Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Drug discovery wikipedia , lookup
Prescription costs wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Prescription drug prices in the United States wikipedia , lookup
Compounding wikipedia , lookup
Pharmacogenomics wikipedia , lookup
List of off-label promotion pharmaceutical settlements wikipedia , lookup
Margaret M Dotzel
(202) 778-1998
mdotzel@zuckerman,com
April 23, 2009
Division of Dockets Management
Food and Drug Administration
5630 Fishers Lane, Room 1061
Rockville, MD 20852
Re: Comments to King Citizen Petition Docket No. 2009P-0040
Dear Sir or Madam:
I am writing on behalf of Sun Pharmaceutical Industries Limited to respond to King
Pharmaceuticals, Inc. January 29, 2009 citizen petition.
Introduction
In December 2007, Sun Pharmaceutical Industries Limited (hereinafter referred to as "the
Applicant") filed an ANDA application for surnatriptan succinate injection referencing
Glaxo Smith Kline’s (GSK’s) Imitrex STATDose® Injection. Both the drug portion
(sumatriptan succinate) of the combination product and its labeling are the same. In
addition, the performance of the autoinjector device in the GSK product and the
autoinjector device in the Applicant’s product are similar and meet applicable FDA
standards, although certain aspects of the Applicant’s device that are not related to
performance are not identical to the GSK device. Importantly, the Applicant has
demonstrated that its product is bioequivalent to the GSK product. As discussed below,
the differences between the two products are both beneficial and in one important respect
necessary to meet current ISO standards that have been recognized by FDA.
On January 29, 2009, King (the maker of several autoinjector products) filed a citizen
petition requesting FDA to confirm that any ANDA application for sumatriptan succinate
injection containing an autoinjector is only eligible for approval if the autoinjector is
identical to the reference product’s autoinjector in performance, physical characteristics,
and labeled instructions. King argues that an autoinjector that is not identical will
adversely affect public health because of the risk of confusion and improper use of the
substituted product. King further asks FDA to clarify drug nomenclature to ensure
consistent identification of dosage form, route of administration, and strength for all drug
products containing sumatriptan. King’s 2009 citizen petition refers to an earlier citizen
petition that King filed on Sep 26, 2007, which is pending at the Agency. In the 2007
petition, King requests that FDA 1. Decline to approve or stay the approval of any ANDA submitted under section
505(j) that references a drug product containing an autoinjector as the listed drug,
unless it has been demonstrated that the proposed autoinjector is the "same" as the
autoinjector in the Reference Listed Drug ("RLD");
2. Refuse to designate any drug product containing an autoinjector approved under
sections 505(b) or 505(j) as therapeutically equivalent to an RLD containing an
autoinjector, unless it has been demonstrated that the autoinjector is
pharmaceutically equivalent to, bioequivalent to, and has the same labeling as the
autoinjector contained in the RLD; and
3. Require that sponsors of new drug products containing autoinjectors conduct
appropriate clinical studies in patients under the conditions for which the
autoinjector is indicated if: (i) the sponsor files a section 505(b)(2) application or
an application pursuant to a suitability petition, and (ii) the autoinjector is not the
"same" as the autoinjector in the RLD.
The Applicant does not object to FDA clarifying drug nomenclature to ensure consistent
identification of dosage forrn, route of administration, and strength for all drug products
containing sumatriptan, but since such clarification is not a prerequisite to approval of a
generic sumatriptan injector, any time necessary to issue such a clarification may not
delay approval of Applicant’s product. More importantly, there is no legal basis for
King’s claim that the Applicant’s autoinjector must be identical to the reference drug’s
autoinjector, particularly since the autoinjector utilized in Applicant’s product already has
been cleared by FDA and such autoinjector is in fact safer than the reference drug
product’s autoinjector in that it includes additional safety features that are required by the
FDA adopted consensus standards used to clear such device. In fact, King’s argument, if
accepted, would mean that applicants for approval of combination drug-device products
would be prohibited from meeting consensus standards recognized between approval of
the reference product and submission of an abbreviated new drug application. If King
were correct, then the device feature of combination products would be frozen in place at
the time the reference product is approved and FDA could not encourage or even permit
improvements that advance the public health. Theretbre, FDA should deny the King
petition and proceed immediately to approve the Applicant’s ANDA. In addition, FDA
should find that the petitioner has failed to demonstrate that delay in approval of the
Applicant’s ANDA is necessary to protect the public health under Section 505(q) of the
FDC Act.
Background
The generic injectable sumatriptan product, which is the subject of the Applicant’s
ANDA, is a combination product that contains both a drug (sumatriptan succinate) and a
device (the autoinjector). The reference listed drug (RLD) is GSK’s Imitrex
STATDose® Injection.
2
The drug portion of the Applicant’s product is identical to the RLD. Both products
contain 6.0mg/0.5 ml of sumatriptan succinate for injection. The Applicant has data
demonstrating that its product is both qualitatively and quantatively similar to the
reference drug and therefore qualifies fbr a waiver of traditional bioequivalence studies.
The Applicant’s drug labeling is the same as the labeling of the reference drug2.
The Applicant’s sumatriptan device is pre-filled with the drug. It is a needle based,
spring loaded, plunger (piston) drive injector. It is disposable, self injectable, pen shaped
and portable, it has a safety cover to limit needle exposure, a click at the beginning of the
injection and a second click at the end. The injector has an inspection window for drug
delivery confirmation. It also has safety features that prevent accidental firing of the
device and needle stick injuries.
The device used in the Applicant’s product has been cleared by FDA pursuant to a 510(k)
notification (510(k) clearance number K050434), which was based on comparative data
submitted to FDA. FDA issued an order finding the device to be substantially equivalent
to Owen Mumford Autoject Mini (510(k) Clearance Number: K000482) and eligible to
be marketed in United States. A 510(k) is a premarket submission made to FDA to
demonstrate that the device to be marketed is at least as safe and effective as, that is,
substantially equivalent to, a legally marketed device (21 C.F.R. § 807.81) that is not
subject to premarket approval. Submitters are required to compare their device to one or
more similar legally marketed devices and to make and to support their substantial
equivalency claims. A 510(k) requires demonstration of substantial equivalence to the
legally marketed device, which is referred to as the "predicate." Section 513(i) of the
FDC Act provides that a device is substantially equivalent in comparison to a predicate if
it¯
¯
has the same intended use as the predicate, and
has the same technological characteristics as the predicate;
or
¯ has the same intended use as the predicate, and
¯ has different technological characteristics and the information submitted to
FDA both;
o does not raise new questions of safety and effectiveness; and
1 Nevertheless, the Applicant has performed traditional bioequivalence studies, which it will submit to FDA
upon request.
2 The Applicant’s label is similar to the label of the RLD in all aspects, except that, unlike the RLD label,
the Applicant’s label does not include instructions on assembly and disassembly of the device. The reason
this inlbrmation is excluded is because the Applicant’s device requires no assembly. Thus, the device is
actually easier to use because it has fewer instructions for the patient, as compared to the device of the
RLD. The remaining steps for the Applicant’s device are similar to those in the RLD device, and hence,
the Applicant’s label is in fact similar to the RLD label.
demonstrates that the device is at least as safe and effective as the legally
marketed device.
See also 21 C.F.R. § 807.100(b). In order to demonstrate substantial equivalence, the
device sponsor does not need to demonstrate that the new and predicate devices are
identical. Instead substantial equivalence is established by showing that even if there are
differences, the new device is as safe and effective as the predicate device and
specifically that the device "[d]oes not raise different questions of safety and
effectiveness than the predicate device." 21 C.F.R. § 807.100(b).
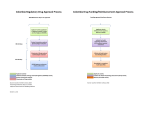
The device used in the Applicant’s ANDA product was assessed using the sections and
methods specified in ISO 11608:2000 "Pen injectorsJbr medical use - Part I : Pen
injectors - Requirements and test methods" as they apply to injection devices with nonreplaceable prefilled cartridges. This ISO standard is an FDA-recognized consensus
standard and therefore can be used to support a showing of safety and effectiveness.
Activation force, needle extension, injection time, completeness of injection,
functionality, and robustness were assessed; the device met all requirements and
specifications provided in ISO 11608:2000.
The International Standard ISO 11608:2000 relates to requirements and test methods for
pen-injectors intended for human use, for evaluating drug products contained in
autoinjectors. This ISO standard provides performance requirements regarding essential
aspects, so that variations of design are not unnecessarily restricted. Particularly, it
includes ¯ When the pen-injector is ready for injection, the cartridge holder shall allow
visibility of the deliverable volume. It shall be possible to determine whether
sufficient medicinal product remains in order to administer the maximum presettable dose.
¯ The pen-injector shall be designed such that it is able to deliver the labeled
volume from the cartridge for which it is designed.
¯ The pen-injector shall indicate the pre-set dose.
¯ The pen-injector shall indicate, at least by visual means, that it is ready for
injection. There shall be an indication of the pre-setting procedure by tactile or
audible means, or both.
¯ The state of the pen-injector, when ready to deliver a dose, shall be different to
its state when the dose has been delivered. The difference shall be visible.
¯ The pen-injector shall indicate, by visual, audible or tactile means or any
combination of these, that the injection stroke has been completed.
Design and performance features of the autoinjector device used in the ANDA product
meets these standards. In addition, the device includes a safety mechanism to prevent
inadvertent activation, a needle-cover that extends to cover the used needle, a cutout
window on the front assembly to permit inspection of the syringe, locking tabs to prevent
disassembly of the autoinjector once the two subassemblies have been connected, and
4
self-disabling after use. The autoinjector device used in the ANDA product is currently
marketed in the USA under the trade name SureClickTM. SureClickTM is being used by
Amgen fi~r its Aranesp® and Enbrel® products, which have been approved by FDA and
for which tens of millions of doses have been delivered to U.S. patients.
The Applicant’s device delivers the same amount of drug in the same arnount of time as
the reference product. In addition, the Applicant’s product is delivered exactly the same
as the brand - by pushing against the body and pressing a blue button. The only
differences between the Applicant’s device and the brand device are that
¯
¯
¯
The Applicant’s product requires no preassembly of the syringe while the brand
does;
The Applicant’s product has safety features that prevent accidental firing and
needlestick injuries; and
The Applicant’s product has a window that shows that the drug has been
dispensed, while the brand does not. The window also allows inspection of the
injectible solution tbr presence of any particulate matter, prior to injection.
The differences in the Applicant’s device make it safer than the brand in that there is less
risk of needle stick injury, less risk that the patient will think drug has been dispensed
when it has not, and less risk that the patient will accidentally trigger the mechanism.
Analysis
The Jbundation of the King petition is" that there is" a requirement in the law that the
device in a generic combination product must be identical to the device in the brand
combination product and that the labeling for the device must also be identical. There is,
however, no such requirement in the Federal Food Drug and Cosmetic Act (FDC AcO.
This is fortunate because, with respect to the Applicant’s autoinjector product, imposing
such a requirement would deprive consumers of both a less expensive generic version of
the product and one that is easier and safer to use.
1. The generic drug provisions of the FDC Act do not require the Applicant to use the
identical autoinjector in its" combination product.
King’s petition provides no statutory or regulatory authority for the proposition that the
device portion of a combination product must be identical to the device portion of the
reference product. Moreover, FDA has explicitly stated in guidance, that the device
portion of a combination product need not be identical to the device portion of the
reference listed drug. In a guidance on nasal aerosols and nasal sprays, FDA states that
although assurance of bioequivalence is greatest when the generic uses the same brand
and model device as the brand, if this is infeasible then FDA recommends that the
designs be as close as possible to the critical dimensions of those of the reference.
Guidance for Industry, Bioavailability and Bioequivalence Studies for Nasal Aerosols
and Nasal Sprays for Local Action (April 2003).3 It is important to note that in the
context of nasal aerosols, the design of the device is critical to assuring that the same
amount of the drug is being delivered because it affects factors such as droplet size,
plume geornetry, and spray pattern. As set forth below, the Applicant has demonstrated
that the same amount of sumatriptan is delivered with its autoinjector and King has not
even raised much less refuted that fact.
King also argues that FDA should issue guidance describing the circumstances under
which a drug containing an autoinjector may be approved under an ANDA. King
speculates that the absence of FDA guidance on autoinjectors may reflect an internal
conclusion by the Agency that the ANDA pathway is not suitable for products containing
autoinjectors. There is absolutely no statutory mandate that FDA must issue a guidance
before approving a particular combination product and King has no basis for claiming
that the absence of a guidance suggests that the Agency has concluded that the ANDA
route is not appropriate for the applicant’s product. There is nothing in FDA’s
regulations or guidance to imply that this would be FDA’s position.
2. Comparative tests" have demonstrated that the Applicant’s combination product is
bioequivalent and has the same perjbrmance as the Imitrex STATDose®.
In the 2007 Citizen Petition, King states in Sec 2.1.1 that "an auto-injector should not be
approved as pharmaceutically equivalent to another auto-injector, and should not be
approved under an ANDA, unless the two auto-injectors are demonstrated to deliver
identical amounts of the active ingredients in an identical dispensing time based on
comparative performance testing of the auto-injectors." The Applicant performed tests to
compare its device with the STATDose® device of Glaxo’s hnitrex injection product for
deliverable volume and dispensing time. These tests showed that, pursuant to the
standard advocated by King, the autoinjector device used in the Applicant’s product is
equivalent to the autoinjector used in the reference product. The Applicant also
compared the following with Imitrex STATDose® ¯
¯
¯
¯
¯
¯
¯
¯
Stability
Drop tests results (from 1.5m height, on various surfaces)
Excessive force on device test
Shield remover removal force
Needle cover pre-injection force
Actuator button safety force
Activation force
Injection time
Injection depth
The Applicant’s autoinjector device is similar to the reference product because
3 In fact, FDA approved a generic fluticasone propionate nasal spray that has a device that has a safety clip
feature that is not included in the brand reference product device.
¯
¯
¯
¯
¯
¯
¯
The final delivery steps are same ("Press against the injection site and
press the blue button.");
The device delivers same volume of drug (0.5 ml);
The depth of needle penetration is the same (4-7 mm);
The delivery time is similar ( 1-2 seconds);
The forces required to operate the device are similar;
The colors are similar; and
The safety features both products have are the same (although as discussed
herein, the Applicant’s product has additional safety features).
As stated above, the Applicant has also complied with FDA’s bioequivalence
requirements by demonstrating that its sumatriptan succinate injection product is both
qualitatively and quantitatively similar to that of the GSK product.
This showing of performance equivalence of the device used in the Applicant’s product is
sufficient to establish that the device is at least as safe as the device of the reference
product. An ANDA pathway requires that the ANDA product meets the "sameness"
criteria, and hence data establishing performance equivalence of the devices is sufficient
to meet this "sameness" requirement.
The Applicant has demonstrated that its device and Glaxo’s device do not differ in
releasing the drug into the systemic circulation of the patient. The delivery of the drug to
the patient is comparable, both in terms of volume delivered and in terms of the
bioavailability of the drug, because the Applicant has demonstrated that sumatriptan
injection and Imitrex STATDose® are bioequivalent.
King’s own experience with an epinephrine autoinjector products supports approval of
the Applicant’s ANDA. Prior to the time it was available in an autoinjector product,
epinephrine was available in ampuls. King obtained approval for the Epipen autoinjector
on the basis of an application that did not contain any preclinical, clinical or
bioequivalence studies. Similarly, Twinject, another epinephrine autoinjector product,
was approved without any such studies. King’s argument that clinical studies must be
required in order to resolve safety issues raised by the Applicant’s product is entirely
inconsistent with its application for the Epipen and with the Agency’s approval of that
application.
In section 2.1.2 of the 2007 Citizen Petition, King states that "FDA should establish new
auto-injector dosage forms that distinguish among auto-injectors with significant
differences in administration and physical appearance as well as distinguish autoinjectors from other injectable dosage forms." King further states that "differences
among auto-injector release mechanisms would satisfy criteria under 21 C.F.R.
§ 314.127(a)(8) for refusing to approve an ANDA because ’there is a reasonable basis to
conclude that one or more of the inactive ingredients of the proposed drug or its
composition raises serious questions of safety or efficacy’" King cites 21 C.F.R.
§ 314.127(a)(8)(ii)(A)(2),(3), (5), and (6) and FDA’s Abbreviated New Drug
Applications regulations at 57 Fed. Reg. 17950, 17969 (Apr 28, 1992), to argue that
changes in release mechanism are comparable to other changes in inactive ingredients for
the purpose of 21 C.F.R. § 314.127(a)(8).
The obvious response to King’s argument is that the autoinjector component of the
Applicant’s product is not an inactive ingredient, and there is nothing in the statute or
regulations to suggest that it is. But even if the autoinjector component were somehow
considered to be an inactive ingredient, then the applicant has met all the requirement of
the statute and regulations. For example, section 505(j)(4)(H) of the FDC Act provides
that one basis for disapproving an ANDA is "information [which] shows that.., the
inactive ingredients of the drug axe unsafe." Of course, if the information provided to
FDA shows that the inactive ingredients are safe, as is the case here, then FDA must
approve the generic product.
The FDA regulations and Federal Register notice cited by King are entirely consistent
with the statute. Thus, 21 C.F.R.§ 314.127(a)(ii)(A) identifies situations where the
inactive ingredient will be found to be unsafe, including where the inactive ingredient
"does not comply with an official compendium," "a change in composition to include an
inactive ingredient that has not been previously approved in a drug product for human use
by the same route of administration," changes to include inactive ingredients that have
not been previously approved in the dosage form proposed by the ANDA applicant or the
use of inactive ingredients at levels not previously approved or in a way that might
increase absorption of toxic ingredients, and the "use of a delivery or modified delivery
mechanism never before approved for the drug." The Federal Register preamble cited by
King restates some of these same criteria. Although one would have to stretch beyond
recognition the meaning of inactive ingredient to include an autoinjector device, the
principles in the regulation on which King relies support approval of the Applicant’s
ANDA. In contrast to the situations identified in the regulations, which would be the
basis for a safety concern, the device component in the Applicant’s product has
previously been approved by FDA and it will deliver the active drug to the body at the
same rate as the reference listed drug. Thus if King were correct that the autoinjector is
an inactive ingredient, then under King’s argument the mere fact that the Applicant’s
autoinjector has minor differences from the device component of the RLD would not be a
basis for denying the ANDA.
In Sec 2.3 of the 2007 citizen petition, King states that an in-vivo bioequivalence waiver
should apply to drug products containing auto-injectors only in the presence of "other
data" in the form of comparative performance testing. According to King, such testing
should show that the auto-injector used in a proposed drug product will (i) deliver the
same amount of drug (ii) to the same area (iii) in the same amount of time (iv) with the
same force (v) under similar conditions. King, for once, cites an applicable requirement,
which is in line with requirements set forth in the ISO 11608:2000 standard and used by
the FDA to clear 510(k) premarket notifications. Where the ANDA applicant can
establish performance equivalence to the device of the reference product, the ANDA
8
product may be approved without the requirements of clinical testing, particularly if the
drug contained in the autoinjector device is a parenteral solution that is qualitatively and
quantitatively similar to that contained in the reference product.
3. Requiring the Applicant to use the identical autoinjector would be requiring use of an
autoinjector that does not meet ISO standards" that FDA has" recognized, is more difficult
to use than Sun % injector, and lacks" certain saJ~ty features.
Section 514(c) of the FDC Act gives manufacturers explicit authority to use FDArecognized standards to meet the requirements of the act.4 It directs FDA to recognize
national and international standards by publication in the Federal Register and allows
manufacturers, if they elect to conform to any of these standards, to submit a declaration
of conformity to FDA or a statement of conformity to FDA.
When FDA cleared the autoinjector included in the Applicant’s combination product, it
relied on such a recognized ISO standard. If FDA were to accept King’s argument and
require the Applicant to use the autoinjector device in Glaxo’s product, then the device
would no longer meet that recognized standard because the autoinjector device used in
the reference product, Glaxo’s Imitrex STATDose®, does not meet all of the
requirements set forth in the ISO 11608:2000. Specifically, the Glaxo device does not
have a cutout window to permit inspection of the syringe prior to injection. Substitution
of the autoinjector device of the reference product with the improved autoinjector device
ensures that safer and easy-to-use devices are made available to the patient. While we are
not suggesting that the failure of the Glaxo device to meet ISO requirements would be a
basis for withdrawing the product from the market, FDA’s policy should encourage
applicants to improve device products as new materials and techniques become available;
it surely should not prohibit the adoption of such improvements which would be the
effective result of accepting King’s arguments.
The Applicant’s autoinjector device is safer than the autoinjector device in Glaxo’s
reference product in other respects as well. The advantages include ¯
¯
The risk of needle stick injuries and needle phobia is reduced in the device, since
the needle is not visible to the user and the needle is never left uncovered (the
needle cover automatically locks in its extended position after injection in the
device). In the Glaxo device, after the injection, the needle is visible and there is a
risk of needle stick injury.
The device is a single-use disposable device, and hence eliminates the risk of
malfunction that may arise upon multiple-use, as well as the confusion associated
with the same. For example, in the Glaxo device there is a risk that user may load
the used syringe again.
4 See also, Guidance for Industry and for FDA Staff: Use of Standards in Substantial Equivalence
Determinations (March 2000).
The device is convenient for the user since it eliminates the preparation and
disposal steps associated with the Glaxo device. As a result, the training time, as
well as the time required to dispense and administer the injection is significantly
less for the device.
These improved safety features are a result of the improved design of the Applicant’s
autoinjector device.
King does not dispute that the patient will benefit from a better device that is equivalent
in performance to the device of the reference product. Yet its claim that an ANDA
applicant must use an "identical" device, if accepted, would deny the patient the benefits
associated with the improved devices. In fact, the Applicant’s autoinjector device is a
safer and better alternative to the Glaxo autoinjector device, which falls below current
ISO standards.
Since a generic combination product is developed much later than the reference product,
it should have the benefit of being able to use a newer and improved autoinjector device,
which has advantages and conveniences. Accepting King’s petition would freeze
technology in place, force generic manufacturers of combination products to copy
outmoded device components, and deny patients better alternatives that are a result of
research into developing user-friendly, safer, convenient and cost-effective autoinjector
devices.
4. The labeling on the autoinjector used in the Applicant % sumatriptan succinate
product meets" the FDA-recognized ISO standards" requiring clear instruction of patients
and is" consistent with safe use of the product by patients.
In Section 1.4 of the 2007 citizen petition, entitled "Substitution of Auto-Injectors is
Potentially Unsafe", King argues that patients will not read the labeling of a substituted
autoinjector product and will use it improperly. Section 2.2 of the 2007 petition argues
that FDA’s labeling regulations do not permit differences in operating instructions or
graphic illustrations.
As set forth above, FDA has permitted the device portion of a combination device to be
different from the reference product. For example, a generic fluticasone nasal spray
product was approved although the device used in the generic product is different from
that of the reference product in that it has a safety clip, and the label for the generic has
illustrations and instructions that are different from the label of the reference product.
Thus, FDA does permit differences in the device portion of the labeling to account for
these differences. King’s concerns on improper use of the Applicant’s sumatriptan
injection are therefore unfounded. In addition, as described below, the Applicant’s
inserts meet the ISO standards. Moreover, a pharmacist dispensing the Applicant’s
sumatriptan injection would provide demonstration and explanation on the use of the
device to the patient, as necessary. These careful instructions by the pharmacist assure
10
that the patient will use the device in the proper manner suggested in the Applicant’s
package insert, and thus remove any risks associated with the improper use.
The ISO standard applicable to the autoinjector, ISO 11608.2000, requires clear
instructions to the patient on how to use the device. Specifically, the standard includes
requirements regarding information to be provided by the manufacturer, and states that
the pen-injector shall be accompanied by sufficient information to use it safely, taking
into account the training and knowledge of the potential users. Section 15.3 of this
standard provides requirements related to instructions for use. These requirements relate
to instructions to be included in the package insert, and require inclusion of, among
others, the following particulars ¯ any warnings and/or precautions to be taken
¯ any risks associated with its normal use
¯ sufficient details of its characteristics to identify the pen-injector and related
equipment in order to obtain a safe combination
¯ details on any preparation needed before the pen-injector can be used, e.g. the need to prime before each injection, how to assemble/disassemble the
product, replace the cartridge and attach the needle
¯ description of the method of use, e.g. the injection procedure as step-by-step
operations
¯ time to wait before removing the needle from the injection site
¯ description of special features
¯ details allowing the medical staff to brief the user on any contraindications
and any precautions to be taken.
The package insert accompanying the Applicant’s sumatriptan injection provides detailed
and pictorial description on use of the device, as required under ISO 11608:2000.
The issue raised by King is whether the patient will be given, and can properly receive
training when a generic product having a different autoinjector device is dispensed by a
healthcare professional or a pharmacist. In the dispensation of medications, the
dispensing healthcare professionals are known to exercise due care. In the case of the
Applicant’s product, the autoinjector component is already on the market, and thus
pharmacists and healthcare professionals will already be familiar with it and how to
instruct patients on the products’ use. initial training is provided to the patient to ensure
that he or she can use the alternate autoinjector device as required. The patient can also
exercise his or her choice for the reference product. However, if the patient is
comfortable with the generic product, which has the same performance, and if the patient
is comfortable that he or she can learn how to use the generic product, then the patient
should not be denied access to a more affordable, safer generic product. As mentioned
above, the ISO standard requires that the package insert for the proposed device include
instructions for use of the device that may be used by the healthcare professional to
provide training to the patient. Hence, the graphic/pictorial illustrations and the written
description on the steps to use the device would ensure that the healthcare professional
11
would provide the necessary training, and thereby address any contusion that King
alleges may arise.
5. King hasJktiled to show that delay of approval of the Applicant’s ANDA is"
necessary to protect the public health.
Section 505(q) of the FDC Act provides that FDA shall not delay approval of a pending
ANDA application because of any request in a citizen petition to take any form of action
relating to the application, either before or during consideration of the request, unless the
requested delay is necessary to protect the public health. Because King is effectively
arguing that FDA should require the use of an autoinjector that falls below ISO consensus
standards and lacks certain safety features, there is no basis to conclude that FDA should
delay approval of the Applicant’s ANDA because such delay is necessary to protect the
public health. In fact, in the unusual circumstances of the Applicant’s ANDA, such a
delay would be inconsistent with the public health.
Conclusion
Contrary to King’s arguments, nothing in the law requires the autoinjector in the
Applicant’s generic combination product to be identical to the reference drug’s
autoinjector. In tact, if, as King argues, FDA must require an ANDA applicant to use an
autoinjector that is identical to the one used in GSK’s product, it in effect would be
requiring use of an autoinjector that does not meet ISO standards that were adopted by
Agency. The autoinjector in the Applicant’s product has been cleared by FDA and is
safer than the reference drug product’s autoinjector. FDA should promptly deny the King
petitions and proceed to approve the Applicant’s ANDA. In any event, FDA should
reach a decision within 180 days of January 29, 2009, the date King filed its citizens
petition, as required by section 505(q) of the FDC Act.
Zuckerman Spaeder LLP
12
VERIFICATION STATEMENT UNDER 21 U.S.C. § 355(q)(1)(I)
I, Margaret M. Dotzel, certify that, to my best knowledge and belief: (a) I have
not intentionally delayed submission of this document or its contents; and (b) the
information upon which I have based the action requested herein first became known to
me on or about February 10, 2009. If I received or expect to receive payments, including
cash and other forms of consideration, fbr the time required to file this information or its
contents, I received or expect to receive those payments in the form of standard hourly
rates from the tbllowing persons or organizations: Sun Pharmaceutical Industries, Ltd.
and its affiliates. I verify under penalty of perjury that the foregoing is true and correct as
of the date of the submission of this petition.
13