Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
1198
JACC Vol. 6. No.6
December 1985:1198-9
Classification of Sports
JERE H. MITCHELL, MD, FACC, C. GUNNAR BLOMQVIST, MD, FACC,
WILLIAM L. HASKELL, PHD, FACC, FREDERICK W. JAMES, MD, FACC,
HENRY S. MILLER, JR., MD, FACC, WILLIAM W. MILLER, MD, FACC,
WILLIAM B. STRONG, MD, FACC
Sports may be classified according to the type and intensity
of exercise performed and to the danger of body collision
(l,2). A classification of sports is given in Table 1 which
divides exercise into two general types: static (isometric)
and dynamic (isotonic) (3,4) and categorizes the intensity
of exercise into low, medium or high. It also lists those
sports that pose significant danger of body collision, either
because of the probability of hard impact between compet•
itors or between a competitor and an object, and the further
danger the athlete would be exposed to if syncope occurred.
Dynamic exercise involves changes in muscle length and
joint movement with rhythmic contractions which develop
a relatively smaller force, whereas static exercise involves
development of a relatively larger force with little or no
change in muscle length or joint movement. These two types
of exercise should be thought of as the two extremes of a
continuum with most physical activity having both static
and dynamic demands. For example, distance running,
swimming and rhythmic calisthenics have principally dy•
namic demands and weight lifting, water skiing and gym•
nastics have principally static demands.
Dynamic exercise performed with a large muscle mass
causes a marked increase in oxygen consumption and car•
diac output. There is an increase in systolic blood pressure;
however, diastolic and mean pressures remain relatively
constant and peripheral vascular resistance decreases. On
the other hand, static exercise, which usually involves a
much smaller muscle mass than dynamic exercise, causes
a smaller increase in oxygen consumption and cardiac out•
put. There is a marked increase in systolic, diastolic and
mean arterial pressure; however, peripheral vascular resist•
ance increases only slightly. During dynamic exercise there
is an increase in stroke volume with small changes in mean
arterial pressure, whereas during static exercise the stroke
volume changes little with an increase in mean arterial pres•
sure. Thus, dynamic exercise may be thought of as primarily
© 1985 by the American College of Cardiology
causing a volume load, and static exercise as producing a
pressure load, on the left ventricle.
Both static and dynamic exercise change several factors
that are important in determining myocardial oxygen de•
mand: heart rate, wall tension and contractile state of the
ventricle (5,6). Wall tension is affected by pressure devel•
opment and ventricular volume. In dynamic exercise, there
is a large increase in heart rate and an increase in stroke
volume, which is achieved both by an increase in end•
diastolic volume (Frank-Starling mechanism) and a decrease
in end-systolic volume (increased contractile state). In static
exercise there is a smaller increase in heart rate and little
change in end-diastolic and end-systolic volumes of the left
ventricle. However, arterial pressure and contractile state
of the ventricle are increased. Thus both dynamic and static
exercise cause increases in factors that are important in
determining myocardial oxygen demand.
There are important limitations to the classification of
sports according to the type and intensity of exercise per•
formed as presented in Table 1. For example, it does not
consider the emotional stress a particular athlete experiences
during a specific event. Thus, although competitive golf has
low dynamic and static demands, during championship com•
petition the subject may be exceedingly anxious and the
resulting catecholamine response cause marked increases in
heart rate or arterial pressure, thereby increasing myocardial
oxygen demand. In addition, the classification scheme does
not take into consideration the training programs required
for each of the specific sports that might require a different
type and increased intensity of exercise (and thereby risk)
above and beyond that of the competitive event itself.
Finally, this classification may be of theoretical interest
but its practical value is unknown because our current
knowledge regarding the relative risks of these two types of
exercise for various cardiovascular abnormalities is
limited.
0735-1097/85/$3.30
MITCHELL
CLASSIFICATION OF SPORTS
lACC Vol. 6. No.6
December 19X5:1198-·Y
1199
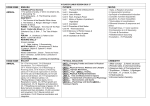
Table I. Classification of Sports
I. Intensity and type of exercise performed
A. High to moderate intensity
I. High to moderate dynamic and static demands
Boxing
Crew/rowing
Cross-country skiing
Cycling
Downhill skiing
Fencing
football
Ice hockey
Rugby
Running (sprint)
Speed skating
Water polo
Wrestling
2. High to moderate dynamic and low static demands
Badminton
Baseball
Basketball
Field hockey
Lacrosse
Orienteering
Ping-pong
Race walking
Racquetball
Running (distance)
Soccer
Squash
Swimming
Tennis
Volleyball
3. High to moderate static and low dynamic demands
Archery
Auto racing
Diving
Equestrian
Field events (jumping)
Table I. «('()ntinueJ)
field events (throwing)
Gymnastics
Karate or judo
Motorcycling
Rodeoing
Sailing
Ski jumping
Water skiing
Weight lifting
B. Low intensity (low dynamic and low static demands)
Bowling
Cricket
Curling
Golf
Riflery
II. Danger of body collision
Auto racing*
Bicycling"
Boxing
Dlving*
Downhill skiing*
Equestrian'"
Football
Gymnastics *
Icc hockey
Karate or judo
l,acn)~~c
Motorcycling*
Polo*
Rodeoing*
Rugby
Ski jumping*
Soccer
Water polo*
Water skiing*
Weight lifting*
Wrestling
*Increased risk if syncope occurs.
References
I. Shaffer TE. The health examination for participation in sports. Pediatr
Ann 1978:7:27-40.
2. Strong WB, Alpert BS. The child with heart disease: play. recreation
and sports. Curr Prob Cardiol 1981 :6: 1-38.
3. Mitchell JH, Wildenthal K. Static (isometric) exercise and the heart:
physiological and clinical considerations. Annu Rev Med 1974:25:369-81.
4. Asmussen E. Similarities and dissimilarities between static and dynamic
exercise. Cire Res 19~n:48(6)(suppll):3-IO.
5. Sonnenblick EH, Ross J Jr, Braunwald E. Oxygen consumption of the
heart. Newer concepts of its multifactorial determination. Am J Cardiol
1968:22:328-36.
6. Mitchell JH, Hefner LL, Monroe RG. Performance of the left ventricle.
Am J Med 1972:53:481-94.