Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Effects of long-term benzodiazepine use wikipedia , lookup
Orphan drug wikipedia , lookup
Drug design wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Drug discovery wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Pharmacognosy wikipedia , lookup
Prescription costs wikipedia , lookup
Prescription drug prices in the United States wikipedia , lookup
Neuropharmacology wikipedia , lookup
Drug interaction wikipedia , lookup
Polysubstance dependence wikipedia , lookup
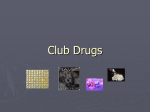
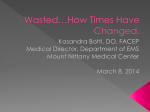
Detox regimens for party drugs Faculty of Addictions Psychiatry essay prize Chloe Taylor UCL Medical School 12/13/2013 0 Party drugs are primarily used in a recreational manner and are a group of substances defined by the context in which they are taken rather than their pharmacological properties. Their use is increasing, both across the UK and worldwide, and there is little research in the literature on how this should be tackled. Some may argue that because recreational use ultimately implies a lack of addiction, we should focus our attention elsewhere. Further, given that most definitions of a drug detox assume a degree of addiction, it is perhaps counter-intuitive to even consider the use of a drug detox regime in the case of party drugs. However, it is clear that these drugs are associated not only with the general risks of intoxication and tolerance, but also with well-defined substance specific harms and in some cases withdrawal syndromes (Winstock & Mitcheson, 2012). This essay will analyse the effectiveness of a current party drug detox regimen and consider other ways of managing the abuse of party drugs in the UK. There is no clear definition of ‘party drugs’ but generally the term describes substances abused for recreational purposes in a social context. They include a vast array of substances from well-established drugs on the club drugs scene, like ecstasy, to novel psychoactive substances (or ‘legal highs’). Over the past decade the number of these drugs has dramatically increased with a current rate of one newly reported substance across Europe each week(EMCDDA, 2013). A simple definition of drug detox could be: a process by which the body is rid of the toxins that have accumulated through drug use or abuse. The term ‘detox’ however has come to mean a variety of things and clarity around the definition is crucial for those involved in the process in order for realistic expectations to be set and achieved. Inherently the concept of withdrawal is closely linked as it can be thought of as the psychological and mental readjustments that occur with the discontinuation of an addictive substance. The NICE guidelines on opioid detox nicely unite the two concepts in their definition: “Detoxification is the process by which an individual is withdrawn from the effects of a psychoactive substance….Typically, the individual is clinically intoxicated or already in withdrawal at the outset of detoxification. Detoxification may involve the administration of medication, the dose of which is calculated to relieve withdrawal symptoms without inducing intoxication, and is gradually tapered off as the individual recovers.”(NICE, 2008) The concept of detox regimens is not a new one; there are already well established regimens for opiate abuse using methadone and buprenorphine in the UK. Likewise the concept of pharmacological agents being used to help treat substance abuse is both common and logical given that addiction is in part due to the physical effects of withdrawal. The idea of acting upon the same receptors modulated by agents of abuse can lead to either a reversal of effects (e.g. naloxone and opiates) or form the basis of substitute therapy (e.g. methadone and opiates). If this is not possible, either because the receptors affected by the substance of abuse are not known or too many are implicated, then drugs can be used to treat the symptoms of withdrawal individually. Instances of this include the use of hyoscine butylbromide (Buscopan®) for gastro-intestinal muscle spam in opioid withdrawal. In defining detox in this manner it leads to the logical conclusion that a degree of addiction must be present and that, dependent on the substance abused and amount consumed, 1 there may be a risk of withdrawal. This is important to establish as many users of party drugs view their use as recreational; a term that is used to suggest occasional use (for instance on weekends) and one that ultimately implies a lack of addiction.There is a perception amongst some healthcare professionals and drug users that party drugs are not addictive or are safer in some way than ‘classic’ drugs of abuse such as cocaine or heroin(Winstock & Mitcheson, 2012). In part this view is held and reinforced by the lack of knowledge on such substances and the dearth of academic literature on their management. However it is clear that these drugs are associated not only with the general risks of intoxication but also with well-defined substance specific harms and in some cases withdrawal syndromes(Winstock & Mitcheson, 2012). The recreational drug market has been inundated with numerous new substances over the past few years, many of which have been specifically designed and marketed to comply with legal regulations (the ‘legal highs’). These new substances provide a challenge for healthcare professionals as they have been studied much less than other well established substances of abuse such as heroin and cocaine(Winstock & Mitcheson, 2012). To explore the range of party drugs currently used in the UK would be beyond the scope of this essay but broadly they fall into categories similar to those of common illicit substances (see Table 1). One of the major groups of new party drugs are those derived from cathinone, a naturally occurring psychoactive substance, which includes mephedrone. The popularity of which has tailed off over the past few years with 1.6% of 16-24 year olds reporting having used it within 2012-13 compared to 4.4% in 2010-11(Home Office, 2013). Group Stimulants Tranquilisers Dissociatives Positive Effects euphoria increased energy increased libido empathy pro-social effects disinhibition increased libido relaxation euphoria stimulation sensory dissociation hallucinations Negative Effects tachyarrhythmias disorientation anxiety dehydration agitation, bradycardia, hypotension, seizures Examples mephedrone methylone palpitations disorientation psychosis urinary symptoms ketamine nitrous oxide GHB GBL 1,4-butanediol Table 1: Major groups of common party drugs and their effects (GHB = gamma-hydroxybutyrate, GBL = gamma-butyl-lactone) Within this group there is one drug for which a relatively new detox regimen is used clinically albeit on the background of limited evidence; gamma-hydroxybutyrate (GHB). The way in which GHB can cause addiction and precipitate a severe withdrawal syndrome is well illustrated in a clinical case I came across when on placement at a drug advisory service in London. It involves Darren, a 28 year old Romanian man, who has presented several times to the service, each time with an increasingly dependent GHB/GBL habit,and who has recently undergone a GHB detox. 2 Case Example Darren’s story begins in Romania where he experienced a difficult upbringing, both suffering and witnessing emotional and physical abuse from his mother and step-father. His stepfather would beat up his mother and cause damage to the house on a regular basis although he denies ever suffering physically.Darren was vaguely aware of his biological father but only knew him as a local man, until his funeral, when Darren was 7, at which his mother revealed his true identity. It transpired his mother had left his biological father when he was 1 as he was a violent alcoholic. Darren has a brother whom his is close to and also had an older sister who died in a car accident when he was 8 years old (she was 26 at the time). Following this incident, Darren states that his mother ‘went really downhill’ and describes what sounds like an episode of depression. At this time his step-father left and the family found themselves in financial difficulty through a combination of this and the debts of his biological father. He has never had a significant intimate relationship and states that he is scared to love someone, finding long term relationships hard to maintain. Nonetheless he has a good relationship with his brother who, along with his sister in law, provides a strong family support network and gives him motivation to become abstinent. Despite this many of Darren’s friends are users, although he has recently moved house and changed his mobile number in a bid to leave some of his drug using networks behind. He used to work as a hairdresser but since he has been using GBL daily has found that the impact on his mental and physical health has made it difficult to hold down employment. Darren started using drugs at 15 by smoking cannabis although he denies his use ever became problematic. A year later he moved to London and started using more and varying types of drugs and on a regular basis. He would go out most weekends and take combinations of ecstasy, amphetamine, ketamine, MDMA and mephedrone. Whilst this use was regular he claims it was not a problem and only confined to weekends. However by the time he was 17 he had started taking cocaine and would buy 3 grams to last during the week, a marked departure from his previous patterns of substance abuse. The first time he took GBL he was 17 and ended up accidentally overdosing and requiring hospitalisation after he suffered a cardiac arrest. This incident seemed to frighten him and he moved away from London back to Romania where he remained drug abstinent for 3 years, although he was drinking heavily during this time (60 units per week). When he returned to the UK at 21 his GBL use resumed and although it was limited to the weekend he started to combine it with crystal meth and crack. The use of these combination drugs was not sustained as he found them unpleasant but the GBL use continued to escalate.Aged 25 he was using 15mls every other day althoughDarren states his drug use only became problematic at the start of 2011 at which time he was using 30mls per day of GBL. He has injected several times in the past but no longer does although he has had an acute hepatitis B infection and currently has hepatitis C, while his HIV status is negative. His drug use is currently funded by money he borrows from his brother who helps to manage his finances and pays his rent. He lives alone and struggles to keep up with basic household tasks such as cleaning and cooking; in fact he often eats very little and is currently underweight.In terms of his physical health he has blood borne viruses as 3 mentioned and a history of cardiac arrest (due to GBL overdose) and a head injury at 10 (due to a car accident) although he reports no long term problems from either of these. His only criminal history is that he received a suspended sentence, aged 18, when a friend committed theft and he was charged as an accomplice.While Darren has no formal diagnosis of a mental health disorder he has occasionally exhibited behaviour which sounds psychotic in nature e.g. running outside naked and talking nonsense. There may also be underlying issues that he is struggling to deal with regarding the grief effects of losing his father and sister. His first presentation to the service was in June 2011, as an emergency following several days of withdrawal after he had suddenly stopped using GHB. He was brought in by his sister in law who was generally concerned about his drug use but felt compelled to access health services after his withdrawal symptoms had progressed and did not appear to be resolving. His withdrawal included both mental symptoms such as agitation, disorientation and forgetfulness as well as physical symptoms of diarrhoea, twitching in his hands and feet, lower back pain and tiredness. This episode was self-limiting; he was duly assessed in hospital and following normal bloods and ECG was discharged the same day. This episode is important as prior to his current treatment it represents the longest period of time for which he has been GHB abstinent (2 days).Following this episode Darren struggled to attend appointments and when he did he seemed reluctant to engage with services. Treatment consisted of 1:1 psychology sessions and some group work but Darren was still regularly using and dropped out by the end of the year. Despite admitting his drug use was problematic, as he was unable to work, he had little motivation to address this. The second time Darren accessed services was in October 2012 when he was taking 30mls of GHB daily, 20mls in the day and another 10mls at night whilst also taking mephedrone recreationally. He said he felt that his GHB use was the primary problem and that he was unable to stop for more than 2 days at a time or else he would experience withdrawal symptoms (described similarly to his 2011 episode). Crucially for the first time, in by now his 7 years of continual GHB use, he was primarily experiencing negative effects whenever he used. The major symptoms included heart palpitations, agitation, sweats and nervousness. He had also developed such a level of tolerance that he was using every 2 hours, and this was having devastating effects on his sleep patterns as he would spend most of the night walking in between doses. His desire for treatment was considerably greater on this presentation and he underwent a mixture of psychosocial interventions and medically assisted GBL detox. The detox was provided as high dose benzodiazepine therapy monitored in the community while the psychosocial work consisted of mainly relapse prevention and motivational interviewing. He was discharged in March 2013 on co-dydramol and zopiclone in order to help treat symptoms of withdrawal after becoming abstinent. Unfortunately as with many GHB users this abstinence was short lived and only a month later he referred himself back to drug services. At this presentation he was back using at pre-treatment levels of GHB and also mephedrone recreationally. Despite prescribed sleeping tablets he was still struggling with a lack of sleep and had relapsed as a result of this.It was decided more focus should be put on pre and post detox care and specialist GHB services should be involved. He was again given high dose benzodiazepines at 100mg per day that were tapered down to nil over 7 days. Concurrently he was given Baclofen that was 4 then continued for a further 2 weeks. Unfortunately funding was not available for him to access inpatient detox but despite this he is actively engaging in treatment and taking part in therapies while most of his friends are also now not using. He has recently moved and changed his mobile number in the hope he can avoid old social networks that might want to sell him drugs and finally break free of his pattern of drug abuse. GHB is a dissociative compound most commonly sold in the form of an oily liquid in small bottles or capsules which cost around £15(FRANK, 2013).GHB is both a metabolite and a precursor of the neurotransmitter GABA which occurs endogenously in low levels in the brain (Figure 1). When at naturally occurring levels GHB binds to specific GHB receptors causing the inhibition of GABA release. It has also been implicated in the modulation of several other neurotransmitters including dopamine and serotonin(Schep, et al., 2012). When exogenous GHB is consumed it causes abnormally high levels to occur in the brain where the overall metabolism of GHB is therefore increased and it acts as a partial GABAB receptor agonist. This explains why at low levels GHB can cause euphoria and relaxation but in higher doses cause CNS depression(Bell & Collins, 2011). GHB is popular as it is relatively cheap, is not detected on most routine drug screens and if used occasionally produces no hangover effect(Stein, et al., 2012). Gamma hydroxybutyrate (GHB) was initially developed as an anaesthetic in 1961 and became available to the general public in the 1980s when it was sold in over the counter preparations aimed as health supplements. Papers published in the early 1990s report the first incidences of GHB being used as a drug of abuse following several case reports in the USA of poisoning following intoxication. A restriction on the availability of the substance to the general public consequently came into being and like much of the market of current ‘legal highs’ this legislation inadvertently created a market for analogues of the banned substance. Subsequently gamma butyrolactone (GBL) and 1,4-butanediol (BD) were developed and came to circumvent legal restrictions by being advertised as dietary supplements or cleaning agents(Stein, et al., 2012). GHB was made a class C drug in the UK in 2003 although it is currently licensed in the treatment of narcolepsy with catalepsy and as a substitute agent itself in alcohol detox regimens(Jong, et al., 2012). Considering GHB has been a drug of abuse for several decades and until relatively recently was easily and cheaply available it would be easy to assume it has become a major player in the party drugs scene. However whilst the trend for GHB consumption has been steadily increasing during the 2000s, relative to other synthetic drugs such as MDMA and the amphetamines it is consumed on a much smaller scale. It is interesting to note that the 2003 criminalisation of the substance has so far had no effect on the increasing rate of consumption(EMCDDA, 2013). It could be speculated that this is because the marketing of the substance has changed to be in keeping with legislation (effectively making it legal to possess GHB containing compounds if for industrial cleaning purposes). Alternatively the recipe for GHB has been widely available on the internet for many years and by stockpiling legal compounds that could then be formulated into GHB users may have been unaffected by the law(EMCDDA, 2013). 5 GBL 1,4-butanediol succinic semialdehyde ADH ALDH 4-hydroxybutaldehyde ADH GHB GABA transaminase GABA ALDH succinic acid Figure 1: Metabolic pathway of GHB (adapted fromhttp://en.wikipedia.org/wiki/File:GHB_metabolic_pathway.svg) (ADH = alcohol dehydrogenase, ALDH = aldehyde dehydrogenase) Figure 1 also explains the rationale behind GBL abuse as it is a pro-drug of GHB that is rapidly converted into the active compound. Whilst GBH was made illegal in the UK in 2003, GBL and another pro-drug 1,4-butanediol were not criminalised until 2009. Many GHB abusers will use whichever substance they can access as they produce identical effects hence Darren’s interchangeable use in the case. There is minimal difference in cost between the substances and despite all 3 compounds now being illegal a loophole in UK legislation means GHB containing compounds may still be owned if they are used for industrial purposes (mainly cleaning products). This has reduced the impact of legislation on GHB consumption as it is still readily sold to the UK from websites based abroad in the form of tyre cleaning sets(EMCDDA, 2013). There has however since the criminalisation of the derivative compounds been a shift away from use with 0.4% of 16-24 year olds using tranquilisers in 2012-13 compared with 1% in 2008-09(Home Office, 2013). A well-recognised problem with GHB is the withdrawal syndrome it produces that can occur 1-6 hours after the last dose and cause symptoms for 5-15 days(Bell & Collins, 2011). The commonest symptoms are tremor, hallucinations, tachycardia, insomnia, anxiety and hypertension while less common but important complications include rhabdomyolysis and seizures(Wojtowicz, et al., 2008). 6 Figure 2: Comparing the occurrence of withdrawal symptoms between GHB and its derivatives from a review of 27 case reports or series totalling 57 patients (Taken from (Wojtowicz, et al., 2008)) It was initially suggested that benzodiazepines should be used in high doses at first then tapered off while refractory cases might benefit from barbiturates and that these should occur as inpatients(McDonough, et al., 2004). This has been reinforced by several case series reporting incidences of GHB withdrawal being successfully managed with benzodiazepines(Bell & Collins, 2011). Effectiveness in these incidences is often defined as the ability to get a user to transition from high levels of GHB to tapering levels of benzodiazepines without experiencing withdrawal symptoms. In the UK there are no formal protocols as GHB detox is not common enough to have forced a level of research that would allow for the formal evidence on which to base one. The current thinking though is broadly the same as the initial suggestions although there is some debate as to whether this care can be provided in the outpatient setting given already limited resources in the UK. The main theory for using benzodiazepines as a treatment for GHB withdrawal comes from fact it acts as a GABA receptor agonist. When GHB is suddenly stopped the CNS enters a state of unopposed stimulation (the majority of the withdrawal effects can be attributed to this with the minority to mild autonomic dysfunction). Benzodiazepines cause the same overall increase in GABA as GHB would and thereby oppose the over stimulatory CNS component of withdrawal(Wojtowicz, et al., 2008). The main problem with assessing the effectiveness of any intervention in GHB management is that the majority of the literature is case reports or series with few reviews and no meta-analyses. This may in part explain why there is a lack of concordance then regarding whether benzodiazepines are the most effective way to pharmacologically manage GHB withdrawal. Another issue is that GHB acts on a receptor that is modulated by other common drugs and as such its withdrawal 7 syndrome is on a spectrum with those of alcohol and benzodiazepines themselves. This meant that it took time for GHB withdrawal to be clearly identified and consistently observed in the literature, exacerbated by the fact it is not a common presentation to emergency departments in comparison to the alcohol or benzodiazepines. There have been few studies into alternative agents for detox but some case reports of baclofen being superior to benzodiazepines when the two agents are used together(LeTourneau, et al., 2008). The rationale for this is based on the fact baclofen is a specific GABAB receptor agonist and therefore directly mimics the effects of GHB rather than benzodiazepines which act on GABAA and so only indirectly cause the increase in GABA. Another approach is to use pharmaceutical GHB following the same principal of opioid substitute therapy, i.e.using low doses then tapering to find the correct dose that will block withdrawal symptoms. One incidence of this approach reported that all of the 23 patients involved experienced only minor withdrawal symptoms and none where transferred to intensive care as a result of uncontrolled withdrawal (which has been noted to occur with even high dose benzodiazepines in some literature). Whilst the results are especially encouraging given the high level of concomitant substance use in the sample group, this study like many others lacked the population size to have the statistical power needed to draw conclusions from which protocols could be developed(Jong, et al., 2012). In conclusion the use of party drugs in the UK has increased over the past decade, in line with a European wide trend. The reasons for this are complex and involve a combination of legislature change opening the door for emerging markets and the advancement of the internet for distributing drug recipes and enabling sales. Whilst GHB and GBL use has stabilised in the UK at low levels over the past few years, the problem of newly emerging drugs and their subsequent abuse problems is a challenge that will only continue to grow in the 21st century. In the future, healthcare professionals will face substance users taking compounds that are relative unknown commodities to addiction services. The rationale behind developing protocols for these drugs to reduce withdrawal syndromesand mortality is admirable. Yet with ever increasing pressure on NHS funds there is likely to be debate over the best use of public health resources in treating cases that may involve serious withdrawal but are relatively small in number.It is important that further research is conducted into specific drug withdrawals but the feasibility of providing tailored and highly monitored inpatient detox to these individuals (as is the case in GHB) is unclear as little cost effective analysis has been undertaken.Healthcare professionals can help by making sure they are up to date with new drugs and treatments but in reality this burden will most likely fall on specialist addiction services. Bibliography Bell, J. & Collins, R., 2011. Gamma-butyrolactone (GBL) dependence and withdrawal. Addiction, 106(2), pp. 442-7. EMCDDA, 2013. European Drug Report: Trends and Developments, 8 FRANK, 2013. FRANK GHB Profile. [Online] Available at: http://www.talktofrank.com/drug/ghb [Accessed 10 December 2013]. Home Office, 2013. Drug Misuse: Findings from the 2012/13 Crime Survery for England and Wales Jong, C. A. J., Kamal, R., Dijkstra, B. A. G. & de Haan, H. A., 2012. Gamma-hydroxybutyrate detoxification by titration and tapering. European Addiction Research, 18(1), pp. 40-5. LeTourneau, J. L., Hagg, D. S. & Smith, S. M., 2008. Baclofen and gamma-hydroxybutyrate withdrawal. Neurocritical Care, 8(3), pp. 430-3. McDonough, M., Kennedy, N., Glasper, A. & Bearn, J., 2004. Clinical features and management of gamma-hydroxybutyrate (GHB) withdrawal: a review. Drug Alcohol Dependence, Volume 75, pp. 3-9. NICE, 2008. Drug Misuse: Opioid Detoxification. CG52. London: National Institute for Health and Care Excellence. Schep, L. J. et al., 2012. The clinical toxicology of gamma-hydroxybutyrate, gammabutyrlactone and 1,4-butanediol. Clinical Toxicology, 50(6), pp. 458-70. Stein, L. A. R. et al., 2012. Preliminary web-based measures development for GHB: expectancies, functions, and withdrawal. The American journal of drug and alcohol abuse, 38(2), pp. 121-9. van Amsterdam, J. G. C., Brunt, T. M., McMaster, M. T. B. & Niesink, R. J. M., 2012. Possible long-term effects of γ-hydroxybutyric acid (GHB) due to neurotoxicity and overdose. Neuroscience and Biobehavioural Reviews, 36(4), pp. 1217-27. Winstock, A. R. & Mitcheson, L., 2012. New recreational drugs and the primary care approach to patients who use them. BMJ, Volume 344, p. e288. Wojtowicz, J. M., Yarema, M. C. & Wax, P. D., 2008. Withdrawal from gammahydroxybutyrate, 1,4-butanediol and gamma-butyrolactone: a case report and systematic review. CJEM, 10(1), pp. 69-74. Word Count: 4273 9