, Chemotherapy, Other drug therapy, Biologic therapy & Targeted therapy. Photodynamic therapy uses a combination of drug and a laser light that work together to kill cancer cells with little damage to the surrounding healthy tissue. The drug is specially formulated to accumulate within tumor cells and remain inactive until exposed to light. It is injected into a vein and the laser light is directed onto the affected area which activates the drug to kill the tumor cells. (Humme, D., Nast, A., Erdmann, R., Vandersee, S., & Beyer, M., 2014) Mycosis fungoides can also be treated with a type of radiation therapy called total skin electron beam radiation therapy. This treatment type uses rays of electrons on the skin surface of Mycosis Fungoides 16 the entire body. Electrons treat superficially, so, the normal underlying tissues and organs will be unaffected. Another type of radiation that can be used is ultraviolet B radiation therapy. This uses a special light that directs UVB radiation over the skin. (National Cancer Center) Chemotherapy uses drugs to prevent cancer cells from growing, either by killing them or by preventing them from dividing. When the drugs are taken orally or injected into the body through either a vein or into a muscle, the drugs are able to reach the whole body through the bloodstream. This is called a systemic treatment because it treats the entire system of a body. This is a good treatment option for cancers that have started to metastasize because the distant cancer cells won’t be missed. Chemotherapy can also be given topically through the use of a cream, lotion, or ointment on the skin. For example, topical corticosteroids can be applied to relieve painful symptoms of red, swollen, and inflamed skin. They come in many forms of application. (Panasiti, V, et al., 2006) The type of chemotherapy chosen for a patient depends on their disease type and stage that needs to be treated. (National Cancer Center) Another treatment called biologic therapy uses different substances to activate a patient’s own immune system to fight off their cancer. These substances are made either in the body or within a laboratory. The goal of them is to enhance, instruct, or repair the natural defenses of the patient’s body against their cancer. Mycosis fungoides can be treated with a substance called Interferon as a type of biologic therapy. Interferon interferes with the reproduction of neoplastic cells and can slow the already existing tumor from growing. A similar treatment called targeted therapy uses certain drugs or substances to search for and destroy specific types of cancer cells. The drugs are designed to not harm normal cells. Monoclonal antibody therapy is a specific targeted therapy used to treat mycosis fungoides. This cuts off the nutritional supply to the tumor and stops it from growing and in most cases kills the tumor. (National Cancer Society) Mycosis Fungoides 17 The treatment that is prescribed and delivered to the patient will depends on the type and stage of the cancer being treated. Treatments will vary by patient. Other Therapies & Complications the Patient Received This patient also received UV therapy for her disease. No complications or details on treatment were noted. This was performed in a different cancer research facility and cancer treatment center. Critical Structures & Dose Tolerances When treating patients with mycosis fungoides the main critical structure that needs to be focused on is the skin. This is because the lesions are involved with the skin in multiple locations in most patients. If the skin dose goes past the tolerance, then it could result in acute or chronic dermatitis. For this particular patient, her disease was on her head and neck region. This means that there are some other main critical structures that need to be watched as well. The lenses of the eyes have a really low tolerance dose and she is being treated on her face, so, these need to be monitored closely. If any parts of the eye are damaged including the retina, cornea and lens, then the injury will be blindness. We are treating a lymphoma, so knowing the tolerance dose of the lymph nodes and other lymphatics is also important. Passing these tolerance doses would result in atrophy or sclerosis. Since this patient is being treated with electrons, the treatment dose is very superficial. This means the internal organs and normal tissues are not at risk for exceeding their tolerance dose. Critical Structure TD 5/5 (cGy) Lens of eye 500 Cornea of eye 5000 Retina of eye 5500 Skin 5500 Mycosis Fungoides 18 Lymph nodes and lymphatics 5000 Washington, C., & Leaver, D. (2010). Overview of Radiobiology. In Principles and Practice of Radiation Therapy (3rd ed., pp. 81-82). St. Louis, Mo.: Mosby Elsevier. Routes of Spread The routes of spread for mycosis fungoides are through the lymphatic system and the blood. Since most people are diagnosed at an early stage, they do not make it through all of the stages. This is in part due to the fact that Mycosis fungoides progresses slowly from stage to stage. The majority of patients with mycosis fungoides first develop spots on their skin called patches. These lesions are known to be flat, scaly, pink or red in color, and can be itchy. These patches are caused by Cancerous T-cells due to them moving from the blood and through the skin. The skin cells are not actually cancerous, however, the cancerous T-cells can be found within the patches. The patches do not have a pattern when it comes to presentation. They can fade and resurface or can remain unchanged over time. If the patches on the patient get worse they change into plaques which is the next stage of mycosis fungoides. It is a generally a systematic disease, so it can spread to all parts of the body. It was found “In any stage of mycosis fungoides, the cancerous T cells can spread to other organs, including the lymph nodes, spleen, liver, and lungs, although this most commonly occurs in the tumor stage” (Mycosis Fungoides, 2016). Once the tumor spreads into visceral tissue, it is then considered Stage IVB with the worst prognosis. When the cancer cells spread into an actual tumor they have a possibility of necrotic ulceration. (Mycosis Fungoides, 2016) Prognosis & Survival For patients with mycosis fungoides the prognosis is based greatly on the presentation of the disease. When there is visceral and peripheral blood involvement and lymphadenopathy, the Mycosis Fungoides 19 likelihood of having cutaneous involvement gets worse. As this gets worse, so does the prognosis of the patient. The average survival after diagnosis differs between stages. Patients with stage IA disease have an average survival of 20 years or more. The majority of deaths for patients with this stage of disease are not in any relation to mycosis fungoides. However, over half of the patients with stages III-IV disease have death caused by mycosis fungoides. They only have less than 5 years for an average survival. Since the symptoms of mycosis fungoides often lead to a misdiagnosis of eczema or other skin irritations, the symptoms can be present for years. It has been found that the degree of cutaneous involvement, the T scale in the staging system, is considerably linked with the patient’s prognosis. As involvement increases, there is a decreased overall survival. In advanced stages of cutaneous involvement some patients have had progression-free survival. (National Cancer Institute) Patient’s Prognosis & Survival Although this patient has seen progress to her lesions, I do not think that her prognosis is good. Her cancer is at a very progressive stage for this type. The average survival for her stage IVB is 5 years or less. Also, her physician had planned her treatment to be palliative not curative. I think she has a 20% chance for a 5-year survival. Mycosis Fungoides 20 Sources Cited Articles & Websites Boulos, S., Vaid, R., Aladily, T. N., Ivan, D. S., Talpur, R., & Duvic, M. (2014). Clinical presentation, immunopathology, and treatment of juvenile-onset mycosis fungoides: A case series of 34 patients. Journal of the American Academy of Dermatology, 71(6), 1117-1126. Retrieved February 18, 2016, from ScienceDirect. Compton, C. (2012). Primary Cutaneous Lymphomas. In AJCC Cancer Staging Atlas: A Companion to the Seventh Editions of the AJCC Cancer Staging Manual and Handbook (2nd ed., pp. 619-626). New York, NY: Springer. Retrieved February 18, 2016, from GVSU Online Library. Cutaneous T-Cell Lymphoma. (2016, January 15). Medscape. Retrieved February 18, 2016, from http://emedicine.medscape.com/article/2139720-overview Guitart, J., Kennedy, J., Ronan, S., Chmiel, J. S., Hsiegh, Y., & Variakojis, D. (2001). Histologic criteria for the diagnosis of mycosis fungoides: Proposal for a grading system to standardize pathology reporting. J Cutan Pathol Journal of Cutaneous Pathology, 28(4), 174-183. Retrieved February 20, 2016, from PubMed. Humme, D., Nast, A., Erdmann, R., Vandersee, S., & Beyer, M. (2014). Systematic review of combination therapies for mycosis fungoides. Cancer Treatment Reviews, 40(8), 927933. Retrieved February 18, 2016, from ScienceDirect. Jawed, S., Myskowski, P., Horwitz, S., Moskowitz, A., & Querfeld, C. (2014). Primary cutaneous T-cell lymphoma (mycosis fungoides and Sézary syndrome) : Part I. Diagnosis: Clinical and histopathologic features and new molecular and biologic Mycosis Fungoides 21 markers. Journal of the American Academy of Dermatology, 70(2), 205.e1-205.e16. Retrieved February 19, 2016, from ScienceDirect. Jawed, S., Myskowski, P., Horwitz, S., Moskowitz, A., & Querfeld, C. (2014). Primary cutaneous T-cell lymphoma (mycosis fungoides and Sézary syndrome) : Part II. Prognosis, management, and future directions. Journal of the American Academy of Dermatology, 70(2), 223.e1-223.e17. Retrieved February 19, 2016, from ScienceDirect. Mycosis fungoides. (2016). Retrieved February 20, 2016, from http://ghr.nlm.nih.gov/condition/mycosis-fungoides Mycosis Fungoides and the Sézary Syndrome Treatment. (n.d.). National Cancer Institute. Retrieved February 15, 2016, from http://www.cancer.gov/types/lymphoma/patient/mycosis-fungoides-treatment-pdq Panasiti, V., Devirgiliis, V., Borroni, R., Rossi, M., Curzio, M., Mancini, M., . . . Calvieri, S. (2006). Management of skin ulcers in a patient with mycosis fungoides. Dermatology Online Journal, 12(2), 16. Retrieved February 21, 2016, from PubMed. Washington, C., & Leaver, D. (2010). Overview of Radiobiology. In Principles and Practice of Radiation Therapy (3rd ed., pp. 81-82). St. Louis, Mo.: Mosby Elsevier. What is lymphoma of the skin? (2014). American Cancer Society. Retrieved February 21, 2016, from http://www.cancer.org/cancer/lymphomaoftheskin/detailedguide/lymphoma-of-theskin-what-is-lymphoma-of-the-skin Images Compton, C. (2012). Primary Cutaneous Lymphomas. In AJCC Cancer Staging Atlas: A Companion to the Seventh Editions of the AJCC Cancer Staging Manual and Handbook Mycosis Fungoides (2nd ed., pp. 619-626). New York, NY: Springer. Retrieved February 18, 2016, from GVSU Online Library. Hilmers Studios, Medical Illustrations. (n.d.). Retrieved February 20, 2016, from http://www.hilmersstudios.com/medical#anchor_lymphatic-system_ Mycosis Fungoides and the Sézary Syndrome Treatment. (n.d.). National Cancer Institute. Retrieved February 15, 2016, from http://www.cancer.gov/types/lymphoma/patient/mycosis-fungoides-treatment-pdq 22