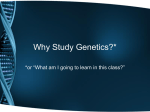
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
DECEMBER 2015 ISSUE 139 IN THIS ISSUE Moving Towards the Next Generation of Genetic Testing News from HRLMP Administration Education News News from Genetics News from Hematology NEW – EMA test for Diagnosis of HS News from Pathology Quality News Research News – Coming soon Editorial Board: Chemistry: Dr C Balion Microbiology: Dr M Smieja Pathology: Dr C Ross Genetics: Dr E. McCready Hematology: K Moffat Editorial Office: Co-Editors: Dr C Ross; K Moffat Snapshot of this edition: • • Moving Towards the Next Generation of Genetic Testing NEW - Eosin-5-Maleimide (EMA) Test for Diagnosis of Hereditary Spherocytosis HAPPY HOLIDAYS !! Moving Towards the Next Generation of Genetic Testing Since publication of the draft and completed human genome sequence in 2001 and 2004, respectively (Venter et al. 2001. Science, 291:1304-51; International Human Genome Sequencing Consortium. 2001.Nature, 409:860-921; International Human Genome Sequencing Consortium. 2004. Nature, 431:931-45), the field of genetics and genomics has experienced unprecedented growth that has led to an enhanced understanding of how both heritable and acquired genetic mutations contribute to population health. Expanding knowledge about the molecular determinants of disease has further increased the pressure on clinical genetics laboratories to provide more comprehensive testing of an increasingly broad range of genetic variants. The increasing utility of genetic testing coupled with both decreasing costs and improved through-put of next generation sequencing (NGS) technologies is driving forward a paradigm shift in laboratory genetics practices. This shift is most apparent in an increasing trend away from single gene analysis to the development of tests that enable analysis of multiple genes simultaneously. Testing of single genes can have a high diagnostic yield for disorders with specific syndromic features and/or limited “causative” mutations. For example, the beta-globin gene (HBB) is the only gene known to cause beta-thalassemia. Analysis of the HBB gene for point mutations and deletions enables the accurate molecular diagnosis of beta-thalassemia in over 99% of affected individuals. However, there is limited utility of these single analyte tests for the investigation of heterogeneous phenotypes that can be due to mutations of any one of multiple genes. Noonan syndrome, for example, is known THE EDITORIAL OFFICE WELCOMES YOUR FEEDBACK, SUGGESTIONS AND NEW IDEAS 1 Lab Connections to be caused by mutations of at least nine different genes involved in the RAS-MAPK pathway (PTPN11, SOS1, RAF1, KRAS, NRAS, SHOC2, RIT1, BRAF and CBL); PTPN11 mutation is the most common cause of Noonan syndrome but genetic testing of this gene alone only allows confirmation of the diagnosis in 50% of cases. Sequential analysis of associated genes within the differential diagnosis list can be prohibitively costly, require numerous blood draws and evoke considerable anxiety for patients who require repeated testing along their "diagnostic odyssey". Development of next generation sequencing (NGS) based assays allow testing of all nine Noonan syndromeassociated genes in a single assay. This not only improves the diagnostic yield of the test (up to ~82% of Noonan syndrome-associated alleles), but also enables detection of mutations causing other syndromes related to the RAS-MAPK pathway including cardio-facio-cutaneous, Noonan syndrome with multiple lentigines (formerly LEOPARD) and Costello syndromes (reviewed in Rauen. 2013. Annu Rev Genomics Hum Genet, 14:355-69;Tidyman and Rauen.2008. Expert Rev Mol Med, 10:e37). stochastic effects. Sensitivity and specificity of the assay can also be limited by the bioinformatics tools used to analyze and interpret the data. For example, an assay that enables sequencing of all the known proteincoding genes (exome) can return 200-400,000 variants, most of which are benign and unlikely to contribute to clinical features. Sequencing all of the known protein-coding genes provides a high degree of certainty that a “pathogenic” mutation will be sequenced, if present. As such, whole exome studies represent a powerful investigational tool, particularly when other genetic testing has been exhausted or when a specific genetic diagnosis is not apparent by clinical examination. Bioinformatic tools are used to “filter” these variants and enable a more focused analysis of variants most likely to be pathogenic . While this makes analysis of the data more streamlined and manageable, it can also result in loss of relevant data from the analysis pipeline. Therefore, while exome tests relying on these types of bioinformatic filters are extremely efficient as screening tools, their utility in ruling-out a genetic diagnosis is limited. While next generation sequencing (NGS) provides a unique opportunity to develop genetic tests for large groups of genes, it is important to note that not all NGS based tests are created equal. The two most notable factors that can influence test sensitivity and specificity include the genomic regions targeted by the test (sequence targets) and the number of times a sequence is sampled (depth of sequence coverage). Increasing the amount of genomic sequence targeted by the test will enhance the ability to detect a broader range of mutations. However, this comes at the cost of the number of times that any specific region is sampled. Low depth of sequence coverage increases the chance of false positive results due to sequencing artifacts and of false negative results or genotyping errors due to Within the HRLMP there have been a number of concerted efforts to incorporate NGS technologies into the existing workflow. Completed and ongoing test development projects are anticipated to have significant impact on the laboratory service by either introducing new tests to the menu or by improving efficiency and/or utility of existing tests. In January of this year, BRCA1- and BRCA2-associated hereditary breast and ovarian cancer became the first test that was transitioned to the new technology and has served to “pave the trail” for the development of other tests. Prior to the introduction of a NGS protocol, BRCA1 and BRCA2 were assessed by a more traditional approach that required amplification of the entire BRCA1 and BRCA2 protein-coding regions through 61 December 2015 Issue 139 independent reactions. This test was very labour intensive and required two technologists an average of two weeks to process 16 samples. Conversion of the test to NGS has streamlined the testing considerably and enables processing 24 samples with 1.5 technologists in the same period of time. The entire coding region is sequenced to a very high depth of coverage allowing for sensitivity and specificity rates approaching 100%. The high depth of coverage further enables detection of partial or whole gene deletions/duplications that may be missed using traditional sequencing protocols, thus eliminating the need for copy number evaluation using multiplex ligation-dependent amplification (MLPA). Building on the success of the BRCA1 and BRCA2 NGS test, the HRLMP is collaborating with laboratories at London Health Sciences and the Children’s Hospital of Eastern Ontario to develop NGS-based tests for pediatric and adult mitochondrial disorders due to nuclear or mitochondrial genome mutations. HRLMP has developed and validated two NGS panels for mitochondrial disorders: (1) 68 nuclear genes that are associated with adult-onset mitochondrial diseases, and (2) 37 genes from the mitochondrial genome. Both panels will be offered as part of a provincial service beginning early 2016. By restricting the number of targets to relevant genes with characterized disease associated mutations, we have been able to attain a high depth of coverage across all clinically relevant regions. This is particularly important for the analysis of the mitochondrial genome as disease-associated mutations may be present in only a small percentage of mitochondria due to heteroplasmy, and can be missed against a normal background if there is insufficient depth of coverage. The expertise developed through the hereditary breast cancer and mitochondrial projects is being directly translated in other genomics-based projects and analysis of acquired (rather than inherited) genetic mutations. A strong collaboration between the HRLMP and the Juravinski Cancer Centre Translational Research group has been particularly fruitful in pushing forward the development of NGS based companion diagnostics for solid tumours. Testing of EGFR, KRAS, NRAS and BRAF is currently available through the HRLMP as Cancer Care Ontario funded single analyte assays for specific tumours. Actionable mutations are assessed in each gene to predict patient response to targeted therapies. Conversion of the singleanalyte assays to NGS mutation panels enables streamlining of work flow and expansion of the available testing to include a broader range of clinically useful mutations. The potential for applying NGS technology to fusion gene testing and liquid biopsies is also being explored. This is an important endeavour for the laboratory as it allows further promotion of an already strong cancer genetic program and marks increasing emphasis on “personalized genomics”. Traditional cytogenetic and molecular genetic approaches continue as important tools for the investigation of both heritable and acquired genetic mutations. However, incorporation of NGS technologies into the armamentarium ensures that the HRLMP Genetics Laboratory is keeping up with the rapid pace of new age genomics. Dr. Elizabeth McCready, PhD, FCCMG, Genetics Dr. John Waye, PhD, FACMG, Genetics 2 3 Lab Connections News from HRLMP Education News News from HRLMP Administration The HRLMP’s 8th Annual Rapid Fire Showcase was held on Saturday November 21st, 2015 and was a great success again this year. There were over 100 attendees both internal to the HRLMP and external from within our LHIN and beyond. Twelve members of the HRLMP team, spanning MLAs, MLTs and management, presented eleven short oral presentations during this halfday education session. These presentations covered the wide breadth of the great work done within our HRLMP laboratories and were very well done. Thank you to all our speakers for an excellent morning of continuing education. The HRLMP is already looking forward to offering our 9th Annual in 2016! The HRLMP is pleased to announce that our Tumour Bank was recognized for the fiscal year 2014/15, and for the third year in a row, as the OTB Collection Centre with the highest number of tumours collected. Our Tumour Bank was also recognized as having the most total donors and having the fullest sets of tumours with matching blood samples across the Province. Congratulations to our Pathology team and especially our Pathology Assistants for this outstanding accomplishment! It is with great sadness that we announce that Mr. Bill Craig passed away November 22, 2015. Bill was a valued member of our Management team and joined the HRLMP in 2011 as a Supervisor, Hamilton General Core Laboratory, followed by an administrative role in Special Projects in 2014. Prior to joining the HRLMP, Bill had a well-established career in laboratory medicine. We are very fortunate to have worked with him. The HRLMP is excited to be involved in an international study that has been accepted (with minor revision) to the Journal of Clinical Microbiology. This study was collaboration at ECCMID of laboratories from the Netherlands, Italy, Canada (Quebec and Ontario (HRLMP)) and the USA. The paper describes the automated image analysis of chromogenic agar plates compared to a technologist manually reading a captured image of the plate on a monitor using WASPlab image analysis software. Mr. David Langstaff, Executive Director, CoLabs Laboratory Medicine Network, stated “Congratulations to the entire team for leading this groundbreaking work … it’s never easy being on the leading edge, but at times so rewarding!”. December 2015 Issue 139 News from Genetics test will be launched in late 2015 or early 2016. Myeloproliferative neoplasms (MPN) represent a rare group of bone disorders in which one or more blood cell type is overproduced. Affected individuals have an increased risk for transformation to acute myeloid leukemia. JAK2 and MPL have emerged as important biomarkers in three forms of MPN: polycythemia vera (PV), essential thrombocythemia (ET) and primary myelofibrosis (PMF). Mutations of these genes are identified in approximately 60% of cases negative for BCR-ABL1 fusion genes. Until recently there was little information about the molecular genetic events that drive the neoplastic process in BCR-ABL1 negative MPN cases that also lack JAK2 or MPL mutations. In 2013 whole exome sequencing efforts lead to the discovery of acquired (somatic) mutations in a new gene calreticulin (CALR) responsible for previously unexplained cases of MPN (Nangalia et al, N Engl J Med. 2013;369:2391-2405; Klampfl et al, N Engl J Med. 2013;369:2379-2390). While CALR mutations are extremely rare in PV (Broséus et al, Blood. 2014 124(26):3964-6), they are detectable in approximately 50-85% of patients with ET or PMF and no JAK2 or PML mutation (Nangalia et al., 2013; Klampfl, 2013; Rotunno et al, Blood. 2014; 123(10):1552-5). The HRLMP Molecular Oncology Laboratory is currently completing validation of CALR testing for the investigation of cases with a clinical suspicion of ET or PMF and absence of detectable JAK2 mutation. Adding CALR to our testing menu will increase diagnostic yield in MPN to up to 90%. It will also provide valuable prognostic information for MPN patients, as CALR mutations have been shown to be associated with different disease course in ET and PMF and better survival rates in PMF compared to JAK2 and MPL positive or triplenegative patients(Rumi et al, Blood. 2014 14;124(7):1062-9; ; Blood. 2014, 123(10):154451). It is anticipated that the CALR molecular Dr. Elizabeth McCready, Genetics Dr. Daria Grafodatskaya, Molecular Genetics Fellow We are pleased to announce that Kristen Wagner (MLT, Genetics) received the Margie Patterson Memorial Scholarship in Molecular Genetics from the Michener Institute’s Genetics Technology Program. The annual award is for the new graduate of the program who has demonstrated excellent technical skills in the laboratory, consistently exhibited professional behavior in both academic and health care settings, has achieved excellence in their Molecular Genetics studies, demonstrated leadership skills, shown a commitment to improving the lives of others, and illustrated the ability to work effectively both as an individual and as part of a health care team. The award was established in memory of Margie Patterson who passed away in 2005 and was a long serving technologist in genetics at HRLMP (see Hemoglobin 2006; 30:1-2). Past recipients include Robyn White (2007) and Anna Haasen (2010), both current members of the HRLMP genetics staff. Dr. John Waye, Genetics Genetics Staff Changes The HRLMP Genetics Laboratory is happy to welcome Dr. Brenda Murphy to the professional staff. Dr. Murphy brings with her considerable experience in clinical laboratory genetics service and was employed as a certified genetics technologist for several years before returning to academia to pursue graduate studies. After completing her doctoral degree, Dr. Murphy continued to demonstrate a strong interest in medical genetics and completed training in clinical 4 5 Lab Connections molecular genetics through a joint Canadian College of Medical Geneticists (CCMG) fellowship training between McMaster University, Hamilton Health Sciences and Credit Valley Hospital. She continued to be involved in Genetics and was responsible for teaching several courses with the undergraduate science program at Western University. In 2014 she completed additional CCMG Cytogenetics fellowship training at McMaster University and had been working as a Laboratory Scientist at Trillium Health Partners – Credit Valley Hospital. She joined the Genetics Laboratory in the Summer of 2015 as the Head of Cancer Cytogenomics and has been a positive addition to this service. The laboratory also welcomes Kristen Wagner as a permanent full-time technologist in the laboratory. Kristen is an awarded Genetic Technologist who has recently completed training through the Michener Institute(see article above). Her contributions have been invaluable in the Cytogenetics Laboratory. News from Hematology The times are definitely changing! For over 35 years, the smiling face of Wendy Patterson has become synonymous with excellence in morphology in the HRLMP’s Malignant Hematology laboratory at the Juravinski site. In November of this year, Wendy decided to hang up her lab coat for the final time and join the ranks of the retired. Although we are still a little shell shocked and miss her greatly, we wish Wendy well in her new life as a retiree, knowing full well that she will be successful in that endeavor (and will be able to finally sleep in after staying up late to watch the Jays and the Leafs play overtime/extra innings). With mixed emotions, the Genetics Laboratory also announces the retirement of a Molecular Genetics technologist, Ming Ye. While Ming will be missed in the laboratory, we wish her all the best in her retirement. Dr. Elizabeth McCready, Genetics A celebration tea was held Friday November 13,2015. Thanks to the many that showed up to wish her well! December 2015 Issue 139 NEW Eosin-5-Maleimide (EMA) Test for Diagnosis of Hereditary Spherocytosis A normal red blood cell (RBC) is shaped as a biconcave disc which allows the red cell to deform without damage in small capillaries and within the reticuloendothelial system, including the spleen. Hereditary spherocytosis (HS) is due to an inherited abnormality in the RBC cytoskeleton that causes RBCs to be spherical in shape. RBCs in HS lose their ability to deform and are therefore damaged in the narrow sinusoids of the spleen, resulting in a chronic hemolytic process. For the past 100 years the primary laboratory test for HS has been the Osmotic Fragility (OF) Test. OF measures the resistance to hemolysis of RBCs exposed to hypotonic solutions. If a patient’s RBCs are spherocytic, then they will be more fragile in higher salt concentrations compared to normal shaped RBCs, and thus have an increased OF. Although the OF test is very sensitive to spherocytes, it is not specific for HS, and is positive for other forms of spherocytosis (e.g. warm autoimmune hemolytic anemia). Furthermore, the results of OF are not reliable unless samples are kept cold throughout transport and tested within a twenty four hour time period. It is for these reasons the HRLMP has chosen to implement a new Flow Cytometry test for HS known as the Eosin-5-maleimide (EMA) test. In patients with HS, spherocytes have decreased binding of the EMA dye to cytoskeletal proteins, and small decreases can be detected by flow cytometry. For each test case, a batch of 6 normal controls must be run and averaged. A decrease in signal that exceeds established parameters is considered a positive result. A few very rare disorders may show reduction in EMA binding, and recent transfusions may affect results. This is a very positive process improvement for the HRLMP to eliminate a test that has been frustrating due to its labour intensive nature and lack of specificity as a measure of disease. The new EMA test is more easily standardized with increased sensitivity and specificity and can be turned around in a few hours, and will be more helpful in the accurate diagnosis of haemolytic disorders. Sample case of EMA testing for hereditary spherocytosis Dr. Madeleine Verhovsek, Hematology Dr. Cathy Ross, Pathology With thanks to Dave Kimmel, Technical Specialist, Malignant Hematology and Linda Halchuk, Senior Technologist, Molecular Hematology and Red Cell Disorders 6 7 Lab Connections Congratulations to Dr. Deborah Siegal, Clinical Scholar, Division of Hematology and Thromboembolism, and Dr. Mark Crowther for their recent publication in the New England Journal of Medicine of their study on improving the safety and decreasing the risks of new blood thinners. The study has successfully tested an antidote that reverses the effect of two new blood thinners, Apixaban and Rivaroxaban. To read this NEJM free text article, click on the link below: http://www.nejm.org/doi/pdf/10.1056/NEJMo a1510991 To read the Hamilton Spectator press release, click on the link below: http://www.thespec.com/news-story/6111530antidotes-mean-more-patients-can-take-bloodthinners/ Congratulations to Dr. John Kelton and Dr. Ted Warkentin for recently receiving the 2015 Prix Galien Canada Award, the highest award for Canadian scientists who have made significant advances in pharmaceutical research. Drs. Kelton and Warkentin have worked for more than 30 years in the diagnosis, characterization, treatment, and treatment strategies for heparin induced thrombocytopenia (HIT). To read more on this outstanding accomplishment, please click below: http://dailynews.mcmaster.ca/article/best-inthe-nation-warkentin-and-kelton-to-receiveprix-galien-canada-award/ Save the Date – Friday May 13, 2016 – 5th Multidisciplinary Hematology Education Day This educational day, to be held at the Juravinski Hospital, in the 4th floor Auditorium, provides an opportunity for Physicians, Nurses, Pharmacists and Allied Health Professionals to interact with colleagues who have expertise in treating patients with Multiple Myeloma, Myelodysplastic Syndromes/AML, Lymphoma and CLL. MOCOMP Section 1 credit will apply and a Certificate of Attendance and hours will be provided. December 2015 Issue 139 The HRLMP is pleased to announce that Karen Moffat, Technical Specialist, Coagulation, has accepted the role of Chair, Hematology Scientific Committee, Institute for Quality Management in Healthcare, effective January 1, 2016. Congratulations Karen! News from Pathology We are pleased to inform you that our Breast Assessment Centre at the Juravinski Hospital has won the 2015 Cancer Quality Council of Ontario Quality Award. Congratulations to the team for this outstanding accomplishment! To read the full article, please click on the link below: http://www.cqco.ca/awards/award_recipients_ 2015/#.Vk6G95fUmTU.gmail Canada’s first full-time female forensic pathologist, Dr. Rao, has retired after 31 years and 7700 autopsies. Dr. Rao’s contributions to forensic pathology will be remembered fondly by both the medical and the legal communities. Quality News Update from the Pre-analytical Quality Management (QM) Team The Pre-analytical QM Team was formed in September with the aim to address preanalytical gaps identified in our last IQMH (OLA) assessment. Our first project has been to try and ensure that Meditech mnemonics (HHS) or NU identifiers (SJH) are consistently recorded on specimen labels, along with the time of collection. This is being done by a multi-faceted educational program with audit and feedback to clinical educators based on specimen comments being added by HRLMP laboratory staff. The following comments are being added to specimens which have missing information: NOTIME = NO COLLECTION TIME NOCOLLID = NO COLLECTOR ID NOTIMEID = NO COLLECTION TIME AND COLLECTOR ID ILLID = ILLEGIBLE “Mom of the Morgue” – Dr. Chitra Rao The following article recently appeared on the front page of the Hamilton Spectator: the HRLMP is proud of Dr. Rao's many accomplishments; http://www.thespec.com/news-story/6160531the-mom-of-the-morgue-canada-s-first-fulltime-female-forensic-pathologist-is-retiring/ Thank you to all MLAs and MLTs who have 8 9 Lab Connections taken on the extra work of adding these specimen comments. An additional thank you to Mary Kokoski who has supplied us with audit data and to Nikki Sjoblom who has tirelessly worked to do individual education with nurses. We would also like to thank Dan Perryman, Ronda Snowdy and Audrey Stewart for providing clinical education, on behalf of the lab program, for nurses at the Annual Review for the Juravinski site this month. Cheryl Main Allahna Elahie Cathie McCallum Research News