Survey
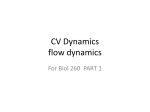
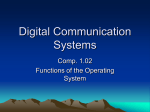
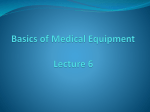
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
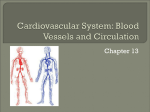
PeriPheral Arterial Disease Peripheral Arterial Disease: Evaluation, Risk Factor Modification, and Medical Management Anil Verma, MD, MPH, Amit Prasad, MD, Ghasan H. Elkadi, MD, and Yung-Wei Chi, DO Abstract • Objective: To review the evaluation and medical management of peripheral arterial disease (PAD). • Methods: Review of the literature. • Results: PAD is a highly prevalent but underrecognized and undertreated condition associated with significant morbidity and mortality. PAD is an important manifestation of systemic atherosclerosis, which reduces arterial blood to the lower extremities during exercise or rest. It has a strong association with the well-defined atherosclerotic risks factors such as diabetes mellitus, cigarette smoking, advanced age, hyperlipidemia, and hypertension and can have a varied clinical presentation. PAD can be diagnosed accurately with a comprehensive history and physical examination and simple, noninvasive, tests. Given the association of PAD with significant morbidity and mortality and multiple atherosclerotic risk factors, aggressive risk factor modification and secondary prevention strategies such as antiplatelet therapy, lipid lowering therapy, smoking cessation, diabetes control, and antihypertensive treatment should be considered in patients with PAD. Therapeutic angiogenesis using gene-based growth factors and stem cell–based therapies remain a promising future option for the treatment of PAD. • Conclusion: Clinicians should have a high index of suspicion for PAD in patients with atherosclerotic risk factors. These patients will benefit from early detection of PAD and aggressive management.[1] Peripheral arterial disease (PAD) is a common manifestation of systemic atherosclerosis and affects a significant subset of the population. Its incidence increases with known cardiovascular risk factors, and PAD commonly coexists with coronary and cerebrovascular diseases. Asymptomatic PAD is several times more common than symptomatic PAD, so the diagnosis of PAD is often overlooked. The prevalence of PAD in all patients over age 70 and diabetes patients over age 50 is approximately 29% [1]. However, only about 11% to 14% of patients are routinely screened for PAD in the primary care setting [2]. PAD is considered to be coronary 74 JCOM February 2011 Vol. 18, No. 2 heart disease equivalent but few patients undergo aggressive risk factor reduction (Figure 1). The diagnosis of PAD is important for 2 reasons. First, symptomatic PAD results in claudication, ischemic rest pain, and potential limb loss. These symptoms result in poor functional status and quality of life [3]. Secondly, atherosclerosis is a chronic, progressive, systemic disease with multifactorial etiology including hypertension, diabetes, smoking, and hyperlipidemia. However, the sensitivity and positive predictive value of these traditional variables in identifying patients at high risk for cardiovascular events is low [4]. The presence of asymptomatic PAD confers on average a 30% risk of myocardial infarction, stroke, and vascular death over 5 years [5]. Thus, early detection of PAD is fundamental to implementing early risk factor modification and disease management. Epidemiology Approximately 27 million people in North America carry the diagnosis of PAD. The distribution is the same in men and women and incidence increases with age. About 21% to 29% of patients over age 50 who have diabetes or a smoking history have PAD. Five percent of patients over age 40 with 1 or more risk factors develop PAD [6]. The most common manifestation of PAD is claudication, but fewer than 50% of patients with PAD are symptomatic [6,7]. In a study of 460 patients with PAD, 19.8% had no symptoms, 28.5% had atypical leg pain, and only 32.6% had classic claudication [6]. Risk Factors The risk factors for PAD are similar to those for coronary heart disease and include age, hyperlipidemia, hypertension, diabetes mellitus, and smoking. The strongest predictors for the development of PAD are age, diabetes, and tobacco use [8,9]. Age The incidence of PAD increases with age. The prevalence of PAD in patients over the age of 40 is approximately 4.3%. In From the Department of Cardiology, Ochsner Clinic Foundation, New Orleans, LA. www.jcomjournal.com clinical review * 90 * 80 PAD CAD 90 * 67 70 Medication use, % 88 * * 57 60 52 * 50 40 40 30 34 31 37 33 27 19 20 10 0 Statins Beta blockers ACE inhibitors Calcium inhibitors Aspirin Nitrates Figure 1. Differential medication use in patients with peripheral arterial disease (PAD) and coronary artery disease (CAD). * P < 0.001 (Adapted from Welten GM, Schouten O, Hoeks SE, et al. Long-term prognosis of patients with peripheral arterial disease: a comparison in patients with coronary artery disease. J Am Coll Cardiol 2008;51:1588–96.) patients over the age of 70 or age 50 to 69 with risk factors, the prevalence of PAD is as high as 29% [1]. Studies estimate that approximately 25% of patients over the age of 55 in a general medical practice have PAD [10]. Diabetes In the National Health and Nutrition Examination Survey (NHANES), about 26% of patients with PAD also had diabetes [11]. In population-based studies such as the Framingham Heart Study and Edinburgh Artery Study, the relative risk of developing PAD increases by 1.5 to 4 times in patients with diabetes [7, 12]. Tobacco Use Smokers have a 4 times higher lifetime risk of developing PAD than nonsmokers [7]. Tobacco use has a stronger association with PAD than CAD [7]. Former smokers have an elevated risk of PAD that is intermediate between current smokers and nonsmokers. There is, however, a reduction in mortality and critical limb ischemia in patients who stop smoking [13]. In smokers, a diagnosis of PAD is made approximately a decade earlier than in nonsmokers. Results from the www.jcomjournal.com Edinburgh Artery Study [14] found that the relative risk of intermittent claudication was 3.7 in smokers compared with 3.0 in previous smokers (who had discontinued smoking for less than 5 years). A recent 4.5-year follow-up study of over 400 patients with documented PAD demonstrated that continued smoking was the most powerful predictor of disease progression as defined by an anklebrachial index (ABI) decrease of < 0.3 [15]. Tobacco cessation slows the progression of PAD in critical limb ischemia and reduces the 10-year death rate due to vascular cause over 30% [16]. Other important risk factors for the development of PAD include hypertension, hypercholesterolemia, hyperhomocysteinemia, and elevated CRP (Figure 2) [9,17]. These risk factors are weaker predictors for the development of PAD compared with smoking and diabetes. Clinical Manifestations and Medical Evaluation Patients with PAD are frequently asymptomatic, with less than 20% of patients reporting typical symptoms of intermittent claudication of leg discomfort on exertion that is relieved with rest [18]. Frequently, these patients may presVol. 18, No. 2 February 2011 JCOM 75 PeriPheral Arterial Disease Smoking Diabetes Hypertension Hypercholesterolemia Hyperhomocysteinemia C-Reactive Protein .5 1 2 3 4 5 Relative Risk Figure 2. Risk of developing lower extremity peripheral arterial disease. The range for each risk factor is estimated from epidemiologic studies. The relative risks take into consideration current smokers vs. former smokers and nonsmokers; the presence vs. the absence of diabetes and hypertension; and the highest vs. the lowest quartile of homocysteine and C-reactive protein levels. The estimate for hypercholesterolemia is based on a 10% risk for each 10-mg/dL rise in total cholesterol. (Adapted from reference 9.) ent with atypical symptoms including leg fatigue, difficulty walking, and nonspecific leg pain. Among patients with asymptomatic PAD, about 5% to 10% develop symptoms of PAD over 5 years [1]. Clinicians should maintain a high index of suspicion when assessing patients for PAD. Complaints of lower extremity pain with findings such as hair loss, cool extremities, or poorly palpable pulses should alert the physician to conduct a thorough history and physical examination, elicit symptoms, determine the true initial and absolute claudication distances, and impact on functional capacity and quality of life. A careful assessment of atherosclerotic risk factors should be made in patients suspected of having PAD, particularly those with advanced age, diabetes, smoking, chronic kidney disease, and hyperlipidemia. Physical examination of the vascular system requires careful inspection, palpation, and auscultation. Atherosclerosis in other vascular beds should also be investigated, and it is imperative to examine the heart and neck for carotid bruit and the abdomen for an abdominal aortic aneurysm. Abnormal pedal pulses, femoral artery 76 JCOM February 2011 Vol. 18, No. 2 bruit, delayed venous filling time, cool skin, and abnormal skin color are some of the common physical findings in patients with PAD. Noninvasive Studies Ankle-Brachial Index Measuring the pressure in the ankle arteries and assessing the ABI is the initial test of choice when assessing for PAD. The ABI is a comparison of systolic blood pressure in the dorsalis pedis and/or posterior tibial arteries of the lower limb with that of the brachial artery using a continuous wave doppler device. It has a 95% sensitivity and 100% specificity [19]. ABI is simple, inexpensive, reliable, and a reproducible method of identifying PAD. The severity of PAD is indicated by a lowered ABI and is a potent predictor of cardiovascular events such as ischemic stroke, myocardial infarction and premature mortality [20]. Prevalence of PAD defined by ABI are reported to be 2.5% at 40 to 59 years of age, 8.3% at 60 to 69 years, and 18.8% at 70 to 79 years [21]. High ABI values ( > 1.3) are suggestive of medial calcification most commonly seen in patients with www.jcomjournal.com clinical review diabetes and/or with renal insufficiency [4,5]. The association between high ABI and mortality is similar to that of low ABI and mortality. Exercise treadmill testing combined with pre- and postexercise ABI can help in differentiating between claudication and pseudoclaudication. It can also provide a functional assessment of the patient with PAD and is a reliable method of detecting PAD if the resting ABI is normal but there is still a high index of suspicion of PAD. Exercise normally produces significant vasodilatation leading to increased blood flow to the extremities. This will not occur in the presence of a fixed arterial obstruction, and a significant pressure gradient develops with a subsequent fall in pressure during exercise. ABIs do not provide anatomically detailed information on specific arterial segment involvement. Anatomical information is usually provided by duplex ultrasound examination or contrast-based imaging modalities. Pulse Volume Recordings and Segmental Limb Pressures Location and extent of PAD can be further defined by segmental limb systolic pressure measurements. Doppler measurements are obtained from plethysmographic cuffs placed over the brachial artery and various points on the lower limb, including upper thigh, lower thigh upper calf, ankle, metatarsal, and digit. Segmental limb pressure measurement has the same limitations as ABI regarding noncompressibility of vessels. Segmental pressure measurements usually obtained with pulse volume recordings have a reported diagnostic accuracy of 97% [22]. Pulse volume recordings detect changes in pulse contour and can be analyzed. A normal wave form has a steep upstroke, sharp systolic peak, narrow pulse width, a dicrotic notch, and a down slope bowing to baseline [23]. It should be emphasized that a pulse volume recording constitutes a qualitative, not quantitative, study; it is less accurate than duplex ultrasound in localizing a specific lesion. Duplex Ultrasound Color-assisted duplex ultrasonography is a noninvasive and safe diagnostic modality useful in identifying and confirming the specific location, morphology, and extent of suspected PAD. It can help in delineating between stenotic and occlusive lesions and may provide functional information such as velocity gradients across stenoses. Duplex ultrasonography uses the Doppler principle in assessing the severity of arterial stenosis based on the change of measured peak systolic velocity and end-diastolic velocity. It is limited in its variability of skill of the technologist, length of the examination, body habitus, bowel gas, signal dropout due to vascular calcification, and the presence of multiple stenoses with close proximity (tandem lesions). www.jcomjournal.com Noninvasive Angiography Computerized tomographic angiography (CTA) and magnetic resonance angiography (MRA) are the recent advances in noninvasive imaging that have been rapidly embraced to define the vascular anatomy with greater speed and improved resolution. Noninvasive angiographic imaging has the advantage over invasive contrast angiography of allowing 3-D reconstruction of the images, which permits evaluation of bifurcation lesions, eccentric plaques, and areas of vessel overlap. Inherently, noninvasive imagings with CTA and MRA have less risk of vascular complication compared to invasive catheter based angiography. CTA allows acquisition of high-resolution volumetric data of vascular structure in cross-sectional images, which are then formatted into 3-D angiographic images. With the advent of 64-channel multidetector CT scanners, advantages of CTA over MRA include better patient acceptance, faster speed of scanning, better spatial resolution, and the ability to evaluate previously stented arteries and use of less contrast medium [24]. CTA is able to characterize a lesion in a multiplane view, allowing for evaluation of plaque and calcification. It is also able to visualize segments immediately distal to the arterial occlusion. CTA has been found to be diagnostically equivalent to invasive angiography in multiple studies [25]. Disadvantages of CTA include beam hardening artifacts from the vessel calcification, which makes stenosis harder to evaluate. Additionally, use of intravenous contrast is a concern in subjects with borderline renal function. MRA has advantages over CTA in that potentially nephrotoxic iodinated contrast and ionizing radiation are not required for imaging. For fear of device malfunction, patients with implantable defibrillators and permanent pacemakers may not undergo magnetic resonance studies. Gadolinium-enhanced MRA when compared with color duplex ultrasound was found to have better sensitivity for detecting arterial segments, with greater than 50% diameter stenosis (98% vs. 88%) but similar specificity (96% vs. 95%) [26]. There is current agreement between MRA and catheter angiography of 91% to 97% in diagnosing significant peripheral arterial disease [27]. The major disadvantages of MRA include higher cost, claustrophobic patients, and patients who have contraindications to MR imaging (ie, pacemaker/defibrillator). Nephrogenic systemic fibrosis, a potentially debilitating systemic disorder, has been linked with the use of gadolinium-based contrast agents, predominantly in patients with acute renal failure or end-stage renal disease [28]. Overall, both CTA and MRA are useful in patient selection and planning for endovascular and/or surgical treatment of PAD. Invasive Catheter-Based Angiography Invasive contrast angiography is considered the “gold standard” for defining both normal vascular anatomy and vasVol. 18, No. 2 February 2011 JCOM 77 PeriPheral Arterial Disease cular pathology against which all other imaging methods are compared for accuracy. It also has the added advantage of digital subtraction angiography with its enhanced imaging technique compared with unsubtracted angiography. In addition, hemodynamic consequences of the stenosis can be assessed by measuring a pressure gradient across a stenosis. Invasive contrast angiography carries the risks associated with vascular access, catheter trauma, and systemic complications associated with contrast reactions. Rates of major complications of peripheral vascular angiography range from 1.9% to 2.9% [29]. Invasive contrast angiography is now reserved for patients with PAD who are being considered for endovascular revascularization. Medical Treatment Tobacco Cessation Multiple modalities for tobacco cessation such as behavioral therapy, nicotine replacement, and medications (bupropion and varenicline) are more effective than a single modality [30]. Varenicline acts as a partial agonist at the alph-4-beta2 nicotinic acetylcholine receptor and has been associated with higher smoking cessation rates than either placebo or bupropion. Patients who smoke should be encouraged to quit smoking primarily to reduce their risk of cardiovascular events and to reduce progression of PAD. Antiplatelet Therapy Aspirin therapy for patients with PAD is widely recommended by professional society guidelines including those of the American College of Cardiology/American Heart Association and the Inter-Society Consensus for Management of Peripheral Arterial Disease [18]. The evidence for aspirin therapy in patients with coronary and cerebrovascular disease has been established by a number of large-scale trials [31], but these trials lack patients with PAD. The Antithrombotic Trialists Collaboration (ATC) was a meta-analysis that contained a subgroup of 9214 patients with PAD. There was a 22% reduction in the primary end point of vascular death, nonfatal stroke, and nonfatal myocardial infarction in patients receiving antiplatelet therapy. Remarkably, only one-third of the trials included in this meta-analysis utilized aspirin monotherapy as the antiplatelet therapy [32]. A meta-analysis of the 5 aspirin monotherapy trials in the ATC showed no significant benefit of aspirin in the reduction of the primary end point [33]. A more recent meta-analysis of 18 trials including aspirin monotherapy in patients with PAD also failed to show a statistically significant reduction in the primary end point. [34]. Larger prospective studies would be necessary to draw firm conclusions about the net clinical benefit of aspirin in patients with PAD. Clopidogrel has been used as an alternative to aspirin. This indication is based primarily on a subset of the 78 JCOM February 2011 Vol. 18, No. 2 CAPRIE trial. CAPRIE enrolled 19,185 high–cardiovascular risk patients and randomized them to receive either clopidogrel 75 mg/d or aspirin 325 mg/d. Of these, 6452 patients had PAD. After 3 years, the PAD subpopulation had a 23.8% relative risk reduction in MI, stroke, or cardiovascular death in favor of clopidogrel [35]. There is little evidence to support dual antiplatelet therapy in PAD. The CHARISMA trial had 3096 patients with PAD. These patients were randomized to dual antiplatelet therapy with aspirin 75 to 162 mg/d and clopidogrel 75 mg/ d or aspirin 75 to 162 mg/d with placebo. Dual antiplatelet therapy showed a nonsignificant reduction of 7.1% in the composite end point of death, MI, or stroke at a median of 28 months [36]. Warfarin is not indicated for PAD. The WAVE trial enrolled 2161 patients with PAD and randomized them to receive warfarin (goal INR, 2–3) with an antiplatelet agent or an antiplatelet agent alone. The warfarin group had no reduction in primary end point and had a statistically significant increase in major bleeding events [37]. Exercise Therapy Supervised exercise therapy is the first line of treatment in the management of intermittent claudication (Figure 3). A meta-analysis by the Cochrane collaboration including randomized controlled trials examining exercise training for intermittent claudication showed improved maximal walking ability by an average of 150% [38]. In addition to relieving symptoms, exercise training has prognostic implications. McDermott et al demonstrated that patients who walk 3 times weekly experienced less functional decline at 1-year follow-up [39]. Several studies have shown that patients with asymptomatic PAD have impaired walking distance and speed. This casts doubt as to whether these patients are truly asymptomatic or have adapted to reduce their exertion and minimize their symptoms [40]. Various studies have suggested that supervised exercise training may provide benefit for these “asymptomatic” patients [40]. Exercise training as a practical matter is fraught with difficulties. Patients are often not motivated to exercise since it induces pain and discomfort. Moreover, patients who were told to “go out and walk” did not derive the same benefit as those in a supervised exercise program similar to cardiac rehabilitation. Deficiencies in funding and reimbursement are the major reasons for lack of supervised exercise programs for patients with PAD [41]. Treatment of Hypertension Hypertension is strongly linked to the development of atherosclerosis and is a major risk factor for PAD. Hypertension guidelines support blood pressure lowering www.jcomjournal.com clinical review Confirmed PAD Diagnosis No significant functional disability • No claudification treatment required • Follow-up visits at least anually to monitor for development of leg, coronary, or cerebrovascular ischemic symptoms Lifestyle-limiting symptoms with evidence of inflow disease* Lifestyle-limiting symptoms Supervised exercise program Pharmacological therapy: Cilostazol (Pentoxifylline) Further anatomic definition by more extensive noninvasive or angiographic diagnostic techniques Three-month trial Endovascular therapy or surgical bypass per anatomy Three-month trial Preprogram and postprogram exercise testing for efficacy Clinical improvement: Follow-up visits at least annually Significant disability despite medical therapy and/or inflow endovascular therapy, with documentation of outflow† PAD, with favorable procedural anatomy and procedural risk-benefit ratio Evaluation for additional endovascular or surgical revascularization Figure 3. Treatment of claudication. *Inflow disease should be suspected in individuals with gluteal or thigh claudication and femoral pulse diminution or bruit and should be confirmed by noninvasive vascular laboratory diagnostic evidence of aortoiliac stenoses. †Outflow disease represents femoropopliteal and infrapopliteal stenoses (the presence of occlusive lesions in the lower extremity arterial tree below the inguinal ligament from the common femoral artery to the pedal vessels). (Adapted from reference 18.) in patients with atherosclerosis. Angiotensin-converting enzyme (ACE) inhibitors have a very important role in patients with PAD [42–45]. ACE inhibitors may increase pain-free interval and maximum walking time in patients with symptomatic PAD [46]. Beta-adrenergic blocking drugs have previously been discouraged in PAD because of the possibility of worsening claudication symptoms, but this has not been supported in the randomized controlled trials. Thus, beta-adrenergic blockers can be considered in patients with PAD [47]. Treatment of hypertension primarily involves pharmacotherapy but nondrug interventions must also be initiated in tandem; weight reduction, limited salt intake, and regular exercise play significant roles [48]. According to the Joint National Committee 7 guidelines, hypertension in PAD can be managed with any class of blood pressure– lowering agent and they advocate initial use of a diuretic in most cases [49]. Certain compelling indications such as coronary artery disease, diabetes mellitus, heart failure, www.jcomjournal.com and chronic kidney disease obligate the use of angiotensin inhibitors, beta blockers, or aldosterone antagonists as first-line agents [50]. The recommended blood pressure goal for patients with PAD is less than 140/90 mm Hg. If patient also has diabetes, the goal shifts to less than 130/80 mm Hg [49]. Treatment of Hyperlipidemia Aggressive lipid lowering is recommended in patients with existing PAD, as hyperlipidemia is known to be one of the many conventional atherosclerotic risk factors involved in the disturbance of the normal homeostatic function of the endothelium and vascular wall [51]. A subgroup analysis of the Heart Protection Study demonstrated that in patients with PAD (even in the absence of a prior myocardial infarction or stroke), aggressive low-density lipoprotein cholesterol (LDL) lowering was associated with a marked reduction in cardiovascular events [52]. PAD represents equivalent risk to that of established coronary artery disease, and aggressive Vol. 18, No. 2 February 2011 JCOM 79 PeriPheral Arterial Disease Antiplatelet activity Vasodilation Increase HDL-C Cilostazol Decrease triglycerides Inhibition of vascular smooth muscle cells Antithrombotic activity Increase blood flow Mild increase in heart rate Figure 4. Proposed effects of cilostazol. cholesterol lowering must be offered to all patients with PAD to reduce subsequent adverse cardiovascular events. The guidelines advocate lowering LDL to less than 100 mg/mL and triglyceride levels to less than 150 mg/mL with further LDL reductions to less than 70 mg/mL has also been suggested [48]. Treatment with simvastatin and atorvastatin in hypercholesterolemic patients with PAD resulted in an increase in pain-free and total walking distance as well as improved physical function compared with placebo [53,54]. The pleotropic effects of statin therapy are many; in addition to its role in lowering LDL, it increases endothelial nitric oxide production, inhibits smooth muscle migration, exerts antithrombotic and antiplatelet effect [55], and it may decrease inflammation as reflected by lower C-reactive protein (CRP) levels [56]. Patients with low CRP levels have better clinical outcomes than those with high CRP regardless of their LDL levels [57]. Thus, all patients with PAD should be on cholesterol-lowering therapy independent of baseline cholesterol levels. Treatment of Diabetes Mellitus Diabetes mellitus is a potent risk factor for PAD and systemic atherosclerosis. About 20% to 30% of PAD patients have diabetes, and this cohort has a high risk of lower limb amputation (up to 15 times more likely) as well as adverse cardiac and cerebrovascular outcomes [58]. The duration of 80 JCOM February 2011 Vol. 18, No. 2 diabetes and the degree of glycemic control are intimately linked to the risk of PAD. For every 1% rise in glycated hemoglobin (A1C), there is a 28% increase in the risk of PAD [59]. Intensive control of blood sugar effectively prevents microvascular complications, but its effects on macrovascular complications such as intermittent claudication are less definitive [60]. American Diabetes Association guidelines advocate tight glycemic control in PAD patients with diabetes, setting an A1C target of ≤ 7% [61]. Despite the association of PAD with diabetes, there is lack of evidence that there is any favorable effect of intensive glycemic control on the progression of PAD. Both the Diabetes Control and Complications Trial [62] and the United Kingdom Prospective Diabetes Study [60] found that intensive therapy was associated with a trend toward a reduction in cardiovascular events but had minimal effect on the risk of PAD. In diabetics, meticulous attention to foot care, appropriate footwear, cleansing and use of moisturizer, and inspection by patient and physicians is necessary to reduce risk of skin ulceration, necrosis, and subsequent amputation [18]. Claudication-Targeted Medical Treatment Cilostazol Cilostazol is a phosphodiesterase type 3 inhibitor that mediates a variety of physiologic responses (Figure 4) and was approved in 1999 for the treatment of intermittent claudicawww.jcomjournal.com clinical review tion. Cilostazol is a vasodilator that inhibits smooth muscle proliferation and platelet function [63]. Cilostazol has been shown to improve maximal walking distance by 40% to 60% compared with placebo after 12 to 24 weeks of therapy in patients with intermittent claudication [64,65]. Cilostazol has also found to be significantly more effective than pentoxifylline and placebo in patients with intermittent claudication [66]. The AHA/ACC guidelines have a class I recommendation for the use of cilostazol (100 mg orally 2 times/day) as an effective therapy to improve symptoms and increase walking distance in patients with lower extremity PAD and intermittent claudication (Figure 3) [18]. For those experiencing adverse effects or the elderly, a dose of 50 mg twice daily is recommended. Common side effects associated with cilostazol include headache, diarrhea, palpitations, and dizziness. Cilostazol is contraindicated in patients with heart failure because of class-associated proarrhythmic effects [67]. Pentoxifylline Pentoxifylline is a methylxanthine derivative that purportedly improves the deformability of red cells, inhibits inflammatory response, and attenuates platelet aggregation. The mechanism of pentoxifylline, however, was examined in an in vivo study and showed no improvement in red cell deformability, plasma viscosity, or fibrinogen levels [68]. A meta-analysis of 13 studies looking at the use of pentoxifylline in intermittent claudication showed that there was an increase in total walking distance of 44 m (10–67 m). There was no effect on ABIs or functional status [69]. The bulk of studies examining pentoxifylline show a mild improvement in walking distances but there is a lack of compelling evidence for the use of pentoxifylline in the treatment of intermittent claudication [70–72]. As such, it has been given a class IIb recommendation in the ACC/AHA practice guidelines [18]. Therapeutic Angiogenesis There is emerging data on therapeutic angiogenesis using angiogenic growth factors and stem cell therapy to stimulate collateral circulation in PAD. Many angiogenic agents have been used, including vascular endothelial growth factor (VEGF), hepatocyte growth factor (HGF), fibroblast growth factor (FGF), and hypoxia-inducible factor-1 (HIF-1) [73]. The Therapeutic Angiogenesis with Recombinant Fibroblast Growth Factor 2 (rFGF-2) for Intermittent Claudication (TRAFFIC) study, an early randomized trial in 190 patients with infranguinal PAD, demonstrated that rFGF-2 provides significant improvement in peak walking time and ABI [74]. The Regional Angiogenesis with Vascular Endothelial Growth Factor in Peripheral Arterial Disease (RAVE) study using intramuscular VEGF121 was negative as it did not show any differences in symptom reduction between placebo and the treated groups [75]. The hepatocyte growth www.jcomjournal.com factor plasmid provided encouraging results by demonstrating improving limb tissue perfusion as measured by transcutaneous oxygen tension (TcPO2) in the Study to Assess the Safety of Intramuscular Injection of Hepatocyte Growth Factor Plasmid to Improve Limb Perfusion in Patients with Critical Limb Ischemia (HGF-STAT trial) [76]. On the other hand, the results of a dose-ranging study of hypoxiainducible factor-alpha in a large cohort of patients randomized to 1 of 3 doses or placebo via intramuscular injection was negative [77]. Recently, the results of the NV1-FGF Gene Therapy on Amputation-Free Survival in Critical Limb Ischemia (TAMARIS) trial [78] were presented at the AHA 2010 Scientific Session. The TAMARIS trial randomized patients with critical limb ischemia unsuitable for revascularization to 8 intramuscular injections of NV1-FGF gene therapy versus intramuscular injections of placebo. Death or major amputation at 12 months occurred in 37% in the gene therapy group versus 33% in the placebo group (P = 0.48), demonstrating no benefit of from intramuscular NV1-FGF therapy. Tateishi-Yuyama et al [79] assessed the role of stem cell transplantation using bone marrow–derived progenitor cell in therapeutic angiogenesis. Improvements in measured ABI, pain-free walking distances, and transcutaneous oxygen pressure at 24 weeks were observed with intramuscular injection of bone marrow–derived progenitor cell in 22 patients with bilateral PAD. Similar efficacy and safety have been reported in uncontrolled studies of limited size where autologous bone marrow-derived progenitor cells were used, but data concerning true efficacy are still at an early stage and there is no clear evidence as to the best therapeutic cells to use in PAD [79]. Although angiogenesis using genebased growth factors and stem cell–based therapies remains a promising future option for the treatment of peripheral vascular disease, it is still at the early investigational stages. Summary PAD is a highly prevalent but underrecognized and undertreated atherosclerotic condition associated with significant morbidity and mortality. Physicians need to maintain a high index of suspicion for the diagnosis of PAD. PAD can be diagnosed accurately with a comprehensive history, physical examination, and methodologic noninvasive vascular tests. It has a strong association with the well-defined risk factors for atherosclerosis, such as diabetes, smoking, advanced age, hyperlipidemia, and hypertension. Thus, aggressive risk factor modification and secondary prevention strategies such as antiplatelet therapy, lipid lowering therapy, smoking cessation, diabetes control, and antihypertensive treatment should be considered in patients with PAD. Cilostazol improves both pain-free maximal treadmill walking distance and quality of life. Angiogenesis using gene-based growth Vol. 18, No. 2 February 2011 JCOM 81 PeriPheral Arterial Disease factors and stem cell–based therapies remains a promising future option for the treatment of PAD. Corresponding author: Yung-Wei Chi, DO, UC Davis Medical Center, Sacramento, CA 95817, [email protected]. 14. Financial disclosures: None. References 1. Hirsch AT, Criqui MH, Treat-Jacobson D, et al. Peripheral arterial disease detection, awareness, and treatment in primary care. JAMA 2001;286:1317¬–24. 2. Mohler ER 3rd, Treat-Jacobson D, Reilly MP, t al. Utility and barriers to performance of the ankle-brachial index in primary care practice. Vasc Med 2004;9:253–60. 3. Dumville JC, Lee AJ, Smith FB, Fowkes FG. The health-related quality of life of people with peripheral arterial disease in the community: the Edinburgh Artery Study. Br J Gen Pract 2004;54:826–31. 4. Ankle Brachial Index Collaboration, Fowkes FG, Murray GD, Butcher I, et al. Ankle brachial index combined with Framingham Risk Score to predict cardiovascular events and mortality: a meta-analysis. JAMA 2008;300:197–208. 5. Resnick HE, Lindsay RS, McDermott MM, et al. Relationship of high and low ankle brachial index to all-cause and cardiovascular disease mortality: the Strong Heart Study. Circulation 2004;109:733–9. 6. Regensteiner JG, Hiatt WR, Coll JR, et al. The impact of peripheral arterial disease on health-related quality of life in the Peripheral Arterial Disease Awareness, Risk, and Treatment: New Resources for Survival (PARTNERS) Program. Vasc Med 2008;13:15–24. 7. Kannel WB, McGee DL. Update on some epidemiologic features of intermittent claudication: the Framingham Study. J Am Geriatr Soc 1985:33:13–8. 8. Hiatt WR. edical treatment of peripheral arterial disease and claudication. N Engl J Med 2001;344:1608–21. 9. Dormandy JA, Rutherford RB. Management of peripheral arterial disease. TASC Working Group. TransAtlantic Inter-Society Consensus (TASC). J Vasc Surg 2000;31(1 Pt 2): S1–S296. 10. Belch JJ, Topol EJ, Agnelli G, et al. Critical issues in peripheral arterial disease detection and management: a call to action. Arch Intern Med 2003;163:884–92. 11. Selvin E, Hirsch AT. Contemporary risk factor control and walking dysfunction in individuals with peripheral arterial disease: NHANES 1999-2004. Atherosclerosis 2008; 201:425– 33. 12. Fowkes FG, Housley E, Riemersma RA, et al. Smoking, lipids, glucose intolerance, and blood pressure as risk factors for peripheral atherosclerosis compared with ischemic heart disease in the Edinburgh Artery Study. Am J Epidemiol 1992;135:331–40. 13. Jonason T, Bergstrom R. Cessation of smoking in patients with 82 JCOM February 2011 Vol. 18, No. 2 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. intermittent claudication. Effects on the risk of peripheral vascular complications, myocardial infarction and mortality. Acta Med Scand 1987;221:253–60. Fowkes FG, Housley E, Cawood EH, et al. Edinburgh Artery Study: prevalence of asymptomatic and symptomatic peripheral arterial disease in the general population. Int J Epidemiol 1991;20:384–92. Aboyans V, Criqui MH, Denenberg JO, et al. Risk factors for progression of peripheral arterial disease in large and small vessels. Circulation 2006;113:2623–9. Faulkner KW, House AK, Castleden WM. The effect of cessation of smoking on the accumulative survival rates of patients with symptomatic peripheral vascular disease. Med J Aust 1983;1:217–9. Margeta C, Giurgea A, Hammer A, et al. Impact of international guidelines on the management of cardiovascular risk factors in diabetic patients with peripheral arterial disease. Int Angiol 2009;28:175–80. Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 practice guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation 2006;113:e463–654. Bernstein EF, Fronek A. Current status of noninvasive tests in the diagnosis of peripheral arterial disease. Surg Clin North Am 1982;62:473–87. Ostergren J, Sleight P, Dagenais G, et al. Impact of ramipril in patients with evidence of clinical or subclinical peripheral arterial disease. Eur Heart J 2004;25:17–24. Criqui MH, Denenberg JO, Langer RD, Fronek A. The epidemiology of peripheral arterial disease: importance of identifying the population at risk. Vasc Med 1997; 2:221–6. Rutherford RB, Lowenstein DH, Klein MF. Combining segmental systolic pressures and plethysmography to diagnose arterial occlusive disease of the legs. Am J Surg 1979;138:211–8. Darling RC, Raines JK, Brener BJ, Austen WG. Quantitative segmental pulse volume recorder: a clinical tool. Surgery 1972;72:873–7. Mallouhi A, Rieger M, Czermak B, et al. Volume-rendered multidetector CT angiography: noninvasive follow-up of patients treated with renal artery stents. AJR Am J Roentgenol 2003;180:233–9. www.jcomjournal.com clinical review 25. Rubin GD, Schmidt AJ, Logan LJ, Sofilos MC. Multi-detector row CT angiography of lower extremity arterial inflow and runoff: initial experience. Radiology 2001;221:146–58. 26. Visser K, Hunink MG. Peripheral arterial disease: gadoliniumenhanced MR angiography versus color-guided duplex US--a meta-analysis. Radiology 2000;216:67–77. 27. Khilnani NM, Winchester PA, Prince MR, et al. Peripheral vascular disease: combined 3D bolus chase and dynamic 2D MR angiography compared with x-ray angiography for treatment planning. Radiology 2002;224:63–74. 28. Swaminathan S, Horn TD, Pellowski D, et al. Nephrogenic systemic fibrosis, gadolinium, and iron mobilization. N Engl J Med 2007;357:720–2. 29. Balduf LM, Langsfeld M, Marek JM, et al. Complication rates of diagnostic angiography performed by vascular surgeons. Vasc Endovascular Surg 2002;36:439–45. 30. Burns P, Gough S, Bradbury AW. Management of peripheral arterial disease in primary care. BMJ 2003;326:584–8. 31. Tran H, Anand SS. Oral antiplatelet therapy in cerebrovascular disease, coronary artery disease, and peripheral arterial disease. JAMA 2004;292:1867–74. 32. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ 2002;324:71–86. 33. Lechat P, Priollet P. [Prevention of major ischemic events in lower limb arterial disease: does aspirin play a role?]. J Mal Vasc 2006;31:129–34. 34. Berger JS, Krantz MJ, Kittelson JM, Hiatt WR. Aspirin for the prevention of cardiovascular events in patients with peripheral artery disease: a meta-analysis of randomized trials. JAMA 2009;301:1909–19. 35. A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events (CAPRIE). CAPRIE Steering Committee. Lancet 1996;348:1329–39. 36. Bhatt DL, Flather MD, Hacke W, et al. Patients with prior myocardial infarction, stroke, or symptomatic peripheral arterial disease in the CHARISMA trial. J Am Coll Cardiol 2007;49:1982–8. 37. Warfarin Antiplatelet Vascular Evaluation Trial Investigators, Anand S, Yusuf S, Xie C, et al. Oral anticoagulant and antiplatelet therapy and peripheral arterial disease. N Engl J Med 2007;357:217–27. 38. Leng GC, Fowler B, Ernst E. Exercise for intermittent claudication. Cochrane Database Syst Rev 2000(2):CD000990. 39. McDermott MM, Liu K, Ferrucci L, et al. Physical performance in peripheral arterial disease: a slower rate of decline in patients who walk more. Ann Intern Med 2006;144:10–20. 40. McDermott MM, Guralnik JM, Ferrucci L, et al. Asymptomatic peripheral arterial disease is associated with more adverse lower extremity characteristics than intermittent claudication. Circulation 2008;117:2484–91. 41. Bendermacher BL, Willigendael EM, Teijink JA, Prins MH. www.jcomjournal.com 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. 54. Supervised exercise therapy versus non-supervised exercise therapy for intermittent claudication. Cochrane Database Syst Rev 2006(2):CD005263. Mehler PS, Coll JR, Estacio R, et al. Intensive blood pressure control reduces the risk of cardiovascular events in patients with peripheral arterial disease and type 2 diabetes. Circulation 2003;107:753–6. Hirsch AT, Duprez D. The potential role of angiotensin-converting enzyme inhibition in peripheral arterial disease. Vasc Med 2003;8:273–8. Effects of ramipril on cardiovascular and microvascular outcomes in people with diabetes mellitus: results of the HOPE study and MICRO-HOPE substudy. Heart Outcomes Prevention Evaluation Study Investigators. Lancet 2000;55:253–9. Yusuf S, Sleight P, Pogue J, et al. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. The Heart Outcomes Prevention Evaluation Study Investigators. N Engl J Med 2000:342:145–53. Ahimastos AA, Lawler A, Reid CM, et al. Brief communication: ramipril markedly improves walking ability in patients with peripheral arterial disease: a randomized trial. Ann Intern Med 2006;44:660–4. Radack K, Deck C. Beta-adrenergic blocker therapy does not worsen intermittent claudication in subjects with peripheral arterial disease. A meta-analysis of randomized controlled trials. Arch Intern Med 1991;151:1769–76. Calhoun DA, Jones D, Textor S, et al. Resistant hypertension: diagnosis, evaluation, and treatment: a scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Circulation 2008;117:e510–26. Chobanian AV, Bakris GL, Black HR, et al. The seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA 2003;289:2560–72. Chobanian AV, Bakris GL, Black HR, et al. The seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. Hypertension 2003;42:1206–52. Kinlay S, Libby P, Ganz P. Endothelial function and coronary artery disease. Curr Opin Lipidol 2001;2:383–9. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet 2002;360:7–22. Aronow WS, Nayak D, Woodworth S, Ahn C. Effect of simvastatin versus placebo on treadmill exercise time until the onset of intermittent claudication in older patients with peripheral arterial disease at six months and at one year after treatment. Am J Cardiol 2003;92;711–2. Mohler ER 3rd, Hiatt WR, Creager MA. Cholesterol reduction with atorvastatin improves walking distance in patients with peripheral arterial disease. Circulation 2003;108:1481–6. Vol. 18, No. 2 February 2011 JCOM 83 PeriPheral Arterial Disease 55. Robinson JG, Smith B, Maheshwari N, Schrott H. Pleiotropic effects of statins: benefit beyond cholesterol reduction? A metaregression analysis. J Am Coll Cardiol 2005;46:1855–62. 56. Albert MA, Danielson E, Rifai N, et al. Effect of statin therapy on C-reactive protein levels: the pravastatin inflammation/ CRP evaluation (PRINCE): a randomized trial and cohort study. JAMA 2001;286:64–70. 57. dker PM, Morrow DA, Rose LM, et al. Relative efficacy of atorvastatin 80 mg and pravastatin 40 mg in achieving the dual goals of low-density lipoprotein cholesterol <70 mg/dl and C-reactive protein <2 mg/l: an analysis of the PROVE-IT TIMI-22 trial. J Am Coll Cardiol 2005;45:1644–8. 58. American Diabetes Association. Peripheral arterial disease in people with diabetes. Diabetes Care 2003;26:3333–41. 59. Selvin E, Marinopoulos S, Berkenblit G, et al. Meta-analysis: glycosylated hemoglobin and cardiovascular disease in diabetes mellitus. Ann Intern Med 2004;141:421–31. 60. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998;352:837–53. 61. Skyler JS, Bergenstal R, Bonow RO, et al. Intensive glycemic control and the prevention of cardiovascular events: implications of the ACCORD, ADVANCE, and VA Diabetes Trials: a position statement of the American Diabetes Association and a Scientific Statement of the American College of Cardiology Foundation and the American Heart Association. J Am Coll Cardiol 2009;53:298–304. 62. Effect of intensive diabetes management on macrovascular events and risk factors in the Diabetes Control and Complications Trial. Am J Cardiol 1995;75:894–903. 63. Chapman TM, Goa KL. Cilostazol: a review of its use in intermittent claudication. Am J Cardiovasc Drugs 2003;3:117–38. 64. Money SR, Herd JA, Isaacsohn JL, et al. Effect of cilostazol on walking distances in patients with intermittent claudication caused by peripheral vascular disease. J Vasc Surg 1998;27:267-74. 65. Beebe HG, Dawson DL, Cutler BS, et al. A new pharmacological treatment for intermittent claudication: results of a randomized, multicenter trial. Arch Intern Med 1999;159: 2041–50. 66. Dawson DL, Cutler BS, Hiatt WR, et al. A comparison of cilostazol and pentoxifylline for treating intermittent claudication. Am J Med 2000;109:523–30. 67. Nony P, Boissel JP, Lievre M, et al. Evaluation of the effect of phosphodiesterase inhibitors on mortality in chronic heart failure patients. A meta-analysis. Eur J Clin Pharmacol 1994;46:191–6. 68. Dawson DL, Zheng Q, Worthy SA, et al. Failure of pentoxifylline or cilostazol to improve blood and plasma viscosity, fibrinogen, and erythrocyte deformability in claudication. Angiology 2002;53:509–20. 69. Girolami B, Bernardi E, Prins MH, et al. Treatment of intermittent claudication with physical training, smoking cessation, pentoxifylline, or nafronyl: a meta-analysis. Arch Intern Med 1999;159:337–45. 70. Hood SC, Moher D, Barber GG. Management of intermittent claudication with pentoxifylline: meta-analysis of randomized controlled trials. CMAJ 1996;155:1053–9. 71. Ernst E. Pentoxifylline for intermittent claudication. A critical review. Angiology 1994;45:339–45. 72. Radack K, Wyderski RJ. Conservative management of intermittent claudication. Ann Intern Med 1990;113:135–46. 73. Attanasio S, Snell J. Therapeutic angiogenesis in the management of critical limb ischemia: current concepts and review. Cardiol Rev 2009;17:115–20. 74. Lederman RJ, Mendelsohn FO, Anderson RD, et al. Therapeutic angiogenesis with recombinant fibroblast growth factor-2 for intermittent claudication (the TRAFFIC study): a randomised trial. Lancet 2002;359:2053–8. 75. Rajagopalan S, Mohler ER 3rd, Lederman RJ, et al. Regional angiogenesis with vascular endothelial growth factor in peripheral arterial disease: a phase II randomized, double-blind, controlled study of adenoviral delivery of vascular endothelial growth factor 121 in patients with disabling intermittent claudication. Circulation 2003;108:1933–8. 76. Powell RJ, Simons M, Mendelsohn FO, et al. Results of a double-blind, placebo-controlled study to assess the safety of intramuscular injection of hepatocyte growth factor plasmid to improve limb perfusion in patients with critical limb ischemia. Circulation 2008;118:58–65. 77. Rajagopalan S, Olin J, Deitcher S, et al. Use of a constitutively active hypoxia-inducible factor-1alpha transgene as a therapeutic strategy in no-option critical limb ischemia patients: phase I dose-escalation experience. Circulation 2007;115:1234– 43. 78. Riferminogene pecaplasmide. Am J Cardiovasc Drugs 2010;10:343–6. 79. Tateishi-Yuyama E, Matsubara H, Murohara T, et al. Therapeutic angiogenesis for patients with limb ischaemia by autologous transplantation of bone-marrow cells: a pilot study and a randomised controlled trial. Lancet 2002;360:427–35. Copyright 2011 by Turner White Communications Inc., Wayne, PA. All rights reserved. 84 JCOM February 2011 Vol. 18, No. 2 www.jcomjournal.com