Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Management of acute coronary syndrome wikipedia , lookup
Coronary artery disease wikipedia , lookup
Heart failure wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Jatene procedure wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Cardiac surgery wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Electrocardiography wikipedia , lookup
Myocardial infarction wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Evaluation of the Contractile State of the
Human Heart from the First Derivative
of the Apexcardiogram
By ATTILLO REALE, M.D.
SUMMARY
Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017
The first derivatives of the left ventricular pressure pulse (dp/dt LV) and of the
apexcardiogram (A ACG) were recorded 73 times in 45 subjects, and the time intervals
from the peak of the R wave of the electrocardiogram to the peak of the derivatives
(t-dp/dt LV and t-A ACG) were determined under different circulatory conditions.
These parameters express the duration of the development of maximum tension during
isometric contraction of the ventricle. The values obtained from the left ventricular
pressure pulse and from the ACG showed close correlation both at rest and after pharmacological interventions which enhanced or depressed the myocardial contractile state.
During orciprenaline infusion, t-dp/dt LV and t-A ACG were consistently shortened,
while they increased in most cases after beta-adrenergic receptor blockade.
Determination of the time to peak derivative of the ACG, a parameter so far unexplored, is proposed as a simple method of detecting changes in the myocardial
contractile state in the intact human being.
Additional Indexing Words:
Myocardial contractility
First derivative
Beta-adrenergic stimulation
interval ffrom the onset of ventricular contraction tto the peak of the first derivative,
rather thain only the magnitude of dp/dt. The
factor thius obtained (t-dp/dt) expresses the
duration (of the development of maximum tension in tIhe ventricle. It varies inversely with
the myoc,ardial contractile state and is said
to be uniinfluenced by variations of ventricular load. The validity of this method was
verified cDn canine heart, on human isolated
papillary muscles, and in man under varying
conditionLs of contractility and ventricular
load. A rshortening of t-dp/dt always corresponded to an increase, and a lengthening of
it, to acdecrease of the myocardial contractile state. .4 5 However, this, as well as other
nnnrno rhlLes to the analysis of the first derivative of tHhe ventricular pressure pulse,3 obviously reqiuires left heart catheterization. Hence,
simpler yyet reliable methods for the evaluation of miyocardial contractility would be ad-
HANGES in myocardial contractility
have generally been interpreted as in-
dicating changes in cardiac performance.
Consequently, much effort has been devoted
to the evaluation of the contractile state of the
heart.
Among the different parameters used as
indices of contractility, one of the more commonly employed methods relates to the analysis of the rate of pressure rise in the left ventricle, or first derivative of the ventricular
pressure pulse.1 2 Its value, however, is limited
by the fact that dp/dt is influenced by factors extraneous to contractility such as variations in ventricular preload and afterload.3 4
To overcome the latter difficulty, Mason and
associates4 5 proposed to determine the time
From the Cardiovascular Department, Clinic of
Surgery, University of Rome, Rome, Italy. (Director:
Prof. P. Valdoni.)
Address for reprints: Dr. A. Reale, Via Panama
68, Rome, Italy.
Circulation, Volume XXXVI, December 1967
Beta-adrenergic blockade
vantageo Ius.
933
934
REALE
Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017
The recording of the low frequency displacement curves of the precordium overlying the apex of the heart yields a tracing,
commonly known as the 'apexcardiogram"
(ACG), which has been extensively used in
the study of the mechanical function of the
heart in health and disease.6-10 A close correlation has been repeatedly demonstrated
between the ACG and the hemodynamic
events within the left heart.7
13
This similarity suggested that it could be
possible to substitute for the left ventricular
pressure pulse the ACG, by analyzing the
rate of ascent of the systolic phase of the
ACG, as determined by the recording of its
first derivative.14
Owing to the difficulty in calibrating the
sensing devices, and therefore, in assigning a
unit of measurement to the first derivative of
the ACG, the latter by itself appeared inadequate for the quantitative evaluation of ventricular function. An analysis of the ACG in
terms of the time interval from the onset of
contraction to the peak of its first derivative
bypasses this difficulty, as it is expressed in
time units, independently of the height of
the derivative.15
The purpose of the present study was to
determine (1) whether correlation exists between the measurements, time to peak of the
first derivative of the left ventricular pressure
pulse (t-dp/dt LV) and time to peak of the
first derivative of the apexcardiogram (t-A
ACG), and (2) whether pharmacologically
induced variations in the contractile state
would cause parallel modifications of the
above parameters.
Methods
In seven normal individuals and in 38 patients
with acquired and congenital heart disease (table 1), the following data were obtained in the
course of diagnostic cardiac catheterization: (1)
left ventricular pressure through the transseptal
or retrograde arterial route,* (2) brachial arterial
pressure,* (3) apexcardiogram, (4) first derivative of the left ventricular pressure (dp/dt LV),
and (5) first derivative of the apexcardiogram
(A ACG).
*Statham P23 Db
pressure
transducers.
Table 1
Summary of Diagnoses of the Forty-five Subjects
Studied
Diagnosis
Cases
No heart disease
Mitral valvular disease
Aortic valvular disease
Patent ductus
Ventricular septal defect
Atrial septal defect (ostium primum)
Myocardiopathy
14
19
19
2
1
1
1
The apexcardiogram was recorded by means
of a piezo-electric microphonet and an amplifier with the band-pass filter set to 0.1 cycles/sec
for the lower limit and to 20 cycles/sec for the
higher limit.t The microphone was held by hand
at the point of maximal apical impulse with the
patient in the supine position. The first derivatives of pressure and ACG were obtained by
means of an RC differentiator with a time constant of 0.5 msec. The instrument has an output
proportionately linear to input frequency within
5%, up to a maximum frequency of 75 cycles.t
All tracings were recorded at 100 mm/sec paper
speed with time lines at 0.05 sec.
In 11 patients the procedure was repeated in
an exactly similar fashion during intravenous infusion of orciprenalinet and after intravenous injection of a beta-adrenergic receptor blocking
agent.§P6, 17
For each different circulatory situation, the
duration in milliseconds was measured from the
peak of the R wave of the electrocardiogram to
the peak of the first derivative of the left ventricular pressure (t-dp/dt LV) and from peak
of R wave to peak derivative of the apexcardiogram (t-A ACG) on a minimum of five cardiac
cycles and averaged. In the only two patients of
the series with atrial fibrillation, the measurements were made on the beats with a preceding
diastole of equal length.
Results
The time to peak of the first derivative of
the left ventricular pressure and the time to
peak of the first derivative of the ACG were
identical in 23 of the 45 persons studied
under basal conditions (from 40 to 92 msec,
tElectronics for Medicine Inc., White Plains, New
York.
*Dihydroxyphenyl-isopropylaminoethanol
sulfate,
registered name Alupent.
§Ciba 39089-Ba.
Circulation, Volume XXXVI, Decemiber 1967
FIRST DERIVATIVE OF APEXCARDIOGRAM
nTns
935
average 64 msec). In 15 cases, t-dp/dt LV
longer, and in seven cases, shorter than
I100
t-A
ACG.
In both groups the maximum differ-t-dp/dfLV
was
10 msec and the average difference
ence
0
v- , AC G
90
90
- - ____
was 7 msec. The same proportion of agree380
> ment
_ w and disagreement between t-dp/dt LV
80._
_
___
and t-A ACG was observed when the total
of 73 determinations obtained from the
70
7rnumber
45 subjects were considered, that is, under ba70 :l C1X3<11t T r
- sal conditions, during orciprenaline infusion,
e0-y-S
60 -e
and after beta blockade (fig. 1). Time to peak
- -j-C
+
L derivative of the left ventricular pres- {
first
_of
sure and time to peak of the first derivative
- - - A
50
50
of _the
r
_ 1ACG
I were identical in 39 instances
25
to 92 msec; average, 57 msec). In
(from
r40
40
oe _-<L
25 instances t-dp/dt LV was longer and in
- - 30
nine, shorter than t-A ACG. In both groups
1
30
______ j
:the maximum difference was 10 msec and
the average difference was 6 msec. In the
..3 120
---X
20 2-0____ - - - - - - -11 patients submitted to intravenous infusion
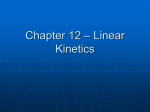
of orciprenaline, a drug which stimulates betaFigure 1
- r
ms
100
was
tI
Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017
7omparison of values for t-dp/dt LV and t-A ACG.
Each closed circle and each open circle correspond to
c
ne determination.
a
creases ranging from 5 to 30 msec
(average,
ms
100
ms
1
b
a b c
cases
Figure 2
Variations of t-dp/dt LV and t-A ACG during orciprenaline infusion. (a) At rest, (b) during
orciprenaline, (c) after orciprenaline infusion was discontinued. Each set of two or three bars
represents one patient.
Circulation, Volume XXXVI, December 1967
REALE
936
ACG
dp/dt L
ECt
Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017
Figure 3
(a) Simultaneous recordings of left ventricular pressure (LV), brachial arterial pressure (BA), ECG, apexcardiogram (ACG) and first derivative of left ventricular pressure (dp/dt LV); t-dp/dt LV 65 msec.
(a1) Same as a, with first derivative of apexcardiogram
(A ACG); t-A ACG 65 msec. (b) Same recordings
as in (a) during orciprenaline infusion; t-dp/dt LV =
45 msec. (bl) Same as in a, during orciprenaline
fusion; t-A ACG = 50 msec.
in-
msec); similarly, t-A ACG was shortened
in all cases (6 to 35 msec; average, 17 msec)
(fig. 2). In six of these patients, determinations repeated after the infusion was stopped
showed parallel returns of values toward
preinfusion levels (figs. 2 and 3). Following
beta-adrenergic blockade, the time to peak of
the first derivative was always affected in a
similar fashion for left ventricular pressure
and apexcardiogram. In eight instances tdp/dt LV and t-A ACG increased from 10 to
30 msec (average, 18 msec) and from 10 to
30 msec (average, 20 msec), respectively.
There was no change in two cases and a
slight decrease of both parameters (-5 msec)
in one patient (figs. 4 and 5).
15
Discussion
A statement of validity of the method proposed in the present investigation should be
supported by an affirmative answer to the
following questions: (1) Does the upstroke
of the systolic phase of the apexcardiogram
correspond to the isometric contraction of
the left ventricle? (2) Does the parameter,
time to peak derivative of the left ventricular
pressure represent a reliable measurement
of the myocardial contractile state? (3) Are
variations of the time to peak derivative of
the ACG comparable to those of the time to
peak derivative of the left ventricle under
different conditions of contractility?
Studies of simultaneous recordings of intracardiac pressures and of the apexcardiogram haMe repeatedly demonstrated that the
rapid rising portion of the ACG comprised
between the end of the a wave and the peak
of the curve (E point) is inscribed during
the ascending limb of the left ventricular
pressure pulse and represents the period of
isometric contraction.7' 11-13 Our data confirmed these findings. Configuration and time
relationships on the ACG corresponded closely to the pressure events in the left ventricle. According to Tavel and associates,'2
corrections should be made on the time measurements for the different delay in conduction
through the cardiac catheters and through
the recording devices of the ACG, the difference being approximately a 3-msec lag of
the pressure curve behind the ACG deflections. In our study, standard catheters and
pressure transducers rather than catheter tip
manometers were used for the recording of
left ventricular pressure and of its derivative.
The main reason for this was that the left
ventricle was entered by transseptal or retrograde arterial catheterization by the percutaneous Seldinger technique which does not
permit the use of micromanometers. This
technique may have introduced phase shifts
and distorted to some extent time relationships as far as dp/dt LV is concerned. However, we were not interested in absolute
values, but rather in changing measurements
Circulation, Volume XXXVI, December 1967
FIRST DERIVATIVE OF APEXCARDIOGRAM
937
Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017
a b
cases
Figure 4
Variations of t-dp/dt LV and t-A ACG after beta-adrenergic receptor blockade. (a) At rest, (b)
after beta-adrenergic blockade. Each pair of bars represents one patient.
I
IaI1
A ACG
ACG
ACG
_
EC
H1! 11 l 11 1 11LVl 11
{ X
/
G11
11
in the same patient under different circulatory
conditions. Thus, any imprecision introduced
by the method of recording could be expected
to influence the measurements in the same
patient to the same degree before and after
pharmacological interventions. In this study,
the first derivative of the left ventricular
1\ Cpressure was used only as a reference for the
events which were being investigated on the
apexcardiogram. Therefore, corrections for
the delay in conduction through the different
systems were not considered essential to the
ultimate purpose of this study. It appeared
b)
bl
Figure 5
(a) Simultaneous recordings of left ventricular
ACG
As\ \ <\
^
9,<
BA
EC
LIVIII 1 11 1flI
Circulation, Volume XXXVI, December 1967
pres-
(LV), brachial arterial pressure (BA), ECG, apexcardiogram (ACG) and first derivative of left ventricu,lar pressure (dp/dt LV); t-dt/dp LV =45 mec.
sure
A
CG
(a,) Same as a showing the first derivative of ACG
(A ACG); t-A ACG = 38 msec. (b) Same tracings as
in a but after j3-adrenergic blockade; t-dp/dt LV = 60
msec. (b,) Same tracings as in a, but after p-adrenergic blockade; t-A ACG=60 msec.
REALE
938
dp/dILV mmHg/sec.
7500
7500
i
P
$ STIMULATION
BLOCKADE
6500
6500tf
5500
6500-~~~~~~~~~~~~~~f.
5500
4500
4500
3500
3500
Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017
2500
\s
1500i
x
.2500
\-
500
1500
500
20
30
40
50
60
40
20 30
t-dp/dt LV ms
Figure 6
70
50
60
70
80
90
Variations of dp/dt LV and t-dp/dt LV after j-adrenergic stimulation and p-adrenergic blockade. Each line represents one patient; the arrow points to the value obtained after pharmacological intervention.
justified to use the first derivative of the ACG
as a measure of the rate of development of
tension that occurs during isometric contraction of the ventricle, and hence the interval,
time to peak derivative of the ACG, should
have the same significance as the interval,
time to peak derivative of the left ventricular
pressure, in expressing the duration of the
development of maximum tension.5 Comparison of the absolute values for both parameters
under control conditions seems to support
the following statement: the time intervals
were identical in most cases and deviated
only slightly from each other in the remaining
determinations. In other words, the duration
of the development of maximum tension was
similar whether determined from the left ventricular pressure or from the apexcardiogram.
It is hardly believable that such a degree
of correlation in a significant number of determinations could have been the result of
coincidence.
The present study confirmed the findings
of Mason and associates.4 When the myo-
cardial contractile state was enhanced by
orciprenaline infusion, there was an elevation
of peak dp/dt accompanied by a decline in
t-dp/ dt. Conversely, when contractility was
depressed by beta-adrenergic blockade, most
patients showed a lower peak of dp/ dt in the
face of a prolonged t-dp/dt (fig. 6). There
were only rare instances in which the height
of dp/dt and t-dp/dt did not vary in the
expected direction in respect to each other.
For practical purposes, therefore, it appears
from these data that t-dp/ dt by itself may be
used as an index of a changing contractile
state without consideration of the variations
in the size of the derivative. This observation
was essential for the method described in
the present study, as it is extremely difficult
to calibrate the recording devices of the ACG
and assign a unit of measurement to the
derivative of the ACG. This was the fundamental rationale for choosing the parameter
time to peak of the derivative in the attempt
to utilize the ACG as an index of changes in
the contractile state. It is well known that
Circulation, Volume XXXVI, December 1967
FIRST DERIVATIVE OF APEXCARDIOGRAM
Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017
the size of the ACG can change considerably
depending on how the crystal is held to the
chest wall. In our experiments reproducibility was the rule in repeated predrug determinations; when the sensing device was
repositioned after pharmacological interventions which affected the hemodynamic situation, it was usually impossible to reproduce
the same aspect of the ACG as before drug
administration. The actual size of the derivative of the ACG changed too in the expected
direction (figs. 3 and 5). Although no attempt
was made at quantitating these changes because of the above-mentioned calibration
problems, it is possible that technical refinements could lead to the inclusion of the size
of A ACG in the evaluation of contractile
state.
It is recognized that a change in heart
rate and hence in total cycle length by itself
may affect measurement of the time to peak
derivative, since most time intervals tend to
change in the direction in which cycle length
is altered. In our experiments with drugs,
no correction was made for changes in heart
rate. However, when variations of time to
peak derivative were expressed in percentage
deviation from the predrug values and compared to the percentage changes in total
cycle length, the following values were obtained. In 16 of the 20 instances in which
drug administration affected the measurement
of the time to peak derivative, this variation
was definitely greater than the change in
cycle length; in three, it was slightly less
when marked changes in heart rate had occurred, and in one, it was equal to the change
in cycle length. Thus, in most cases changes
in cycle length could not be considered the
sole responsible cause of shortening or lengthening of the parameter time to peak derivative. Furthermore, the duration of maximum
tension as measured by this method was
appreciably altered even in those instances
in which drugs did not cause any significant
change in heart rate and cycle length.
The results of this study clearly indicate
that the time to peak derivative of the ACG
followed consistently the behavior of the
Circulation, Volume XXXVI, December 1967
939
time to peak derivative of the left ventricular
pressure whenever the latter deviated from
its resting values by pharmacological interventions which enhanced or depressed the
myocardial contractile state.
For the measurement of t-dp/dt LV and
t-A ACG, the peak of the R wave of the
electrocardiogram was arbitrarily chosen as
a reference point rather than the onset of
ventricular contraction. The inaccuracy which
may have resulted from comparing two entirely different recording systems was outweighed by the much greater ease of defining
the R wave than the beginning of contraction
either from the ventricular pressure pulse
or the ACG derivatives. It must be reemphasized that the method described does not in
any way attempt to establish an absolute
quantification of contractility between different individuals. The values for t-A ACG
showed too wide a range even in normal
subjects, and there was much overlapping
between the figures for normal persons and
for persons with the various diseases examined. The technique was merely designed
as a means of detecting changes in the myocardial contractile state in the same patient.
In this respect, regardless of possible imprecision, there was a closely similar behavior
of the parameter being investigated and of
that used as a reference measurement.
Some difficulties can be encountered in
producing a good apexcardiogram and hence
a reliable derivative of it. This occurs whenever the apex of the heart does not come
close enough to the chest wall during ventricular contraction to produce an appreciable displacement, as in obese or emphysematous subjects, and the need for a more
sensitive pickup device is recognized. The
best tracings were obtained in the presence
of hypertrophy or hyperactivity of the left
ventricle, and the list of diseases in table 1
reflects these situations. Moreover, the configuration and size of the ACG can be
changed considerably depending on how the
crystal is held. This, of course, introduces
the problem of reproducibility of the results.
The technique used in the present study was
940
Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017
that generally followed for the recording of
the ACG: the crystal was held by hand in
the region of the apex and manipulated until
a good quality tracing was obtained on the
oscilloscope. Recognition of a satisfactory
tracing was derived from previous experience
with apexcardiography. Once the best position was defined, it was found that the
same contour of the ACG could be reproduced at will in the same patient as long as
the hemodynamic situation remained stable.
Negation of the reproducibility of the ACG
would invalidate most of the work accomplished in this field, especially that dealing
with confrontation of ACG and intracardiac
events. The most variable factor, depending
on the amount of pressure applied by the
hand holding the crystal, was the height of
the ACG. This did affect the size of its
derivative but not to any extent the time
interval, peak of R wave to peak of derivative.
The same observation applies to the particular contour of the ACG which is obtained
in certain diseases such as aortic stenosis.
In these cases the E point can be blurred
and the ascent is broadened. Conventional
interpretation of the ACG may thus be more
difficult, but, in the present study, only the
derivative was considered and therefore sharp
definition of the E point seems relatively
unimportant. Broadening of the ascent will
be translated into a longer time for the derivative to reach its peak. This is believed to be a
direct consequence of the hemodynamics of
the diseased state which is apparent with
the same characteristics on the left ventricular
pressure pulse.
Knowledge of the configuration of the left
ventricular pressure pulse and of its derivative while recording the ACG could have
prompted the investigator to manipulate the
crystal until both derivatives looked alike,
thus invalidating the results. Because of the
insufficient available number of adequate amplifiers, derivatives of pressure and ACG were
recorded in succession so that the observer
had no simultaneous confrontation with these
curves while they were being inscribed. Attention was directed mainly at obtaining a
REALE
good quality ACG, without consideration of
its derivative. Several separate strips of recording were obtained for each determination
after repositioning the crystal on the chest
wall. In order to prevent biased interpretations of the tracings, t-A ACG was measured
in every instance before t-dp/dt LV, that is,
without knowledge of the hemodynamic
data. At any rate, the technique is designed
to be used without the adjunct of left heart
catheterization. The method is simple and
safe and causes no inconvenience to the
patient. It does not require complex or expensive equipment. Its limitations are mainly those of conventional apexcardiography.
With this in mind, it is concluded that the
time to peak derivative of the ACG, a parameter so far unexplored, does indicate changes
in the myocardial contractile state with the
same approximation as that yielded by the
factor, time to peak derivative of the left
ventricular pressure.
References
1. REEVES, T. J., HEFNER, L. L., JONES, W. B.,
2.
3.
4.
5.
6.
COGHLAN, C., PRIETO, G., AND CARROLL, J.:
Hemodynamic determinants of the rate of
change in pressure in the left ventricle during isometric contraction. Amer Heart J 60:
745, 1960.
GLEASON, W. L., AND BRAUNWALD, E.: Studies
on the first derivative of the ventricular pressure pulse in man. J Clin Invest 41: 80,
1962.
SIEGEL, J. H., SONNENBLICK, E. H., JUDGE,
R. D., AND WILSON, W. S.: Quantification of
myocardial contractility in dog and man. Cardiologia 45: 189, 1964.
MASON, D. T., SONNENBLICK, E. H., Ross, J.,
COVELL, J. W., AND BRAUNWALD, E.: Time
to peak dp/dt: A useful measurement for evaluating the contractile state of the human
heart. (Abstr.). Circulation 32 (suppl. II):
II-145, 1965.
MASON, D. T.: Cardiovascular effects of digitalis
in normal man. Clin Pharmacol Ther 7: 1, 1966.
LUISADA, A. A., AND MAGRI, G.: Low frequency
tracing of the precordium and epigastrium in
normal subjects and cardiac patients. Amer
Heart J 44: 545, 1952.
7. BENCHIMOL, A., AND DIMOND, E. G.: Normal
and abnormal apex cardiogram: Its physiologic variation and its relation to intracardiac events. Amer J Cardiol 12: 368, 1963.
Circulation, Volume XXXVI, December 1967
FIRST DERIVATIVE OF APEXCARDIOGRAM
941
AVITA, J. P., AND BROUSTET, P.: Etude com-
Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017
8. DIMOND, E. G., AND BENCHIMOL, A.: Correlation of intracardiac pressure and precordial
movement in ischaemic heart disease. Brit Heart
J 25: 398, 1963.
9. NIXON, P. G. F., AND WOOLER, G. H.: Phases of
diastole in various syndromes of mitral valvular
disease. Brit Heart J 25: 393, 1963.
10. COULSHED, N., AND EPSTEIN, E. J.: Apex cardiogram: Its normal features explained by
those found in heart disease. Brit Heart J
25: 697, 1963.
11. TAFUR, E., COHEN, L. S., AND LEVINE, H. D.:
Normal apex cardiogram: Its temporal relationship to electrical, acoustic and mechanical
cardiac events. Circulation 30: 392, 1964.
12. TAVEL, M. E., CAMPBELL, R. W., FEIGENBAUM,
H., AND STEINMETZ, E. F.: Apex cardiogram
and its relationships to hemodynamic events
within the left heart. Brit Heart J 27: 829,
1965.
13. DALOCCHIO, M., BRICAUD, H., DROUET, B., BON-
14.
15.
16.
17.
parative du cardiogramme apexien et des
traces de pression intraventriculaires gauches.
Arch Mal Coeur 58: 1078, 1965.
AMBROSI, C., AND STARR, I.: Incoordination of
the cardiac contraction as judged by the force
ballistocardiogram and carotid pulse derivative. Amer Heart J 70: 761, 1965.
REALE, A.: Value of the apex cardiogram in assessing the contractile state of the human heart.
Fifth World Congress of Cardiology. New Delhi, 1966. Abstracts, part II, p. 147.
GARNIER, B., AND IMHOF, P.: Beeinflussung von
Kreislauffunktionsproben ( Orthostasereaktion,
Valsalva, Reaktion auf Vasopressoren) durch
Beta-Rezeptoren-Blockade. Cardiologia 49: 146,
1966.
REALE, A., IMHOF, P., AND MOTOLESE, M.: Influence of beta-adrenergic blockade on the
immediate haemodynamic effects of angiocardiography. Brit Heart J 29: 761, 1967.
.4.
To Perish by Silence
What is needed, suggests Oppenheimer, is a harsh modesty, an affirmation that
common men cannot, in fact, understand most things and that the realities of which
even a highly trained intellect has cognizance are few and far between.
With respect to the sciences, this somber view seems unassailable. And perhaps it
dooms most knowledge to fragmentation. But we should not readily accede to it in history, ethics, economics, or the analysis and formulation of social and political conduct.
Here literacy must reaffirm its authority against jargon. I do not know whether this
can be done; but the stakes are high. In our time, the language of politics has become
infected with obscurity and madness. No lie is too gross for strenuous expression, no
cruelty too abject to find apologia in the verbiage of historicism. Unless we can restore
to the words in our newspapers, laws, and political acts some measure of clarity and
stringency of meaning, our lives will draw yet nearer to chaos. There will then come
to pass a new Dark Ages.-GEORGE STEINER: Language and Silence: Essays on Language, Literature, and the Inhuman. New York, Atheneum, 1967, p. 34.
Circulation, Volume XXXVI, December 1967
Evaluation of the Contractile State of the Human Heart from the First Derivative
of the Apexcardiogram
ATTILIO REALE
Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017
Circulation. 1967;36:933-941
doi: 10.1161/01.CIR.36.6.933
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1967 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
http://circ.ahajournals.org/content/36/6/933
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles
originally published in Circulation can be obtained via RightsLink, a service of the Copyright
Clearance Center, not the Editorial Office. Once the online version of the published article for
which permission is being requested is located, click Request Permissions in the middle column of
the Web page under Services. Further information about this process is available in the Permissions
and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/