Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
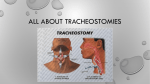
County of Santa Clara Emergency Medical Services System EMS System Policy Change Coversheet EMS SYSTEM POLICY CHANGE COVERSHEET Policy # and Title: Santa Clara County Prehospital Care Policy #700-M05: Stoma and Tracheostomy – Adult & Pediatric Date: April 2, 2015 [Change to be effective May 1, 2015] Staff Contact: David Sullivan Policy Development Unit [email protected] Background: It was determined that current policy was not aligned with current scope of practice for paramedics and EMTs. Policy initially developed for the Critical Care Transport by Paramedic program which is no longer utilized in Santa Clara County. Policy Summary and Objectives: The purpose of this policy change is to align with current scope of practice referenced in the California Health and Safety Code. The suctioning language was changed to more closely match prehospital utilization. Grammatical and formatting issues corrected. Proposed Changes: The sentence discussing tracheostomy tube replacement has been removed. The sentence discussing suctioning the bronchus while the patient turns their head has been removed. The suctioning time frame for an adult was changed from 10 seconds to a range of 5 to 7 seconds. The word hyperventilate was changed to ventilate. A note was added to the procedure section discussing tube depth. Outstanding Issues: All EMS System personnel will require notification of this policy change. Cost: No material costs anticipated. Santa Clara County Emergency Medical Services Prehospital Care Manual Page 1 of 1 County of Santa Clara Emergency Medical Services System ADMINISTRATIVE ORDER Number: 20150501-02 Title: STOMA AND TRACHEOSTOMY CARE – ADULT & PEDIATRIC Effective: May 1, 2015 Declaration The Santa Clara County Emergency Medical Services Agency has determined that revisions to Santa Clara County Prehospital Care Policy are required. Consistent with Santa Clara County Prehospital Care Policy 109 – Policy Development and Implementation; emergency changes and Administrative Orders may be issued as follows: Administrative Orders will be issued when emergency changes or immediate implementation of practices is necessary in order to ensure the protection of the publics’ health and safety. Issuance of Administrative Orders shall bypass the normal review process. Administrative Orders will be executed by the Director, and the Medical Director in matters of medical control, (if of a clinical nature) or their designee, and such orders may be made effective immediately. Administrative Orders will either be formalized into Policy or expire one year after issuance, unless terminated earlier by the Agency. Statement of Change 1. The sentence discussing tracheostomy tube replacement has been removed. 2. The sentence discussing suctioning the bronchus while the patient turns their head has been removed. 3. The suctioning time frame for an adult was changed from 10 seconds to a range of 5 to 7 seconds. 4. The word hyperventilate was changed to ventilate. 5. A note was added to the procedure section discussing tube depth. Page 2 of 2 Rationale for Change The policy is being updated to align with current scope of practice referenced in the Health and Safety Code. The suctioning language was changed to more closely match prehospital utilization. Grammatical and formatting issues corrected. Revised Documents Policy #700-M05 Stoma and Tracheostomy Care – Adult & Pediatric Questions Please direct questions to Linda Diaz, Clinical Programs Manager, at [email protected] or 408.885.4250. Execution This Administrative Order is effective as of 0001 hours on May 1, 2015. County of Santa Clara Emergency Medical Services System Policy #700-M05 Stoma and Tracheostomy Care – Adult & Pediatric STOMA AND TRACHEOSTOMY CARE – ADULT & PEDIATRIC Effective Replaces Review May 1, 2015 June 2012 November 2017 Introduction Due to our aging population, advances in ventilator technology, and the tendency to treat more medical conditions from home, EMS personnel are increasingly more likely to encounter patients with stomas or tracheostomies in respiratory distress. Temporary or permanent placement of a tracheostomy tube is often necessary to maintain an open airway. Patients with tracheostomy tubes or stomas should not be intubated orally. Suctioning of surgical airways is often required to attempt to clear and maintain an open airway. Administration of inhaled medications will need to be given via the stomas or tracheostomy tubes. Suctioning Equipment: Appropriate sized suction catheter (Pediatrics use 8-10 F) Suction unit with adjustable suction capacity BVM with oxygen supply 5 cc syringe filled with sterile saline Contraindications: Use of demand valve Procedure: Adjust suction to 120-150 mmHg for adults; decrease suction to 80-100 mmHg for pediatrics. Apply sterile gloves Flush suction catheter with saline to lubricate tip and establish patency of suction catheter. Remove the T-tube if a tracheostomy patient is on humidified oxygen. Ventilate the patient with 100% oxygen several times. Santa Clara County Emergency Medical Services Prehospital Care Manual Policy 700-M05 Page 1 of 3 Insert the suction catheter into the stoma or tracheostomy opening with the suction off (the thumb hole open). The short length of the tracheostomy tube facilitates suctioning. Apply suction by occluding the thumb hole while slowly withdrawing the catheter in a twisting motion. Suction of a tracheostomy tube should take no longer than 5 to 7 seconds for the adult patient, and 3-4 seconds for the pediatric patient. If mucus plugs or thick secretions are present, the instillation of 3-5 cc of sterile saline may be helpful. Ventilate with 100% oxygen. Check breath sounds. Suctioning can stimulate a cough reflex. Allow the patient to cough. Be prepared to suction or catch secretions from the tracheal opening. Recheck breath sounds. Albuterol Administration Equipment: Albuterol Sterile normal saline Hand-held nebulizer or other FDA approved drug delivery device Oxygen tubing and supply Additional reservoir tubing (optional) Procedure: Assure clear airway. Suction if necessary. Assemble hand held nebulizer as for patient with intact upper respiratory tract. Attach trach collar to reservoir tubing. Connect oxygen delivery tubing to oxygen source at sufficient flow rate to produce misting. Fit trach collar over stoma or tracheostomy tube. Instruct patient to breathe slowly and deeply. Optional: mouthpiece may be replaced by additional reservoir tubing. Stoma Intubation Equipment: Appropriate sized cuffed and uncuffed ET tubes BVM Appropriate sized suction catheters Oxygen supply Suction equipment with adjustable suction capacity Santa Clara County Emergency Medical Services Prehospital Care Manual Policy 700-M05 Page 2 of 3 Contraindication: Use of demand valve Procedure: Select the largest ET tube that will fit through the stoma without force. Check the cuff, unless an uncuffed tube is being used on a pediatric patient. Oxygenate with 100% oxygen using a BVM with the face mask fitted over the stoma. Do NOT use a demand valve. Wear sterile gloves. Do not use a stylet. It is not necessary to lubricate the tube. Suction, if necessary. Pass the ET tube and inflate the cuff (Note: The provider must be mindful of the depth of ET Tube placement. Passing the ET tube too deep can result in mainstem bronchus placement. The pharynx has been bypassed, so the tube will protrude from the neck several inches. Hold the tube in place, watch for chest rise with ventilation. Secure the tube and hyperventilate. Auscultate the lung fields. Check the neck for subcutaneous emphysema indicating false passage. Allow no longer than 30 seconds for the procedure. The table below contains the required documentation elements for every patient care record when an Endotrachael Tube is utilized. Size of ET tube Chest rise with ventilation Number of attempts Suction required Ventilation compliance Any complications with intubation Capnography used ETCO2/Capnography reading Equality of lung sounds Method for securing ET tube Santa Clara County Emergency Medical Services Prehospital Care Manual Policy 700-M05 Page 3 of 3 County of Santa Clara Emergency Medical Services System Policy #700-M05 Stoma and Tracheostomy Care – Adult & Pediatric STOMA AND TRACHEOSTOMY CARE – ADULT & PEDIATRIC Effective Replaces Review May 1, 2015June 2012 June 2012New November 20174 Introduction Due to our aging population, advances in ventilator technology, and the tendency to treat more medical conditions from home, EMS personnel are increasingly more likely to encounter patients with stomas or tracheostomies in respiratory distress. Temporary or permanent placement of a tracheostomy tube is often necessary to maintain an open airway. Patients with tracheostomy tubes or stomas should not be intubated orally. Suctioning of surgical airways is often required to attempt to clear and maintain an open airway. Administration of inhaled medications will need to be given via the stomas or tracheostomy tubes. Tracheostomy tube replacement: A dislodged tracheostomy tube should not be replaced, unless the paramedic has the skill and training to do so. Suctioning Equipment: Appropriate sized suction catheter (Pediatrics use 8-10 F) Suction unit with adjustable suction capacity BVM with oxygen supply 5 cc syringe filled with sterile saline Contraindications: Use of demand valve Procedure: Adjust suction to 120-150 mmHg for adults; decrease suction to 80-100 mmHg for pediatrics. Apply sterile gloves Flush suction catheter with saline to lubricate tip and establish patency of suction catheter. Remove the T-tube if a tracheostomy patient is on humidified oxygen. Santa Clara County Emergency Medical Services Prehospital Care Manual Policy 700-M05 Page 1 of 3 Ventilate the patient with 100% oxygen several times. Insert the suction catheter into the stoma or tracheostomy opening with the suction off (the thumb hole open). The short length of the tracheostomy tube facilitates suctioning. The catheter may be directed through the right or left bronchus by having the patient turn his/her head to the opposite side. Apply suction by occluding the thumb hole while slowly withdrawing the catheter in a twisting motion. Suction of a tracheostomy tube should take no longer than 10 5 to 7 seconds for the adult patient, and 3-4 seconds for the pediatric patient. If mucus plugs or thick secretions are present, the instillation of 3-5 cc of sterile saline may be helpful. Hyperventilate Ventilate with 100% oxygen. Check breath sounds. Suctioning can stimulate a cough reflex. Allow the patient to cough. Be prepared to suction or catch secretions from the tracheal opening. Recheck breath sounds. Albuterol Administration Equipment: Albuterol Sterile normal saline Hand-held nebulizer or other FDA approved drug delivery device Oxygen tubing and supply Additional reservoir tubing (optional) Procedure: Assure clear airway. Suction if necessary. Assemble hand held nebulizer as for patient with intact upper respiratory tract. Attach trach collar to reservoir tubing. Connect oxygen delivery tubing to oxygen source at sufficient flow rate to produce misting. Fit trach collar over stoma or tracheostomy tube. Instruct patient to breathe slowly and deeply. Optional: mouthpiece may be replaced by additional reservoir tubing. Stoma Intubation Equipment: Appropriate sized cuffed and uncuffed ET tubes BVM Appropriate sized suction catheters Santa Clara County Emergency Medical Services Prehospital Care Manual Policy 700-M05 Page 2 of 3 Oxygen supply Suction equipment with adjustable suction capacity Contraindication: Use of demand valve Procedure: Select the largest ET tube that will fit through the stoma without force. Check the cuff, unless an uncuffed tube is being used on a pediatric patient. Oxygenate with 100% oxygen using a BVM with the face mask fitted over the stoma. Do NOT use a demand valve. Wear sterile gloves. Do not use a stylet. It is not necessary to lubricate the tube. Suction, if necessary. Pass the ET tube and inflate the cuff (Note: The provider must be mindful of the depth of ET Tube placement. Passing the ET tube too deep can result in mainstem broncusbronchus placement. The pharynx has been bypassed, so the tube will protrude from the neck several inches. Hold the tube in place, watch for chest rise with ventilation. Secure the tube and hyperventilate. Auscultate the lung fields. Check the neck for subcutaneous emphysema indicating false passage. Allow no longer than 30 seconds for the procedure. The table below contains is the required documentation elements for every patient care record that when an Endotrachael Tube is utilized. Documentation Points Size of ET tube Chest rise with ventilation Number of attempts Suction required Ventilation compliance Any complications with intubation procedureAny complications with intubation Capnography used ETCO2/Capnography reading Equality of lung sounds Method for securing ET tube Santa Clara County Emergency Medical Services Prehospital Care Manual Policy 700-M05 Page 3 of 3