Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
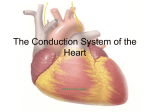
Wenckebach Periods in the Bundle Branches By MAURICIO B. ROSENBAUM, M.D., GERARDo J. NAU, M.D., RAUL J. LEVI, M.D., M. SUSANA HALPERN, M.D., MARCELO V. ELIZARI, M.D., AND JULIO 0. LAZZARI, M.D. SUMMARY Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 Two cases of intermittent bundle-branch block in which Wenckebach periods could be directly visualized are reported. The conduction ratios were either 3:2 or 4:3, as are commonly seen in cases of the Wenckebach phenomenon of atrioventricular (A-V) conduction. Other groups of beats apparently showing 3:1 and 4:1 bundle-branch block were interpreted as indicating incompletely concealed Wenckebach periods in the bundle branches, with actual conduction ratios of 3:2 and 4:3, respectively. Three prerequisites are necessary for the occurrence of either direct or incompletely concealed Wenckebach periods in the bundle branches: (1) The opening beat should be normally conducted (in the affected bundle branch); (2) the second beat should be conducted with a delay of no more than 0.04 to 0.06 sec; (3) the damaged bundle branch should not be activated retrogradely in the closure beat. Wenckebach periods in the bundle branches may be completely concealed if the conduction delay lasts more than 0.04 to 0.06 sec in the opening beat. In cases of bilateral bundle-branch block, Wenckebach periods in the bundle branches may be indirectly visualized through changes in the A-V conduction. Additional Indexing Words: Concealed conduction in the bundle branches Trifascicular blocks T HE EXISTENCE of Wenckebach periods in patients with partial A-V block is well known. However, since Wenckebachl first described the periodic block which follows progressive prolongation of the A-V interval, several authors have pointed out that such a phenomenon has never been observed in the main branches of the bundle of His.2 the existence of concealed Wenckebach riods in the bundle branches. pe- Report of Cases Case 1 The electrocardiograms of a 61-year-old man with pulmonary abscess and aortic valvular disease showed severe left ventricular hypertrophy, first degree A-V block, and intermittent left bundle-branch block (LBBB) (fig. 1). Figure 2 illustrates typical direct Wenckebach periods in the left bundle branch. The first beat displays a pattern of complete LBBB, with a QRS interval of 0.16 sec. The QRS interval measured 0.10 sec in the second beat, 0.11 sec in the third, 0.12 sec in the fourth, and again, 0.16 sec in the fifth beat. Beats 2 to 5 constitute a typical Wenckebach period. The sixth beat starts a new period of three beats (beats 6 to 8). The narrowest and most normal QRS complexes (beats 2, 6, and 9) followed the QRS complexes having the pattern of complete LBBB (1, 5, and 8), indicating that conduction in the left bundle branch failed completely in In this paper, two such cases are reported. In both, groups of beats showing a progressive increase in the degree of the bundle-branch block were observed up to the complete bundle-branch block beat that closed the period. These groups were considered to indicate direct Wenckebach periods. In addition, other groups of beats were observed which indicated From the Services of Cardiology of Salaberry Hospital and Argerich Hospital, Buenos Aires, Argentina. Circulation, Volume XL, July 1969 Bilateral bundle-branch block 79 80 ROSENBAUM ET AL. tSF45..( ^ W; :,.-,. :,s,l:(-;0-^.:- 4~~ s~. ~.. . .. .~. . a; t ::1wK:- -R 7 r20-. -& ! Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 V. .It s W. Figure vt 1 Case 1. In each lead the first beat is without, and the second with, LBBB. However, there is some degree of incomplete LBBB in the "normally" conducted beats. in the first The QRS itnterval widens from 0.10 beat to 0.16 sec in the second one. sec beats 1, 5, and 8 only, while conduction in the left bundle branch was delayed but not interrupted in beats 3, 4, and 7. The changes in QRS duration and configuration occurred without a change in the heart rate or the P-R interval. Therefore, figure 2 exhibits two typical direct Wenckebach periods within the left bundle branch, with conduction ratios of 4:3 and 3:2, respectively. Forty-four direct Wenckebach periods of the same kind, with 3:2 and, less frequently, 4:3 conduction, were recorded on the same patient. In addition, interspersed among the typical Wenekebach periods, some other types of QRS grouping occurred, as illustrated in figure 3. Figure 3 shows three groups of beats. In the first group, containing four beats (2 to 5), the initial QRS complex shows a normal* pattern of *For simplicity, all the beats having the shortest QRS interval and initiating the Wenckebach periods will be called "normal." "Complete" means that, although the electrocardiographic pattern looks like complete LBBB, we cannot be sure that conduction completely interrupted. was intraventricular conduction, while the last three QRS complexes have a pattern of "complete"* LBBB. The next two groups (beats 6 to 8 and 9 to 11) include three beats each. In both, the QRS complex of the first beat is normal. while the last two have a pattern of "complete" LBBB. As in figure 2, the normal beats initiating these periods (beats 2, 6, and 9) always follow a beat with the "complete" LBBB pattern. This stuggests that conduction in the left bundle branch was completely blocked in the preceding beats (beats 1, 5, and 8) only. However, how conduction took place in beats 3 and 4 of the first period and in beats 7 and 10 of the last two periods in the left bundle branch needs clarification. The LBBB configuration of beats 3, 4, 7, and 10 may be explained in one of two ways: either (1) conduction was completely blocked in the damaged region of the left bundle branch (during these beats); or (2) the impulse was conducted in the left bundle branch with a delay greater than 0.04 to 0.06 sec, which is the accepted critical time interval"1-13 necessary for the impulse to arrive from the contralateral ventricle and to produce a pattern of "complete" LBBB. In the first hypothesis, the periods shown in figure 3 would mean 4:1, 3:1, and 3:1 block in the left bundle branch; in the second, these periods would indicate 4:3, 3:2, and 3:2 conduction, with Wenckebach phenomenon. Two observations lend support to the second possibility: First, in the same tracings, direct Wenckebach periods in the left btundle branch, with the same 4:3 and 3:2 conduction ratios were observed, as shown in figure 2. Second, in second degree A-V block, 3:2 conduction of the Wenckebach type is more common thani 3:1 conduction; and 4:3 conduction of the Wenckebach type is much more common than 4:1 conduction. Therefore, the three groups of beats shown in figure 3 most likely indicate Wenckebach periods within the left bundle branch, with conduction ratios of 4:3, 3:2, and 3:2, respectively. We shall refer to these periods as "incompletely concealed Wenckebach periods." Figure 4 shows four successive beats with a pattern of "complete" LBBB, preceded and followed by a normal beat. Since the changes in QRS pattern are unrelated to changes in cycle duration, they could indicate another Wenckebach period in the left bundle branch with a conduction ratio of 5:4. Again, the normal beat (beat 6) indicates that the left bundle branch completely failed to conduct in the preceding beat. A progressive conduction delay may again be assumed, starting with an initial delay greater than 0.04 to 0.06 sec. The second half of the strip in figure 4 reveals 2:1 LBBB. Circulation, Volume XL, July 1969 . WENCKEBACH PERIODS IN THE BUNDLE BRANCHES 2 1 4 3 5 6 9 8 7 81 *R(rAi; x :A 1 t il' 1 Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 Ef :? .: ;:2!|: i: :S::t Case 1. V, and lead Figure 2 simultaneously recorded, showing I, left bundle branch. The conduction the second one (beats 6 to 8). 3 2 1 5 4 ; jf i*i+( 12 11 10 9 8 7 6 'iT|i ., i two direct Wenckebach periods in the the first period (beats 2 to 5) and 3:2 in ratio is 4:3 in 11, . 4.: '. .... " I J 1.i -j- .i - 4- 4.- If .1 1. .. t Figure 3 Case 1. Three groups of beats (beats number 2 to 5, 6 to 8, and 9 to 11) looking, respectively, as 4:1, 3:1, and 3:1 LBBB. However, these were interpreted as incompletely concealed Wenckebach periods, with 4:3, 3:2, and 3:2 conduction ratios, respectively. 1 2 3 4 6 5 7 8 9 10 Figure 4 Case 1. Beats number 1 to 5 are interpreted bach period in the left bundle branch, with typical 2:1 LBBB. Case 2 A 72-year-old man with arterial hypertension had an intermittent right bundle-branch block (RBBB) (fig. 5). From July 8, 1967 to March Circulation, Volume XL, July 1969 as a forming an incompletely concealed Wencke5:4 conduction ratio. Beats 6 to 10 reveal a 15, 1968, six tracings were obtained, all of which showed essentially similar findings. Figure 6 exhibits typical direct Wenckebach periods in the right bundle branch with 4:3 or 3:2 conduction 82 _-.5<+OSZ*XPAYatj1vF4es_>.fri*,|M;IwmvF0t7on.YA_*f>i+,s:0eP.-|r_ a_Fe:.46s8@t*-1-XiFDq.!stSelb-wX:+*fjyiseAd}Q.a+8:-xb>W_ea+4-wX.i%A.&6*rX_o>*<0Yst+msSWvz$tMA+._4b'ft.>+|>i-s1S-y*xTov5*<e_.,z9aF4;r+StXHwi-UsFqs(-o6+Ev.a+z4<>_.g;et7Si*sd; -~4* :#,. t- i .Fi :=i .y - *n: =s. +. e I -t +|++ ++ | _ I ., -4-" r+++: _- 1j4: ;t-?, ,,e tx -* - v .k H +-+|- _ t e * 98 + t . + 6-St v . s.4--T -tt -.I,. 1 t .+ q. ROSENBAUM ET AL. NT" f j ++ 4 ev.s s.j. | . lo f isg, r .... 1 A >! (l; si Z | 0 t :t:> 3(t' t (, :':til::; 3 ; ; t: X=eff+++* * * | :; :0:|-( .|o: f , | t: \;t; ::|: 0 t: ! o >; _ Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 Figure 5 Case 2. In every lead, the first beat is without and the second w;ith RBBB. However, there is definitely some degree of incomplete RBBB in the "normally" conducted beats. The QRS interval widens from 0.08 to 0.12 sec. 1 ;; 3 2 4 5 6 7 8 9 10 11 fi ft I~~~~~~~~~~~~~~~~I I -. ..... .... Ii Figure 6 Case 2. Beats number 2 to 5 constitute a ditect Wenckebach period within the right bundle branch, with a 4:3 conduction ratio. Another direct Wenckebach period with a 3:2 conduction ratio is formed by beats number 8 to 10. The QRS interval measures 0.08 sec in beat number 2, 0.09 sec in beat number 3, 0.10 sec in beat number 4, and 0.12 sec in beat number 5. Both Wenckebach periods are linked by a period of 2:1 RBBB. ratios. Figure 7 shows incompletely concealed Wenckebach periods, appearing as 3:1 or 4:1 RBBB, but indicating (as in case 1) 3:2 and 4:3 conduction ratios, with Wenckebach phenomenon (beats 2 to 4 and 5 to 8); and in the same strip, a direct Wenckebach period (beats 9 to 11). Discussion In 1925, Scherf and Shookhoffj7 in an experiment using dogs, demonstrated the existence of Wenckebach periods within the bundle branches. After sectioning one branch and damaging the other only slightly, typical Wenckebach periods of the A-V conduction appeared, which undoubtedly were taking place in the less damaged bundle branch. They effectively transformed a bifascicular conduction system into a monofascicular conduction system. Taking advantage of the fact that the same trick is occasionally performed by nature, Rosenbaum and Lepeschkin12 were able to establish, also indirectly, the existence of Wenckebach periods in the bundle branches Circulation, Volume XSL, Judy 1969 83 WENCKEBACH PERIODS IN THE BUNDLE BRANCHES 1 2 3 4 7 6 5 8 9 10 11 Figure 7 Case 2. The last three beats constitute a direct Wenckebach period with a 3:2 conduction ratio. Beats number 2 to 4 form an incompletely concealed Wenchkebach period, with the same 3:2 conduction ratio. Beats number 5 to 8 form another incompletely concealed Wenckebach period, with a 4:3 conduction ratio. Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 Figure 8 Two typical Wenckebach periods with 4:3 and 5:4 conduction ratios, respectively, in a common case of second degree A-V block. The opening beat starts with an already prolonged P-FR interval (0.28 sec). of man in clinical cases of "bilateral bundlebranch block." And recently, Rosenbaum's group'4-16 substantiated, in the same indirect way, Wenckebach periods in the anterior and posterior divisions of the left bundle branch, in clinical and experimental cases of "intraventricular trifascicular block." In another type of experiment,6 one bundle branch was slightly compressed, and after allowing recovery of normal conduction, atrial flutter was induced in order to increase the ventricular rate. In this way, the conduction disturbance in the bundle branch was unmasked, and a progressive increase in the degree of bundle-branch block was shown to occur. Holzmann4' 5 reported a similar clinical observation. A patient with intermittent RBBB and atrial fibrillation showed, in consecutive beats, a progressive increase in the degree of the RBBB, with the last beat of the group exhibiting the pattern of "complete" RBBB. However, the next beat did not show normal conduction-as would be expected for a true Wenckebach phenomenon. Segers'7 reported a case showing groups of three beats; the first beat was normally conducted, the second showed incomplete LBBB, Circulaton, Volume XL, July 1969 and the third exhibited complete LBBB. These groups were preceded and followed by a ventricular extrasystole and had characteristic Wenckebach periods in the left bundle branch with 3:2 conduction. However, the fact that the periods were provoked by the ectopic beats suggests that the post-extrasystolic pauses were essential for the occurrence of the normally conducted beats starting each period. A similar case, in which a Wenckebach type of progression in the left bundle branch was observed after post-extrasystolic pauses, has been reported by Ballarino and Rumolo (their fig. 32).1' The two cases reported in this paper are, so far as we were able to determine, the first examples in which typical direct Wenckebach periods within the bundle branches were observed in conventional electrocardiographic tracings, demonstrating that Wenckebach phenomenon may actually occur in the right or the left bundle branch, just as in any other segment of the conduction system subjected to partial impairment of conduction.3 0, 13 18 2 In both cases, we could also uncover the existence of incompletely concealed Wenckebach periods. In fact, periods appearing as 3:1 or 84 Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 4:1 bundle-branch block indicated concealed Wenckebach periods within the bundle branches with 3:2 and 4:3 conduction, respectively. It is then possible that cases previously reported as examples of 3:1 and 4:1 bundlebranch block" really indicate Wenckebach periods in the bundle branches. It is also conceivable that apparently complete bundlebranch block may in fact be intermittent, with completely concealed Wenckebach periods. To render this more understandable, a parallel with Wenckebach phenomenon of the A-V conduction will be helpful. Figure 8 shows typical Wenckebach periods in a case of partial A-V block. The most rapidly conducted impulses, that is, those- occurring after the pauses, have a P-R interval of 0.28 sec, indicating a conduction delay in the A-V junction equal to or greater than 0.08 sec. Should a similar initial conduction delay occur within one bundle branch, the QRS complexes will show the pattern of "complete" bundle-branch block, in spite of the fact that Wenckebach periods are actually present under the surface. The Wenckebach phenomenon is a distinct form of impaired conduction, which occurs when impulse propagation is gradually and progressively slowed until no impulse is propagated. A possible cause for this delayed impulse propagation is a prolonged recovery time. If one impulse falls on the relative refractory period of the preceding beat, some degree of delayed conduction will occur. In turn, this delayed conduction determines a rightward displacement of the corresponding refractory period, in such a way that the next impulse (assuming an appropriate and constant rate of stimulation) will fall on an earlier phase of the recovery curve and will be conducted with greater delay, until one beat falls on the absolute refractory period and is completely blocked. This closes the period, prompts a longer resting time interval within the involved region, and allows the next impulse to be conducted normally or at least with much less delay. Also, the longer resting period produces a longer refractory time, so that the next impulse (after the normally conducted one) falls again on a ROSENBAUM ET AL. relative refractory period, thus perpetuating the cycle. Within this general set up, two factors must be further elucidated. It is well known that in typical Wenckebach impairment of A-V conduction, the greatest increment in conduction delay occurs in the second beat of the period." 5, 23-26 Should this happen in one bundle branch, the conduction delay during the second beat of the period will usually be greater than 0.04 to 0.06 sec. Under such conditions, the resulting QRS complex will have a pattern of "complete" bundlebranch block. If the next impulse is really completely blocked, the QRS complex will again show a similar pattern of complete bundle-branch block. Therefore, under usual conditions, as in the customary 3:2 conduction ratio, a Wenckebach period within one bundle branch will appear in the electrocardiogram as 3:1 bundle-branch block (a normal QRS complex followed by two with "complete"' bundle-branch block). Accordingly, for Wenckebach phenomenon in one bundle branch to appear directly in the electrocardiogram, as in the two cases presented in this paper, the second beat of the period must have a conduction delay shorter than 0.04 to 0.06 sec. The second factor is the behavior of the opening beat (the first beat following the pause of the Wenckebach period). If the opening beat regains completely normal conduction in the affected bundle branch, the Wenckebach period will start with a completely normal QRS complex. If the opening beat has a conduction delay between 0.01 and 0.04 sec, the first beat of the period will have a configuration of incomplete bundle-branch block. This actually occurred in our two cases. If the conduction delay is greater than 0.04 to 0.06 sec, however, the opening beat, as well as the following beats, will all show a pattern of complete bundle-branch block, and the Wenckebach phenomenon will be completely concealed. Therefore, another essential condition for the occurrence of direct (or incompletely concealed) Wenckebach periods in the bundle branches is that the conduction delay in the first beat of the period be no greater than 0.04 to 0.06 sec. Circulation, Volume XL, July 1969 WENCKEBACH PERIODS IN THE BUNDLE BRANCHES Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 An even more essential condition for the existence of Wenckebach phenomenon in one bundle branch is that in the beat which must close the period, there should be no retrograde activation (coming from the contralateral ventricle) of the damaged bundle branch. In fact, this has been assumed to be the only reason why the Wenckebach phenomenon in the bundle branches seems to be so uncommon.3' 10 However, since we do not know how often this takes place under the above circumstances, it is impossible to tell how important the condition is-as compared to the other two conditions previously dealt within determining the real frequency or infrequency of Wenckebach phenomenon in the bundle branches. From the preceding considerations we may conclude that for Wenckebach periods in the bundle branches to become apparent in the electrocardiogram (provided there is no retrograde activation from the contralateral ventricle), the conduction delay in the first two beats of the period should be no greater than 0.04 to 0.06 sec. If the two beats fulfill this requirement, the Wenckebach phenomenon will be directly visualized in the electrocardiogram. If only the first beat is conducted with a delay of less than 0.04 sec, the Wenckebach phenomenon will be incompletely concealed (disguised as 3:1 or 4:1 bundle-branch block). If the conduction delay of the first beat is greater than 0.04 to 0.06 sec, the Wenckebach phenomenon will be completely concealed. Accordingly, when considering the concealed forms (and also the forms precluded because of retrograde activation of the damaged bundle branch), we can say that Wenckebach phenomenon has as good a pathophysiologic chance of occurring in the bundle branches as in any other segment of the conduction system. The opinion that Mobitz type I block may be only characteristic for A-V junctional tissue27 cannot thus be supported. References 1. WENCKEBACH, K. F.: Zur Analyse des unregelmassigen Pulses: II. Mitteilung: Ueber den regelmassig intermittierenden Puls. Klin Med 37: 475, 1899. Circulation, Volume XL, July 1969 8S 2. GRANT, R. P.: Clinical Electrocardiography. New York, McGraw-Hill Book Co., 1957. 3. HERRMANN, G. R., AND ASHMAN, R.: Partial bundle branch block: Theoretical consideration of transient normal intraventricular conduction in the presence of apparently complete bundle branch block. Amer Heart J 6: 375, 1931. 4. HOLZMANN, M.: Seltene Abarten von unbestandigen Schenkelblock. Cardiologia 7: 113, 1943. 5. HOLZMANN, M.: Klinische Elektrokardiographie. Stuttgart, Georg Thieme Verlag, 1961. 6. SCHERF, D.: Reizleitungsstorungen im Schenkel. Klin Wschr 4: 2207, 1925. 7. SCHERF, D., AND SHOOKHOFF, C.: Reizleitungsstorungen im Bundel: II. Mitteilung. Wien Arch Inn Med 11: 425, 1925. 8. VESSEL, H.: Critical rates in ventricular conduction, unstable bundle branch block. Amer J Med Sci 202: 198, 1941. 9. WENCKEBACH, K. F., AND WINTERBERG, H.: Die unregelmassige Herztatigkeit. Leipzig, W. Engelman, 1927. 10. WILSON, F. N., AND HERRMANN, G. R.: Experimental study of incomplete bundle branch block and of the refractory period of the heart of the dog. Heart 8: 229, 1921. 11. KATZ, A. M., AND PICK, A.: Transseptal conduction time in the human heart: Evaluation of fusion beats in ventricular parasystole. Circulation 27: 1061, 1963. 12. ROSENBAUM, M. B., AND LEPESCHKIN, E.: Bilateral bundle branch block. Amer Heart J 50: 38, 1955. 13. STENSTROM, W.: Further experience in incomplete bundle branch block. Acta Med Scand 67: 353, 1927. 14. ROSENBAUM, M. B., ELIZARI, M. V., AND LAZZARI, J. O.: Los Hemibloqueos. Buenos Aires, Ed. Paidos, 1968. 15. ROSENBAUM, M. B.: Types of right bundle brancd block and their clinical significance. J Electrocardiol 1: 221, 1968. 16. ROSENBAUM, M. B.: Types of left bundle branch block and their clinical significance. J Electrocardiol. In press. 17. SEGERS, M.: Les facteurs de controle de la conduction intraventriculaire. Acta Cardiol 2: 256, 1947. 18. BALLARINO, M., AND RUMOLO, R.: Il Fenomeno di Luciani-Wenckebach. Milano, Editore: Recordati-Industria Chimica e Farmaceutica, 1967. 19. HANSEN, A. T.: On intraventricular conduction disturbances in the specific conduction system of the heart. Acta Med Scand 117: 104, 1944. 20. SLATER, S. R.: Partial bundle branch block: Case of three-to-one and four-to-one block. Amer Heart J 5: 617, 1930. 86 21. STENSThOM, W.: Contribution to the knowledge of incomplete bundle branch block in man. Acta Med Scand 57: 385, 1922-23. 22. STENSThOM, W.: Experimental and clinical study of incomplete bundle branch block. Acta Med Scand 60: 552, 1924. 23. ASHMAN, R.: Disturbances of the cardiac mechanism. In Clinical Electrocardiography, edited by M. Gardberg. New York, Padl B. Hoeber, Inc., 1957. ROSENBAUM ET AL. 24. BELLET, S.: Clinical Disorders of the Heart Beat. Philadelphia, Lea & Febiger, 1953. 25. KATZ, L. N., AND PIC, A.: Clinical Electrocardiography: Part I. The Arrhythmias. Philadelphia, Lea & Febiger, 1956. 26. SPANG, K.: Rhytmnusstorungen des Herzens Stuttgart, Georg Thieme Verlag, 1957. 27. WATANABE, Y., AND DREaFus, L. S.: Second degree atrioventricular block. In Mechanisms and Therapy of Cardiac Arrhythmias. New York, Crune & Stratton, Inc., 1966. Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 Circulation, Volume XL, uldy 1969 Wenckebach Periods in the Bundle Branches MAURICIO B. ROSENBAUM, GERARDO J. NAU, RAUL J. LEVI, M. SUSANA HALPERN, MARCELO V. ELIZARI and JULIO O. LAZZARI Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 Circulation. 1969;40:79-86 doi: 10.1161/01.CIR.40.1.79 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1969 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/40/1/79 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/