Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Electrocardiography wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Cardiac surgery wikipedia , lookup
Coronary artery disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Myocardial infarction wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
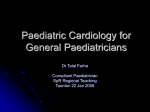
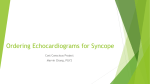
Syncope and The Older Patient Debra L. Bynum, MD Division of Geriatric Medicine Pretest… 1. The ECG has the greatest value in its (NPV or PPV) in the diagnosis of a cardiac etiology for syncope 2. History: 75 year old man reports presyncopal symptoms that occur while he is driving backwards out of his driveway in the morning. This suggests … 3. History: an 80 year old man reports an episode of syncope that occurred after doing arm exercises for a rotator cuff injury. This suggest… 4. The only independent predictor of a cardiac etiology of syncope is a past history of … 5. ____ is a neurodegenerative disease characterized by profound autonomic insufficiency and parkinsonian features on exam 6. An 82 year old man presents with postural hypotension, an idiopathic peripheral neuropathy, significant proteinuria and your attending orders a rectal biopsy to look for____ 7. Name 3 causes of “situational syncope” 8. Older patients are more likely to have positive a. tilt table tests b. carotid sinus massage c. orthostatic hypotension d. all of the above Pretest: bonus question Sudden cardiac death in young men (originally described in young asian men) associated with this sign on EKG is known as what syndrome? Syncope: Definition Sudden and temporary loss of consciousness with inability to maintain postural tone, followed by spontaneous recovery Causes of Syncope Neurally Mediated (up to 58% in some series) Orthostatic/postural Cardiac arrhythmia (20-25%) Structural cardiac or pulmonary causes Cerebrovascular or psychiatric (1%) Unknown (18-30%) Syncope in the Elderly Usually multifactorial Often confounded by findings (orthostasis and carotid hypersensitivity common and may be found and yet not be the cause…) Prevalence up to 25% in nursing home population over age 70 Higher pretest probability of cardiac disease or arrhythmia Importance of History and PE Up to 70% of patients in prospective studies had probable cause identified based upon history, physical exam and ecg The History… History of Heart Disease – – The ONLY independent predictor of cardiac cause (sens 95%, spec 45%) Absence of heart disease up to 97% specific to rule out cardiac etiology (good NPV) The History Position – – – Presyncopal symptoms – – Supine: cardiac until proven otherwise Upon sitting/standing: orthostasis Prolonged standing: venous pooling/orthostasis/vasovagal Presence suggests vasovagal, but does not rule out arrhythmia Lack of suggests arrythmia (up to 65% with sudden syncope) Dyspnea (Pulmonary embolus) Focal neurologic symptoms (TIA, seizure) Seizure like activity (including loss of bowel and bladder control, tongue bite, postictal state) The history… Recovery period – – – Situational syncope (vasovagal) – – – – Instant: arrythmia Feeling hot and nauseated: vasovagal Confusion/lethargy: postictal Cough Swallow (cold liquid) Micturition (urination) Defecation Exertional – Ventricular tachyarrhythmia – – Aortic stenosis or HOCM Pulmonary Hypertension The history… Prior “faint” 1-4 years prior suggest vasovagal Age Medications – – – – Tricyclic antidepressants Nitrates Alpha adrenergic antagonists Diuretics Injury (facial suggests arrhythmia) Postprandial (vagally mediated) Specific Causes and Treatment Options for Syncope Postural Hypotension – – – Drop in systolic blood pressure of over 20 Medications Autonomic Insufficiency – No reflex tachycardia Shy-Drager (multiple systems atrophy) Primary autonomic failure Parkinson’s Disease Diabetes Aging Amyloid Volume Loss Dehydration Blood loss Autonomic Insufficiency and Orthostatic Hypotension Treatment Options – – – – – – – – – – – – – Review of medications Avoid volume depletion Arising slowly Tensing crossed legs while standing Dorsiflex feet or handgrip prior to standing Thigh high Jobst stockings (decreases venous pooling) Avoid prolonged standing (venous pooling) Increased salt diet Smaller meals to avoid postprandial drop in BP Fludrocortisone Midodrine (alpha 1 adrenergic agonist) Phenylephrine (not usually used in older patients) Fluoxetine Mechanical Cardiac Causes Obstruction to LV outflow – – – – Aortic Stenosis HOCM Left atrial myxoma Mitral Stenosis Obstruction to pulmonic flow – – – – Pulmonic stenosis Pulmonary HTN PE (can also have vasovagal type syncope associated with smaller PEs) Right atrial myxoma Other Mechanical Cardiac Causes Large MI with LV dysfunction CHF Tamponade Aortic dissection Cardiac Arrhythmias Bradycardia – – – Sick sinus syndrome 2nd or 3rd degree AV block Pacemaker malfunction Tachycardia – – – – Ventricular tachycardia Ventricular fibrillation SVT If you see atrial fibrillation, think sick sinus syndrome as potential cause of syncope… Brugada Syndrome Triad – – – RBBB pattern in right precordial leads Transient/persistent ST elevation in v1-v3 Sudden cardiac death Structurally normal heart Association with young and healthy men from southeast asia who present with sudden cardiac death Brugada sign may be asymptomatic High risk of sudden cardiac death in those who have syncope or family history of sudden death (Indication for AICD based upon observational data) Brugada Sign Implantable Cardioverter-Defribrillator Guidelines AICD indicated for patients with spontaneous Vtach with underlying heart disease or in patients with normal heart when vtach not amenable to other treatments AICD guidelines Ischemic Cardiomyopathy – – – LVEF <30% At least 1 month after MI and 3 months after revascularization MADIT-II trial – – – Multicenter Automatic Defibrillator Implantation Trial 5.6% ARR in mortality over 4 years Results support prophylactic AICD, but not considered cost wise Based upon subset analysis, Current recommendation in those with QRS >120 ms Unclear result: those with ICDs had 5% absolute increased risk of hospitalization for CHF (19% vs 14%): ?artifact, ?due to living longer?, ?detrimental AICD guidelines… Syncope in patients with advanced structural heart disease – High risk of sudden cardiac death Inducible Vtach with structural heart disease Inducible Vtach with normal heart that is not amenable to ablation therapy Subclavian Steal Syndrome Proximal subclavian artery stenosis Decreased blood flow to distal subclavian artery worsened with exertion of arm Blood from vertebral artery on opposite side goes to basilar artery and then down ipsilateral vertebral artery, away from brainstem, to serve as collateral for arm Usually asymptomatic Atherosclerosis Symptoms of vertebrobasilar insufficiency (dizziness, vertigo, diplopia, nystagmus) Rare to have permanent neurological deficits Diagnosis with dopplers, MRA Treatment: surgical revascularization, stents Cerebrovascular Disease Less common cause of true syncope Vertebrobasilar disease (presyncope) Drop Attacks Vasovagal/Neurocardiogenic syncope Situational Syncope – – – – Micturition Defecation Cough Swallow Recurrent Neurocardiogenic Syncope Posprandial The FAINT Vasovagal Syncope Presyncopal symptoms Setting (procedure, pain, anxiety) Prior history Neurally Mediated Syncope Cardiac sensory receptors in LV stimulated by stretch Increased neural discharge to vasomotor center in medulla Increased parasympathetic tone and decreased sympathetic activity Sudden bradycardia and hypotension Recurrent Neurocardiogenic Syncope Upright posture lead to pooling of blood in lower extremities Decreased venous return Normal response: reflex tachycardia and forceful LV contraction and vasoconstriction Susceptible individuals: activation of mechanoreceptors triggers reflex bradycardia and hypotension Response triggered by forceful LV contraction with prolonged standing or with increased catecholamines (anxiety, fear, panic, pain) Treatment of Recurrent Neurocardiogenic Syncope Medications – Paroxetine – Midodrine – Alpha adrenergic agonist Small studies Fludrocortisone – Only agent shown effective in RCT No good study Beta blockers Often used, mixed evidence in studies Pacemakers in the treatment of Recurrent Neurocardiogenic Syncope 3 large RCTs of permanent pacing – North American Vasovagal Pacemaker Study (VPS-1) – Vasovagal Syncope International Study – Patients with over 6 episodes, positive tilt table test with significant bradycardia Significant decrease in recurrence with pacer (HR .087) 5% recurrence with pacemaker vs 61% without (19 patients) Syncope Diagnosis and Treatment Study Pacemaker vs atenolol 93 patients: 4.3% recurrence vs 26% Pacemakers and neurocardiogenic syncope: Problems with trials… – – – Small numbers of patients Not blinded Highly selected patients Patients had profound bradycardia on tilt table testing and multiple episodes Pacers and neurocardiogenic syncope… Bottom line: – May benefit patients with recurrent episodes of clear neurally mediated syncope, associated with significant bradycardic response, who have a decreased QOL otherwise (injuries, driving, etc) Carotid Sinus Hypersensitivity ?Role of Carotid Sinus Massage – – – – Some recommend if no bruits, recent MI, cva or history of vtach ?monitor Positive response: 3 sec pause In literature, but most cardiologists would not recommend High yield of carotid massage in elderly (up to 40% over the age of 75 may have a positive response), but not specific in identifying this as the cause of syncope (PPV not known) History: syncope/presyncope with turning neck, backing up in car, wearing tight collar Evaluation of Syncope When a cause of syncope is identified, history and physical lead to etiology in up to 85% cases The only independent predictor of a cardiac cause of syncope is the presence of underlying heart disease (95% sens, only 45% spec) Orthostasis May be confounder in older patients Up to 25% of older patients may have orthostasis when tested, the presence of orthostasis may be true, true and unrelated… The ECG Prolonged QT Bradycardia, AVN disease, MI, HOCM, Brugada Only 2-10% will have diagnostic abnormality Up to 50% of patients with syncope have abnormal EKG Greatest use in NPV (negative predictive value) of NORMAL ECG The Holter Monitor 24-48 hours continuous ECG No added yield with 72 hours Low yield unless frequent symptoms Up to 70% of Holter studies negative for diagnosis One series: only 5% of studies had arrhythmia that correlated with symptoms Probably good NPV if symptoms documented with benign rhythm Event or Loop Monitors Higher yield than holter (up to 55% positive yield of symptom-arrhythmia correlation in some series) Problem with patient education and ability to activate monitor correctly (25% of patients have difficulty) May be especially problematic in the very elderly or those with dementia Implantable Loop Recorder Prolonged monitoring for those with syncope of unclear etiology despite workup, especially for those in whom cardiac etiology is suspected Several small studies suggest that in very selected patients, may increase yield of diagnosis to almost 85% Other Cardiac Tests Echo Exercise or Functional Tests EP studies Most useful when history or physical suggests specific further testing to be done… Tilt Table Testing… Passive or Isoproterenol Test: patient held in upright position at 40-90 degrees and observed for symptoms and hypotension or bradycardia Passive testing: sensitivity of 70%, specificity of 90-100% Isoproterenol: only 55% specificity Overall little to add to history and PE; lack of sensitivity with passive testing and lack of specificity with induced testing limits usefulness of test… Lab tests… The basics (anemia) ?BNP: some studies report usefulness as a marker for cardiac cause of syncope: sensitivity of 82% and specificity of 92%, Likelihood ratios of pos and neg tests probably not more useful than pretest probability of underlying heart disease based upon history and physical exam CK, MB and Troponins – – More useful if positive (greater PPV) than neg One series: up to 10% nursing home patients presenting with syncope had positive enzymes… The Least Useful Tests… CT head with negative neurological exam EEG with no neurological symptoms Carotid Artery Dopplers (useful for evaluation of CVA or TIA, not useful for evaluation of syncope without vertebrobasilar symptoms…) The Older Patient Positive tests that are more common in the elderly and not necessarily the cause of the syncope: – – – Orthostasis Positive carotid massage Positive tilt table testing Up to 54% of older patients with syncope may have positive test… Positive test in 10% of asymptomatic elderly! Algorithm for diagnosing syncope Linzer, M. et. al. Ann Intern Med 1997;127:76-86 Summary of Charges for Diagnostic Tests in Syncope* Linzer, M. et. al. Ann Intern Med 1997;127:76-86 Summary Syncope in the older patient usually multifactorial Tailor tests based upon history and physical exam Elderly more likely to have positive tests that may be confounders… Elderly more likely to have underlying heart disease and higher pretest probability of a cardiac etiology Use algorithms in older, complicated patients with great caution!!! Back to the Pretest… 1. The ECG has the greatest value in its (NPV or PPV) in the diagnosis of a cardiac etiology for syncope 2. History: 75 year old man reports presyncopal symptoms that occur while he is driving backwards out of his driveway in the morning. This suggests … 3. History: an 80 year old man reports an episode of syncope that occurred after doing arm exercises for a rotator cuff injury. This suggest… 4. The only independent predictor of a cardiac etiology of syncope is a past history of … 5. ____ is a neurodegenerative disease characterized by profound autonomic insufficiency and parkinsonian features on exam 6. An 82 year old man presents with postural hypotension, an idiopathic peripheral neuropathy, significant proteinuria and your attending orders a rectal biopsy to look for____ 7. Name 3 causes of “situational syncope” 8. Older patients are more likely to have positive a. tilt table tests b. carotid sinus massage c. orthostatic hypotension d. all of the above Answers to Pretest… 1. NPV 2. Carotid Hypersensitivity 3. Subclavian steal syndrome 4. Cardiac history 5. Multiple Systems Atrophy (shy-drager) 6. amyloid 7. micturition, defecation, cough, swallow 8. all of the above 9. bonus: brugada syndrome Selected References Benditt DG, VanDjjk JG, Sutton R. Syncope: Curr Prob Cardiol 2004; 29(4): 152-229 Epstein AE. An update on implantable cardioverter-defibrillator guidelines. Curr Opin Cardiology 2004; 19(1): 23-25 Littman L et al. Brugada syndrome and Brugada sign. Am Heart J 2003; 145(5): 768-778 Raj S, Sheldon RS. Role of pacemaker in treating neurocardiogenic syncope. Curr Opinion Cardiol 2003; 18: 47-52 Gregoratos G, Cheitlin MD, Conill A. ACC/AHA guidelines for implantation of cardiac pacemakers and antiarrthythmia devices: executive summary: a report of the American College of Cardiology/Am Heart Assoc Task Force on Practice Guidelines. Circulation. 1998; 97: 1325-1335 Connolly SJ et al. The North American Vasovagal Pacemaker Study. J Am Coll Cardiol 1999; 33: 16-20 DiGirolamo et al. Effects of paroxetine on refractory vasovagal syncope. J Am Coll Cardiol 1999; 33: 1227-30 Sutton R et al. Dual chamber pacing in the treatment of neurally mediated tilt-positive cardioinhibitory syncope (VASIS). Circulation 2000; 102: 294-299 Selected References… Krahn Ad et al. Use of the implantable loop recorder in evaluation of patients with unexplained syncope Kapoor WN. Current evaluation and management of syncope. Circulation 2002; 106: 1606 Alboni P et al. Diagnostic Value of history in patients with syncope. J Am Coll Cardiol 2001; 37: 1921 Kapoor et al. Evaluation and outcome of patients with syncope. Medicine 1990; 69: 160 Linzer et al. Diagnosing syncope: part I. Ann Int med 1997; 126:989 Linzer et al. Diagnosing syncope: part II. Ann Int Med 1997; 127: 76