Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Fundus photography wikipedia , lookup
Blast-related ocular trauma wikipedia , lookup
Contact lens wikipedia , lookup
Cataract surgery wikipedia , lookup
Visual impairment due to intracranial pressure wikipedia , lookup
Mitochondrial optic neuropathies wikipedia , lookup
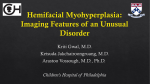
Brief Report Sanitha Sathyan, Aneeta Jabbar Corneal Involvement In A Case Of Mycosis Fungoides - Case Report A 42 year old gentleman, who was diagnosed as Mycosis fungoides in 2006, currently undergoing radiotherapy, presented to our OPD with complaints of pain, watering and defective vision in left eye of 1 month duration. He was under the care of a local ophthalmologist and was on systemic and topical acyclovir, topical antibiotics, cycloplegics and preservative free lubricants for 1 week. On examination, he had generalized hyperpigmented plaques over the body and face including the periorbital region. His visual acuity was: OD: 6/6, OS: 6/18 . OD: upper lid showed an ulcerative plaque like lesion 2 mm from the anterior lid margin with localized keratinization of the skin. Anterior segment and fundus were otherwise unremarkable. fig:3 showing partly epithelialised lesion in OS Fundus examination in both eyes were within normal limits. Our diagnosis was OD: Infiltration of upper lid secondary to Mycosis fungoides, OS : Herpes Simplex Virus epitheliopathy Corneal infiltration secondary to Mycosis fungoides was also considered as a differential diagnosis. He was continued on Acyclovir eye ointment for 2 weeks , Prednisolone acetate 1% eye drops QID and preservative free lubricant eye drops. Since his was a biopsy proven case of Mycosis fungoides, futher biopsy from the lid lesion was deferred. fig: 1 showing the lid lesion in OD OS: There was a linear epithelial defect in the inferior paracentral cornea simulating a dendrite. Stroma surrounding the epithelial lesion was edematous, with cellular reaction and Descemet’s level folds. There was stromal scarring nasally with punctate keratitis There was no vasularization. At one week review, the corneal lesion was resolving with mid stromal scar and mild punctate keratitis. Acyclovir eye ointment was stopped after 3 weeks and topical steroids tapered. At one month follow up, the lesion healed completely with mid stromal scaring. Discussion Mycosis fungoides is a malignant cutanoeus T- cell lymphoma characterized by clonal expansion of T helper cells and rarely T-suppressor or natural killer cells, that usually present as a widespread chronic cutaneous eruption, which progresses to form plaques and tumours. Eventually non-cutaneous involvement supervenes with infiltration of lymph nodes and visceral organs[1]. fig:2 showing the linear lesion, partly scarred in OS Ocular involvement may occur in up to a third of advanced cases of Mycosis fungoides and most frequently presents as tumours or infiltration of the eyelids [2] Less frequent manifestations include involvement of the caruncle[3] the cornea[2] the sclera[4] the optic disc[5] and optic nerve[6] 70 Address for Correspondance: Cataract and Cornea Services, Little Flower Hospital and Research Centre, Angamaly Sanitha Sathyan et al - Case Report - Mycosis Fungoides and the orbit[7].Intraocular involvement has been reported only rarely[5,8]. pointed more towards a self resolving variant of corneal Corneal involvement is a rare occurrence in Mycosis fungoides. This was first reported by Besnier and Hallopeau in (1892) and histologically confirmed by Herman in 1951. Occasionally this may be the first evidence of the disease, but usually it is seen in well developed cases and occasionally as a terminal event. clinical suspicion is needed in the diagnosis of the unusual Corneal manifestations vary. They may appear as a regular linear infiltrate, somewhat resembling a dendrite, which progresses to an ulcerative keratitis involving the stroma and Descemets membrane.Alternatively progressive and usually heavily vascularised stromal infiltrates appear which may suffer acute exacerbations and may breakdown to ulceration or undergo spontaneous resolution. Pathological examinations have demonstrated the typical infiltration characterized by large mononuclear cells of the primitive lymphoblastic type. This case was reported because of the rare corneal presentation of Mycosis fungoides. Antivirals were used in the treatment keeping in view of the more common herpetic keratitis. But the lesion lacked the typical dendritic borders and terminal bulbs. Reference to the older literature involvement in Mycosis fungoides. Therefore a high index of presentation of this rare disease. References 1. Lever WF, Schaumberg-Lever G. Histopathology of skin. Philadelphia: Lippincott, 1990: 819-27. 2. Stenson S, Ramsay DL. Ocular findings in mycosis fungoides. Arch Ophthalmol 1981; 99: 272-7. 3. Fradkin AH, Ruiz RS, Sloane JA. Mycosis fungoides involving the caruncle. AmJ Ophthalmol 1969; 68: 719-22. 4. Wolter JR, Leenhouts TM, Hendrix RC. Corneal involvement in mycosis fungoides. AmJ Ophthalmol 3; 55: 317-22. 5. Keltner JL, Fritsch E, Cykiert RC, Albert DM. Mycosis fungoides: intraocular and central nervous system involvement. Arch Ophthalmol 1977; 95: 645-60. 6. Pariser DM. Mycosis fungoides involving the brain and optic nerves. Arch Dermatol 1978; 114: 397-9. 7. Zucker JL, Doyle MF. Mycosis fungoides metastatic to the orbit. Arch Ophthalmol 1991; 109: 688-91. 8. Forster HC. Mycosis fungoides with intraocular involvement. TransAmAcad Ophthalmol Otolaryngol 1960; 64: 308-13. Dr Sanitha Sathyan has finished her DNB at Little Flower Eye Hospital, Angamaly 71