Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
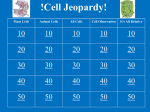
Basic Research—Technology Evaluation of Interference of Cellular Phones on Electronic Apex Locators: An In Vitro Study Preena Sidhu, MDS,* Swapnil Shankargouda, MDS,† Daniel DevaPrakash Dicksit, MPH,* Haydar Majeed Mahdey, MDS,* Danish Muzaffar, MDS,* and Shelly Arora, MDS* Abstract Introduction: Use of mobile phone has been prohibited in many hospitals to prevent interference with medical devices. Electromagnetic radiation emitted from cellular phones might interfere with electronic working length determination. The purpose of this in vitro study was to evaluate the effect of a smart phone (Samsung Galaxy Note Edge) on working length determination of electronic apex locators (EALs) Propex II and Rootor. Methods: Fifteen intact, non-carious single-rooted teeth were decoronated at the cementoenamel junction. Visually, working length was determined by using a #15 K-file under stereomicroscope (20). The effect of cellular phones on electronic working length (EWL) was determined under 2 experimental settings: (1) in a closed room with poor signal strength and (2) in a polyclinic set up with good signal strength and 5 conditions: (1) electronically, without cellular phone in room; (2) electronically, with cellular phone in physical contact with EAL; (3) electronically, with mobile phone in physical contact with EAL and in calling mode for a period of 25 seconds; (4) electronically, mobile phone placed at a distance of 40 cm from the EAL; and (5) electronically, mobile phone placed at a distance of 40 cm and in calling mode for a period of 25 seconds. The EWL was measured 3 times per tooth under each condition. Stability of the readings was scored from 1 to 3: (1) good stability, (2) stable reading after 1 attempt, and (3) stable reading after 2 attempts. The data were compared by using analysis of variance. Results: The EWL measurements were not influenced by the presence of cellular phone and could be determined under all experimental conditions. Conclusions: Within the limitations of this study, it can be concluded that mobile phones do not interfere with the EWL determination. (J Endod 2016;42:622–625) Key Words Cellular phone, electromagnetic interference, electronic apex locator, working length determination R oot canal therapy is an integral part of dental practice. The success of root canal therapy depends on various factors among which correct working length estimation is a crucial step. Electronic apex locators (EALs) have been used worldwide for working length determination. These devices can help reduce treatment time and radiation dose to the patient (1). Various factors such as correct usage, presence of irrigants, vital or necrotic pulp, inflammatory exudate, and obturating material (2–7) in the root canal, contribute to the accuracy of EALs. Moreover, studies have shown that EALs provide accurate working length estimation when compared with the radiographic method (6). It is known that electromagnetic radiation emitted from devices such as cellular phones, iPods, dental devices such as electronic pulp testers, electrosurgery units, and ultrasonic scalers can interfere with the function of implanted cardiac pacemakers in patients with implanted cardiac devices (8–10). Electrical energy from these dental devices can travel down the lead wires and can induce ventricular or atrial fibrillation and reprogram the cardiac device (11). Studies have reported that cellular phones can inhibit the function of a pacemaker, and this depends on the distance between the pacemaker and the electronic device, power output of the electronic device, type of pacemaker, age of pacemaker, and model of the cellular phone (12–14). It is suggested that the use of cellular phones should be restricted in hospitals because electromagnetic interference (EMI) caused by cellular phones can interfere with functions of medical devices (15). Allowing usage of cellular phones in non-patient areas, restrictions in clinical areas, cellular phone safe wards, and use of distance greater than 1 m from all medical equipment are some precautions taken to prevent this interference (15, 16). A dental office has no such limitations for the use of cellular phones in dental operatory. Cellular phones are used by the dentist, dental surgery assistants, and patients in close proximity to dental devices. The technical support documents of EALs such as Root ZX (J Morita Corp, Tokyo, Japan), Propex II (Dentsply Maillefer, Ballaigues, Switzerland), and Rootor (Meta Biomed, Cheongwon-gun, Korea) state that EMI from portable and mobile radiofrequency communications equipment such as cellular phones can cause interference with accurate reading of the EAL and should not be used close to any part of the EAL. There is limited evidence base that can help a dental practitioner come to a decision whether mobile phones can be used in close proximity to EALs and whether these devices can have any effect on the electronic working length (EWL) determination. This in vitro study aimed to evaluate the reliability of EALs (Propex II and Rootor) when placed in contact and in close proximity with a smart phone (Samsung Galaxy Note Edge; Samsung Electronics, Suwon, Korea) in different experimental conditions. From the *Faculty of Dentistry, SEGi University, Jalan Teknologi, Kota Damansara, Selangor, Malaysia; and †KLE University VK Institute of Dental Sciences, Jawaharlal Nehru Medical College Campus, Karnataka, India. Address requests for reprints to Dr Preena Sidhu, Faculty of Dentistry, SEGi University, Jalan Teknologi, Kota Damansara, 47810 Petaling Jaya, Selengor, Kuala Lumpur, Malaysia. E-mail address: [email protected] 0099-2399/$ - see front matter Copyright ª 2016 American Association of Endodontists. http://dx.doi.org/10.1016/j.joen.2015.12.027 622 Sidhu et al. JOE — Volume 42, Number 4, April 2016 Basic Research—Technology Materials and Methods Dental Samples Fifteen single-rooted teeth with 1 canal and mature apices were selected for this study. Roots were examined under magnification (Leica Microsystems, Wetzlar, Germany) with a magnification of 20, and roots with carious lesions, fractures, resorptions, immature apices, or any other anatomic irregularities were excluded. The teeth were sectioned at cementoenamel junction for simplified access to root canal and to obtain a reproducible reference point. The sectioned teeth were stored in distilled water at 4 C for further use. EAL Two different EALs were used in this study: 1. The Propex II (Dentsply Maillefer, Ballaigues, Switzerland), a multifrequency-based EAL that records the signals of 2 alternating currents of 0.5 kHz and 8.0 kHz 2. The Rootor (Meta Biomed, Cheongwon-gun, Korea), a multiple frequency EAL that uses 2 frequencies of 0.5 kHz and 5 kHz Cellular Phone Samsung Galaxy Note Edge, a 4G LTE (Long-Term Evolution) multiband android smart phone used with a network provider Maxis Communications (Berhad, Malaysia), was used in this study. Experimental Setting The experiment was carried out in 2 different settings, one in a closed room (9 9 feet) and the other in a dental polyclinic (26 40 feet) in a university setting that has cubicles (9 9 feet), to record whether the EWL differed between the 2 settings: 1. In a closed room with weak signal strength and where Bluetooth, WiFi, and General Packet Radio Service (GPRS) were inactivated: No phone in the room (control group) Phone placed in physical contact with EAL in standby mode Phone placed in physical contact with EAL and in calling mode for a period of 25 seconds Phone placed at a distance of 40 cm from the EAL in standby mode Phone placed at a distance of 40 cm and in calling mode for a period of 25 seconds 2. In a dental polyclinic with cubicles with good signal strength where Bluetooth, Wi-Fi, and GPRS were activated: Dental students and personnel carrying cellular phones with them in standby mode in vicinity of the cubicle (control group) Phone placed in physical contact with EAL in standby mode Phone placed in physical contact with EAL and in calling mode for a period of 25 seconds Phone placed at a distance of 40 cm from the EAL in standby mode Phone placed at a distance of 40 cm and in calling mode for a period of 25 seconds the file tip was just visible at the apical foramen under the stereomicroscope (Leica Microsystems) with a magnification of 20. The silicone stop was placed at the reference point. The distance from the base of the silicone stop to the file tip was measured with an endodontic ruler (Dentsply Maillefer USA, Tulsa, OK). The lengths were measured to an accuracy of 0.25 mm. The measurements followed a random sequence, each measurement was repeated 3 times, and the mean value was calculated. Determination of EWL The EWL was established by using an experimental model described by Hurstel et al (17). Two holes were perforated in the screw cap of a plastic container, and the tooth along with the lip clip of the EAL was inserted through the screw cap (Fig. 1). The plastic container was filled with 0.9% NaCL solution, and the apical and middle thirds of the tooth were inserted into it. The tooth was irrigated with 2.5% NaOCl, and EWL was calculated in the experimental settings described above. The file tip with the previously calculated length was inserted into the tooth, and the file clip was attached. The file was pushed beyond the 0 reading on the EAL display and withdrawn slightly until the 0 reading was displayed indicating apical patency. This reading was confirmed by the audible signal emitted from the EAL. The file stop was adjusted, and this length was recorded as EWL. A total of 945 measurements were recorded and tabulated, and results were compared for statistical significance. To determine the stability of EWL reading, the following scores were used: 1. Immediate and clear audible signal emitted from EAL for a period of 5 seconds 2. Audible signal emitted from EAL for a period of 5 seconds but after 1 attempt 3. Audible signal emitted from EAL for a period of 5 seconds but after 2 attempts Background noise (sign of interference) between the devices was also noted. Statistical Analysis Data were analyzed by using two-way repeated-measures analysis of variance followed by Bonferroni multiple post hoc procedure. The statistical significance was set at 5% level of significance (P < .05). All the experiments were performed in the same place to ensure accurate replication of the results. Length Determination under Microscope After access opening and verification of canal patency, #10 K-file (Mani Inc, Tokyo, Japan) was used to prepare the glide path. Pulp tissue was removed from the canal by using #10 K-file and 2.6% NaOCl. A #15 file (Mani Inc) fitted with a rubber stop was inserted into the canal until JOE — Volume 42, Number 4, April 2016 Figure 1. Experimental model connected to the electronic apex locator with cellular phone placed in physical contact with the electronic apex locator. Cellular Phones and Apex Locators 623 Basic Research—Technology TABLE 1. Mean Values of Working Length for Each Condition 15.3 1.1 Cell phone in different conditions No phone Mobile phone in standby Mobile phone ringing Mobile phone at a distance of 40 cm Mobile phone ringing at distance of 40 cm Cell phone in different conditions No phone Mobile phone in standby Mobile phone ringing Mobile phone at a distance of 40 cm Mobile phone ringing at distance of 40 cm Working length under microscope Working length measured by using Propex II apex locator Working length measured by using Rootor apex locator Closed room 14.9 0.95 14.9 0.98 14.9 1.07 14.9 1.07 14.9 1.07 Closed room 14.8 1.01 14.8 1.03 14.8 1.03 14.8 1.03 14.8 1.03 Polyclinic 14.9 0.95 14.9 0.98 14.9 1.07 14.9 1.07 14.9 1.07 Polyclinic 14.8 1.01 14.7 1.03 14.7 1.03 14.7 1.03 14.7 1.03 EMI between cellular phones and medical devices generally occurs only when the cellular phones are in proximity to the medical devices (18). The results of this study show that there is no correlation between cellular phone use and EWL determination. Under all the experimental conditions the EAL showed good reliability and stability. This study concluded that presence of cellular phone in close proximity or at a distance from the EAL does not influence the readings of EALs. Thus, cellular phones can be used in a dental operatory during root canal therapy without the risk of EMI between cellular phone and EAL. In vitro studies have used alginate, agar agar, gelatin, and saline to simulate the root surrounding tissues in EWL determination (19, 20). Therefore, saline was used as electroconductive material in this study. Teeth were horizontally sectioned at the cementoenamel junction for obtaining reproducible reference points and were mounted in a plastic container filled with 0.9% NaCl until the root was soaked in the solution. Irrigants are used in endodontics for their antimicrobial, tissue dissolving, and lubrication properties. Studies have shown that NaOCl can be safely used with EALs in working length determination (21). Hence, 2.5% NaOCl was used as a canal irrigant in this study. Previous studies have reported that Propex II and Rootor can accurately locate the major foramen (20, 22), which is similar to the findings in our study. Different experimental settings were used in this study. In experimental setting 1, Wi-Fi, GPRS, and Bluetooth networks were inactivated to prevent any electronic interference. The experiment was carried out in a closed room to prevent interference from other cellular phones. Furthermore, a room with poor signal strength was selected to induce the mobile phone to transmit at maximum power, thus increasing the risk of EMI because cellular phones control output power depending on the availability of the nearest cell base station (23). Experiment 2 was conducted in a polyclinic with good signal strength where Wi-Fi, GPRS, and Bluetooth networks were activated, and the dental personnel carried cellular phones, mimicking a dental operatory in a realistic scenario. Because the distance between 2 electronic devices can influence EMI (16, 24), different distances between the cellular phone and the EAL were tested in this study. The recommended safety distance between a cellular phone and medical device for a Global System for Mobile Communication (GSM) 900 MHz cellular phone is 70 cm, for a GSM 1800 MHz cellular phone the safety distance is 5 cm (16), whereas for GPRS cellular phones, a safety distance of 1 m is recommended between the cellular phones and medical devices (25). Samsung Galaxy Note Edge can be considered a GSM 900 MHz multiband phone and can transmit network frequencies of 900 MHz and 1800 MHz. Also for the present study, GPRS was activated with the existing GSM network. Because the ideal distance between a dental operator and a patient is similar to that of reading a book (26), a distance of 40 cm between the apex locators and the cellular phone was used in this study. Because the wave emission is intense during the calling mode of the cellular phone (17), the calling mode was used to maximize the chances of detecting EMI. The interference between cardiac pacemakers and cellular phones is not time-dependent. A stimulus either does or does not interfere with the pacemaker (27). Therefore, a stimulus of 25 seconds (phone in calling mode) was deemed satisfactory for the purpose of this study. According to Gomez et al (28), EALs can interfere with the activity of pacemakers if the EAL is placed close to the tip of the pacemaker TABLE 2. Two-way Repeated Analysis of Variance (tests of within-subjects effects) for Propex II EAL TABLE 3. Two-way Repeated Analysis of Variance (tests of within-subjects effects) for Rootor EAL Type III Partial sum of Mean F P eta squares df square value value squared Type III Partial sum of Mean F P eta squares df square value value squared Results Three readings were taken for each tooth, and averages of the readings were tabulated and compared for mean and standard deviation under the different conditions. It was found that in a closed room among the different apex locators, there is no significant change in measurement of readings when compared with mobile phone in different conditions (P > .05). However, there is a minimal change in measurement when the tests were performed in a polyclinic setting with Rootor EAL. There is no significant change in Propex II EAL in both closed room and polyclinic (P > .05) (Table 1). No statistically significant differences were recorded between the different groups (Tables 2 and 3) Under all the experimental conditions, the EAL readings were stable (none scored 2 and 3 on the 945 EWL measurements), and no background noise was detected between the 2 electronic devices. Discussion Source Groups Time Groups * Time 0.00 0.01 0.00 1 5 5 0.00 0.00 0.00 *Comparison of the interactions of groups and time points. 624 Sidhu et al. — — 1.0000 .4240 — — — 0.0670 — Source Groups Time Groups * Time 0.00 0.01 0.00 1 5 5 0.00 0.00 0.00 — — 1.0000 .4240 — — — 0.0670 — *Comparison of the interactions of groups and time points. JOE — Volume 42, Number 4, April 2016 Basic Research—Technology electrode. This may also explain the absence of EMI between cellular phones and EALs (17). Also, the findings of this study do not support the claim in the user manuals of EALs that EMI from portable and mobile radiofrequency communications equipment such as cellular phones can cause interference with accurate reading of the apex locator. Conclusion The present study revealed that EWL determination by apex locators is not influenced by the presence of cellular phones. Cellular phones can be used in the dental operatory without the fear of causing EMI in EWL determination during root canal therapy. Further in vitro and in vivo studies with different parameters may be beneficial to confirm the results of the present study. Acknowledgments The authors deny any conflicts of interest related to this study. References 1. Kim E, Lee SJ. Electronic apex locator. Dent Clin North Am 2004;48:35–54. 2. Kim E, Marmo M, Lee CY, et al. An in vivo comparison of working length determination by only root-ZX apex locator versus combining root-ZX apex locator with radiographs using a new impression technique. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;105:e79–83. 3. Gordon MP, Chandler NP. Electronic apex locators. Int Endod J 2004;37:425–37. 4. Khursheed I, Bansal R, Bansal T, et al. A comparative evaluation of working length with digital radiography and third generation apex locator (ProPex) in the presence of various intra canal irrigants: an in vivo/ex vivo study. Dent Res J (Isfahan) 2014; 11:56–60. 5. Akisue E, Gavini G, de Figueiredo JA. Influence of pulp vitality on length determination by using the Elements Diagnostic Unit and Apex Locator. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;104:e129–32. 6. Singh SV, Nikhil V, Singh AV, et al. An in vivo comparative evaluation to determine the accuracy of working length between radiographic and electronic apex locators. Indian J Dent Res 2012;23:359–62. 7. Ebrahim AK, Wadachi R, Suda H. In vitro evaluation of the accuracy of five different electronic apex locators for determining the working length of endodontically retreated teeth. Aust Endod J 2007;33:7–12. 8. Hayes DL, Wang PJ, Reynolds DW, et al. Interference with cardiac pacemakers by cellular telephones. N Engl J Med 1997;336:1473–9. 9. Patel MB, Thaker JP, Punnam S, et al. Pacemaker interference with an iPod. Heart Rhythm 2007;4:781–4. JOE — Volume 42, Number 4, April 2016 10. Miller CS, Leonelli FM, Latham E. Selective interference with pacemaker activity by electrical dental devices. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998; 85:33–6. 11. Madigan JD, Choudhri AF, Chen J, et al. Surgical management of the patient with an implanted cardiac device: implications of electromagnetic interference. Ann Surg 1999;230:639–47. 12. Tandogan I, Temizhan A, Yetkin E, et al. The effects of mobile phones on pacemaker function. Int J Cardiol 2005;103:51–8. 13. Trigano JA. Interferences and cardiac pacemakers-defibrillators: results of in vivo experiments and radio frequencies. Arch Mal Coeur Vaiss 2003; 96(Spec No 3):42–5. 14. Baranchuk A, Kang J, Shaw C, et al. Electromagnetic interference of communication devices on ECG machines. Clin Cardiol 2009;32:588–92. 15. Lawrentschuk N, Bolton DM. Mobile phone interference with medical equipment and its clinical relevance: a systematic review. Med J Aust 2004;181:145–9. 16. Hietanen M, Sibakov V. Electromagnetic interference from GSM and TETRA phones with life-support medical devices. Ann Ist Super Sanita 2007;43:204–7. 17. Hurstel J, Guivarc’h M, Pommel L, et al. Do cell phones affect establishing electronic working length? J Endod 2015;41:943–6. 18. Klein AA, Djaiani GN. Mobile phones in the hospitals: past, present and future. Anaesthesia 2003;58:353–7. 19. Barthelemy J, Gregor L, Krejci I, et al. Accuracy of electronic apex locatercontrolled handpieces. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;107:437–41. 20. Altunbas D, Kustarci A, Arslan D, et al. Comparison of various current electronic apex locators to determine the working length using the clearing technique. Niger J Clin Pract 2015;18:359–63. 21. Duran-Sindreu F, Gomes S, St€ober E, et al. In vivo evaluation of the iPex and Root ZX electronic apex locators using various irrigants. Int Endod J 2013;46:769–74. 22. Chakravarthy Pishipati KV. An in vitro comparison of propex ii apex locator to standard radiographic method. Iran Endod J 2013;8:114–7. 23. Van Lieshout EJ, van der Veer SN, Hensbroek R, et al. Interference by newgeneration mobile phones on critical care medical equipment. Crit Care 2007; 11:R98. 24. Garofalo RR, Ede EN, Dorn SO, et al. Effect of electronic apex locators on cardiac pacemaker function. J Endod 2002;28:831–3. 25. Wallin MK, Marve T, Hakansson PK. Modern wireless telecommunication technologies and their electromagnetic compatibility with life-supporting equipment. Anesth Analg 2005;101:1393–400. 26. Theodore MR, Herald OH, Edward JS. Sturdevant’s Art and Science of Operative Dentistry, 4th ed. St Louis, MO: Mosby Inc; 2002. 27. Sriman N, Prabhakar V, Bhuvaneswaran JS, et al. Interference of apex locator, pulp tester and diathermy on pacemaker function. J Conserv Dent 2015;18:15–9. 28. Gomez G, Duran-Sindreu F, Jara Clemente F, et al. The effects of six electronic apex locators on pacemaker function: an in vitro study. Int Endod J 2013;46:399–405. Cellular Phones and Apex Locators 625