Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Drug interaction wikipedia , lookup
Discovery and development of proton pump inhibitors wikipedia , lookup
Adherence (medicine) wikipedia , lookup
Discovery and development of non-nucleoside reverse-transcriptase inhibitors wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Pharmaceutical marketing wikipedia , lookup
Patent medicine wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Prescription costs wikipedia , lookup
Pharmacognosy wikipedia , lookup
CCR5 receptor antagonist wikipedia , lookup
Prescription drug prices in the United States wikipedia , lookup
Compounding wikipedia , lookup
Medical prescription wikipedia , lookup
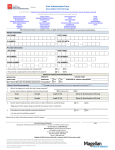
Prior Authorization Form Compounded Prescriptions Access this PA form at https://tenncare.magellanhealth.com/static/docs/Prior_Authorization_Forms/TennCare_Compounds_PA_Request_Form.pdf If the following information is not complete, correct, or legible, the PA process can be delayed. Use one form per member please. Member Information LAST NAME: FIRST NAME: ID NUMBER: DATE OF BIRTH: – – Prescriber Information LAST NAME: FIRST NAME: NPI NUMBER: DEA NUMBER: PHONE NUMBER: FAX NUMBER: – – – – PRESCRIBER CLINIC/OFFICE NAME: ADDRESS: CITY: Is the prescriber a TennCare provider with a Medicaid ID? Yes No Is the prescriber a single-patient contract holder for this patient? Yes No STATE: ZIP CODE: STATE: ZIP CODE: Pharmacy Information PHARMACY NAME: ADDRESS: CITY: PHONE NUMBER: FAX NUMBER: – – This facsimile transmission contains legally privileged and confidential information intended for the parties identified below. If you have received this transmission in error, please immediately notify us by telephone and return the original message to TennCare Pharmacy Program, c/o Magellan Health Services, 1st Floor South, 14100 Magellan Plaza, Maryland Heights, MO 63043. Distribution, reproduction or any other use of this transmission by any party other than the intended recipient is strictly prohibited. © 2016, Magellan Health Services. All Rights Reserved. Revision Date: 09/01/2016 – – Prior Authorization Form Compounded Prescriptions Access this PA form at https://tenncare.magellanhealth.com/static/docs/Prior_Authorization_Forms/TennCare_Compounds_PA_Request_Form.pdf Criteria for Approval ALL of the following MUST be met for approval: The drug manufacturer has a signed rebate agreement with CMS. TennCare considers bulk chemical supplies used in compounded prescriptions as nondrug items, which do not require a drug rebate agreement. The Bureau covers such bulk chemical supplies only as specifically approved by the department. The enrollee's drug therapy needs are unable to be met by commercially available dosage strengths and/or forms of the drug, as indicated by one of the following: Per FDA-approved dosing, patient’s age or weight requires a dose or route of administration for which there is no commercially available product Children age 12 and older that have trouble swallowing, or adults with documented dysphagia or with feeding tube and require administration with an oral liquid, or by topical, rectal, or other appropriate non-oral routes, when these routes of administration are not commercially available OR Patients who have sensitivity to dyes, preservatives, or fillers in commercial products and require allergy-free medications as documented in the medical record, OR There is a current supply shortage of the commercial product OR The commercial product has been discontinued by the pharmaceutical manufacturer for reasons other than lack of safety or effectiveness (provider must submit documentation to support request for off-label use. The compounded product contains at least one covered prescription-only ingredient The vehicle or base used in the compound does not qualify as the sole covered legend ingredient. The active ingredient(s) in the compounded product is FDA-approved, or is supported by peer-reviewed medical literature for the diagnosis in the requested route of delivery. If any ingredient in the compounded product requires Prior Authorization, the patient must meet the Prior Authorization criteria for that ingredient, When oral dosage forms are used in compounds, the most cost-efficient strength meeting the needs of the compound should be used- e.g., #10 Tacrolimus 5mg capsules to be used instead of #100 Tacrolimus 0.5mg capsules Must be prescribed by a prescriber with a Tennessee Medicaid Provider ID Criteria for Denial Compounded Product may be denied if it meets ANY of the following: The compound does not contain any prescription-only ingredient otherwise covered by the plan. The compound is being used for cosmetic purposes. The compound includes prescription ingredients for non-FDA approved indications or purposes given the route of delivery. The compound includes investigational or experimental drugs Compounded formulations that use drugs withdrawn or removed from the market for safety reasons The compound contains extended release formulations or orally disintegrating formulations. Compounded formulations to replace, or copy drug products not covered by or requiring Prior Authorization by TennCare. Prescription ingredients compounded for the purpose of convenience only. Any compound containing insulin of any type Compounds for hormone therapy for treatment of menopause or for androgen decline in the aging male. Compounds for the purposes of diluting higher strength topical corticosteroids, when lower strength topical corticosteroids are commercially available. Compounds for the purposes of adding urea, or other emollient to topical corticosteroids for skin softening Compound contains any bulk substance classified as category 2 or 3 by FDA under 503A or 503B Compounds for topical use that contain any of the following ingredients: Amitriptyline Clonidine Diclofenac Ketoprofen Piroxicam © 2016, Magellan Health Services. All Rights Reserved. Amantadine Cyclobenzaprine Gabapentin Meloxicam Sucralfate Baclofen Dextromethorphan Indomethacin Nabumetone Tramadol Page 2 of 4 Cholestyramine Duloxetine Ketamine Orphenadrine Flurbiprofen (excluding ophth solution) Prior Authorization Form Compounded Prescriptions Access this PA form at https://tenncare.magellanhealth.com/static/docs/Prior_Authorization_Forms/TennCare_Compounds_PA_Request_Form.pdf Clinical Criteria Documentation ****Do not include documentation that is not requested on this form**** 1. List the route of administration for the compound: Oral Topical Other:_____________________ 2. List the patient’s diagnosis which this compound is intended to treat ____________________________________________ 3. Is a similar commercially available product available? Yes No If yes, indicate why a commercially available product is not acceptable and include the specific need for the compound; list previous failed therapies if known : _____________________________________________________________________________________________________________________________________________________________ _____________________________________________________________________________________________________________________________________________________________ 4. Is the active ingredient(s) of the compound FDA-approved for the condition being treated in the requested route of administration? Yes No If no, please attach peer-reviewed medical evidence for support. 5. Level of Effort Requested Level 1 6. Hands-on compounding time: 5 – 15 minutes 7. Special equipment used: 8. Special considerations: Level 2 Laminar flow hood comments) Complex formulation Level 3 16 – 30 minutes Unguator Over 30 minutes Homogenizer Sterility Testing N/A (or if other, explain in N/A (or if other, explain in comments) 9. Additional Information: ________________________________________________________________________________ __________________________________________________________________________________________________________ __________________________________________________________________________________________________________ © 2016, Magellan Health Services. All Rights Reserved. Page 3 of 4 Prior Authorization Form Compounded Prescriptions Access this PA form at https://tenncare.magellanhealth.com/static/docs/Prior_Authorization_Forms/TennCare_Compounds_PA_Request_Form.pdf List the NDC, name, dosage form, and qty of each ingredient. Each ingredient used in the compound MUST be listed. Begin the list with the covered legend drugs. Please attach an additional form if compound has greater than 10 ingredients. Rx Required Active Ingredient Base/ Vehicle Excipient /Other NDC Drug Name Prescriber Signature (Required) Quantity Date (By signature, the Prescriber confirms the above information is accurate and verifiable by patient records.) (Note: Pharmacist may sign as agent of Prescriber IF copy of compound prescription is submitted with this request) Fax This Form to: 1-866-434-5523 Mail requests to: TennCare Pharmacy Program c/o Magellan Health Services 1st floor South, 14100 Magellan Plaza Maryland Heights, MO 63043 Phone: 1-866-434-5524 Magellan Health Services will provide a response within 24 hours upon receipt. © 2016, Magellan Health Services. All Rights Reserved. Dosage Form Page 4 of 4