Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
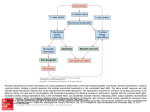
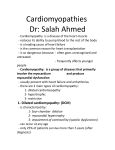
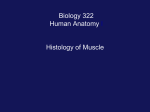
Point /Counterpoint Ventricular Myocytes Are Not Terminally Differentiated in the Adult Mammalian Heart Piero Anversa, Jan Kajstura condition of terminal differentiation, duplicate DNA, and increase in number, regardless of the disease process and the magnitude of myocardial mass. It is rather surprising that in vivo documentation of the replicative capacity of fully differentiated ventricular myocytes21 is questioned in view of the absence of mitosis in artificial in vitro preparations mostly restricted to neonatal myocytes.22–24 The logical expectation would be the opposite. This article will review available information obtained in vivo in animal models and humans favoring and opposing the belief that myocyte cellular hyperplasia is a significant component of the growth mechanisms of the overloaded heart. Terminally Differentiated Cells Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 Primary cultures of various cell types contain dividing and nondividing cells.1,2 However, nondividing cells can rest in the G0 phase and reenter the cell cycle on stimulation3–5 or become terminally differentiated and die without dividing.6 This third category of cells is not dormant in G0 and cannot reenter the cell cycle.6 For example, such a phenomenon is present in vivo at the tip of the villi of the small intestine,7 in the auditory hair cells of the ear,8 and in the upper layers of the epidermis.9 In contrast, hepatocytes in vivo are in a G0 state,10 –12 and after partial hepatectomy or severe injury, liver regeneration is accomplished by proliferation of mature hepatocytes as well as biliary epithelial cells and fenestrated endothelial cells.12 The reconstitution of liver mass is not dependent on a reserve of stem cells, which condition regeneration of bone marrow13 and skin.14 Multipotential cells have also been identified in the central nervous system, but their ability to grow, differentiate, and ultimately survive has been problematic.15 In skeletal muscle, satellite cells can be stimulated to proliferate and develop into mature myocytes, representing an additional form of tissue regeneration.16 –18 These mechanisms of cellular growth have not been considered possible in adult cardiac myocytes, and the concept was advanced that no proliferation of ventricular muscle cells occurs once cell division has ceased, shortly after birth in the mammalian heart.19 The dogma was introduced that adult cardiac myocytes are terminally differentiated cells and, therefore, cannot be recalled into the cell cycle.20,21 These cells are not in G0, cannot be triggered into the proliferative phase, but can perform their physiological functions, undergo cellular hypertrophy, and ultimately die. On this basis, in vitro preparations of neonatal cardiac myocytes22–24 and skeletal muscle cell lines25 have been used for the analysis of the molecular control of the cell cycle in an attempt to identify the key factors of terminal differentiation of myocytes. However, we will challenge the premise that myocytes cannot reenter the cell cycle, synthesize DNA, undergo nuclear mitotic division, and proliferate in vivo in the adult heart. To the best of our knowledge, there is not a single piece of evidence that this cell population is terminally differentiated in vivo. Such a contention requires the demonstration that after mitosis these cells have entered a physiological state from which they cannot be rescued by an appropriate stimulus and that they are not able to leave this History of the Terminally Differentiated Myocyte Numerous studies of the human heart from 1850 to 1911 held the view that myocardial hypertrophy was the consequence of hyperplasia and hypertrophy of existing myocytes.26 –35 However, subsequent reports from 1921 to 1925 have questioned the ability of myocytes to proliferate, suggesting that the increase in cardiac muscle mass in the pathological heart was the result of pure cellular hypertrophy.36 –38 The concept that myocytes cannot divide originated from the difficulty of identifying mitotic figures in the cells and not from any estimation of myocyte cell volume and number.38 Such a conviction has gained support from the autoradiographic analysis of [3H]thymidine incorporation in hearts of animals during postnatal development39 and after conditions of overload.40 – 42 DNA synthesis in myocyte nuclei either was not detected or was found to be essentially negligible. Although we will subsequently provide evidence to the contrary, the lack of DNA replication in cardiac myocytes experimentally with physiological growth and cardiac hypertrophy and the inability to recognize mitoses in the enlarged human heart led to the conclusion that this cell population is not in a G0 state, cannot reenter the cell cycle, and is, therefore, terminally differentiated. There are 4 issues that must be emphasized: (1) Results in animals of different species are not directly applicable to the human heart. (2) Postnatal myocardial growth is a slow physiological process that involves several maturational changes in myocytes, including differentiation and multinucleation; myocardial hypertrophy in the adult is accomplished by the growth response of mature myocytes, Received September 25, 1997; accepted April 8, 1998. From the Department of Medicine, New York Medical College, Valhalla. Reprint requests to Piero Anversa, MD, Department of Medicine, Vosburgh Pavilion, Room 302A, New York Medical College, Valhalla, NY 10595. (Circ Res. 1998;83:1-14.) © 1998 American Heart Association, Inc. 1 2 Myocyte Proliferation which is influenced by the nature and degree of the overload. (3) [3H]Thymidine labeling cannot be equated with an increase in cell number. (4) The presence or absence of cell proliferation can be determined only by counting the number of cells. We will first summarize observations concerning the changes in number and size of ventricular myocytes from birth to adulthood in humans and animals and subsequently relate how aging and pathological loads affect these cellular characteristics. Finally, evidence supporting the role of insulin-like growth factor-1 (IGF-1) in stimulating adult ventricular myocytes to reenter the cell cycle and ultimately divide will be discussed. Postnatal Myocardial Growth Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 The expansion of cardiac mass postnatally is accomplished by increases in myocyte size and number.19,43 However, the cellular changes taking place in the human heart have not been carefully defined. There is no information on myocyte volume at birth in the 2 ventricles, although the claim has been made that myocyte diameter is comparable shortly after birth in the left and right sides of the heart44,45 but that later in life left ventricular myocytes are slightly larger than right ventricular myocytes.46,47 The total number of ventricular myocytes at birth is '13109,48,49 but this parameter is extremely variable.50,51 Recently, myocyte number has been measured in the male and female human heart at 20 years of age. The male left ventricle contains 5.83109 myocytes, and the right ventricular free wall possesses 2.03109 muscle cells.46,47 Corresponding values in the female heart are 4.53109 and 1.43109 myocytes.47 These data suggest that a significant increase in myocyte number occurs in both ventricles with maturation in men and women. However, whether the process of cell proliferation persists in this 20-year period or is completed by 5 months after birth51,52 or earlier53 remains to be determined. The lack of knowledge involving the cellular mechanisms implicated in the growth of the heart during physiological cardiac hypertrophy is part of the uncertainty concerning whether ventricular myocytes in humans actually become terminally differentiated rapidly after birth. Cells are believed to be retained throughout adult life and not to be replaced if they die. Understanding why such a condition should exist in the heart is rather complex, since myocytes are continuously lost as a function of aging alone43,46,47,54 and in combination with various pathological states.54 –58 Myocyte volume markedly increases postnatally,52,59 but further hypertrophy is limited in adulthood.60 As stated in Molecular Biology of the Cell,61 “. . . it is difficult to give any reason at all” why heart muscle cells should be permanent and irreplaceable. Similar problems exist in understanding the role of myocyte hypertrophy and hyperplasia in the developing heart of the rat, the animal model most extensively investigated.43,62– 67 More limited studies have also been performed in mice.39,68,69 Two essential processes occur in the prenatal period: myocyte mitotic division and structural differentiation of the myocyte cytoplasm, involving the synthesis and organization of myofibrils and other cytoplasmic components.19,70 –72 In an attempt to evaluate the contribution of myocyte proliferation prenatally and postnatally, the extent of DNA synthesis in myo- cytes has recently been measured in rats73 and mice.69 However, the behavior of the rat heart differs from that of the mouse heart. Bromodeoxyuridine (BrdU) labeling of left ventricular myocytes involves nearly 17% of cells in the fetal rat heart at the end of gestation, decreasing to 13% one day after birth. In the adult rat heart, values of 0.2%,73 0.45%,74 0.9%,75 and 2%76 have been reported. Conversely, in the mouse, DNA synthesis is markedly reduced at birth but increases to '10% at neonatal days 4 and 5. DNA replication disappears at day 10 and remains absent later in life.69 However, Petersen and Baserga39 demonstrated in 1965 that DNA synthesis occurs in myocyte nuclei of the mouse heart, and a thymidine labeling index of 2.2% was found at 32 days of age. Lower percentages of myocyte nuclei labeling and earlier disappearance of DNA replication also have been described.77,78 The inability of myocytes to synthesize DNA may not apply to all strains of mice; a mitotic image in a myocyte of the left ventricle of a normal FVB/N mouse at 2.5 months of age is illustrated by confocal microscopy in Figure 1. Mitosis in myocytes has been detected in rats at 2 months of age as well.79 Although differences exist in the literature, the apparent contrasting observations in rats and mice have suggested opposite conclusions: myocytes maintain low levels of DNA replication in the normal adult rat heart,73–76 whereas this capacity is excluded in the adult mouse myocardium. In the latter case, it is proposed that myocyte proliferation is completed prenatally, and postnatal DNA synthesis reflects binucleation only.69 A few comments have to be made in an attempt to explain the discrepancy in magnitude and timing of DNA labeling between the rat and mouse heart. In different species, including humans, the mammalian heart varies dramatically in weight, although myocyte cell volume remains relatively constant.46,47,68,80,81 Similarly, in individual species, the greater muscle mass of the left ventricle with respect to the right ventricle is only minimally influenced by myocyte size.46,47,53,80 Myocyte cell number is the critical factor responsible for the increases in cardiac weight in larger animals. On this basis, it is reasonable to assume that heavier hearts with several-fold higher numbers of myocytes may undergo DNA replication and myocyte proliferation for longer periods of time after birth. The persistence of thymidine labeling in myocyte nuclei postnatally in the rat heart has been observed in several other studies,82– 86 indicating that mice and rats may not be identical in this cellular aspect. Moreover, caution should be exercised in the interpretation of BrdU and thymidine labeling data as indicators of the terminal differentiation of myocytes. An example is given below. Recently, the suggestion has been made that DNA replication in myocytes at day 4 and later in rats is coupled with binucleation exclusively, in the absence of cell proliferation.87 This conclusion was reached since a single injection of BrdU at day 4, when most of the cells are mononucleated, resulted in the same percentage of positively labeled myocytes at 2 hours and up to 8 days after BrdU administration. Myocyte binucleation has been claimed to be completed by day 12.87 However, the BrdU labeling index in the manner used has little to do with either binucleation or lack of cell division. Let us assume that 10 myocytes are present in the heart and that Anversa and Kajstura Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 Figure 1. Nuclear mitotic division in a myocyte nucleus from the left ventricle of a normal adult mouse heart (A to C). The nuclear membrane is lost, and cross sections of metaphase chromosomes (arrows) are illustrated by blue fluorescence of propidium iodide (A). Myocytes are recognized by the red fluorescence of a-sarcomeric actin antibody labeling of the cytoplasm (B). These two images are combined to demonstrate the localization of mitosis in a myocyte (C). Original magnification (by confocal microscopy) 32000. 2 mononucleated cells incorporate BrdU, ie, 20%. If these 2 myocytes become binucleated as do the remaining 8 cells, 2 myocytes (4 nuclei) out of 10 (20 nuclei) will be labeled, ie, 20% of the population. Consistent with the authors’ contention, BrdU staining was associated with binucleation without cell proliferation. Let us now consider that these 10 binucleated myocytes in which 2 are labeled by BrdU all divide, generating 20 cells (40 nuclei). As a consequence, 4 myo- July 13, 1998 3 cytes (8 nuclei) will be labeled, ie, 20%; this condition reflects a 2-fold increase in cell number in spite of an identical percentage of BrdU labeling. Let us now take into account a more complex situation: a population of 20 cells, 10 mononucleated and 10 binucleated in which 2 in each group are BrdU-labeled. If 50% of each cell category enter the cell cycle and mononucleated cells become binucleated and binucleated cells form new binucleated myocytes, the results are as follows: 5 mononucleated myocytes with 1 stained by BrdU and 20 binucleated myocytes with 4 stained by BrdU. Again, 5 BrdU-labeled cells out of 25 equals 20% of labeling in the presence of a 25% myocyte proliferation. It is relevant to emphasize that these calculations correctly consider that BrdU-labeled myocytes behave in a manner identical to unstained cells. Importantly, the claim has been made that the consistency in the fraction of myocytes labeled by BrdU over time is a demonstration of the lack of cell division, whereas an increase in labeling index would be indicative of cell multiplication.87 The latter implies that BrdU, per se, can trigger a cell to reenter the cell cycle and undergo cytokinesis. As stated in Baserga’s book in 1985,6 “cell proliferation means that cells are dividing, and the only way to determine the number of cells . . . is to count them.” Additionally, DNA synthesis in myocyte nuclei in the rat heart does not end at day 12, when binucleation is completed. Results from our laboratory in the same strain of Sprague-Dawley rats have shown a 0.52% labeling index at 3 weeks,73 and values of 1.5% and 0.58% have been reported from Clubb and Bishop67 for the left and right ventricles of Fischer 344 rats at the identical age. Quantitative analyses of the changes in myocyte number in the heart of Wistar and Sprague-Dawley rats with maturation are rare; the results are variable; and the differences are, at times, difficult to explain.86 –92 However, the major increases in cell number appear to occur in the early postnatal period, a phenomenon that may also apply to the mouse heart.68,93 The contradictory observations may reflect, at least in part, the limitations inherent in the methodologies used and instrumentation available at the time of these investigations. Additionally, not a single experiment examined the changes in myocyte cell volume and number at different time points during postnatal development and in the adult heart simultaneously. The number of myocytes in the right ventricle achieves an adult value almost immediately after birth,88 and numerous studies have examined the entire heart, neglecting the possibility of regional differences in myocyte proliferation. The deficiencies in the in situ morphometric techniques involve several factors: (1) The presence of multinucleated myocytes could not be detected in histological sections, affecting the recognition of the various cell populations in situ.94 (2) Neither the percentage of myocardium occupied by mononucleated and multinucleated myocytes nor the relative contribution of each cell category to the aggregate myocyte mass could be determined.81 (3) In situ determinations of cell volume were restricted to myocyte volume per nucleus, and cell number was based on the measurement of the total number of nuclei in the ventricle.94 (4) The enzymatic dissociation of myocytes, which allows evaluation of the 4 Myocyte Proliferation Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 percentages of mononucleated and multinucleated cells,64 was not used in early studies.88 Problems also exist in the assessment of myocyte volume of isolated cells by Coulter counter from which cell number was calculated: (1) A cell suspension is run through the machine, and the distribution curve generated by the computer requires that an arbitrary gate be introduced by the observer to establish what will be considered a reliable value of cell volume. This approach results in the exclusion of small and large myocytes, introducing a bias factor, defeating the principle of morphometry. (2) Fragments of myocytes, comparable in volume to an assumed acceptable cell size, are included in the estimation of this parameter. Aggregates of interstitial cells are commonly present at this stage, further weakening the validity of this technique. (3) Coulter counter data do not provide information regarding the volume of mononucleated and multinucleated cells, which is critical for assessment of the total number of myocytes in the ventricles. In summary, whether an increase in cell number occurs in the myocardium in the later phases of postnatal development remains to be determined. Future studies applying morphometric methodologies in situ in combination with myocyte isolation and confocal microscopy68,81,95 will enable us to establish whether cell division is a critical aspect of the maturation of the heart. However, the question whether myocytes become terminally differentiated shortly after birth, ie, cannot reenter the cell cycle, may be negatively answered. DNA synthesis and nuclear mitotic division persist in the adult mammalian heart. The apparent discrepancies between the ability of myocytes to divide and the quantitative results may reflect ongoing cell dropout with aging and the possibility of a slow continuing turnover of old dying myocytes and new cells. Aging of the Myocardium According to the dogma, the number of muscle cells in the mammalian heart is defined at birth, and in the absence of cardiac disease, these myocytes persist throughout the life of an individual or animal. Men and women of 100 years of age and older are present in our society, and nobody dies without a heart. The inevitable implication of the dogma is that myocytes are immortal. Alternatively, myocytes may not live indefinitely, they may have a predetermined life span, and the heart may be characterized by ongoing cell loss and cell regeneration during the entire life of a human being or an animal. We will summarize available information supporting the concept that myocyte death occurs with aging; more complex is recognizing whether cell renewal accompanies the progression of life in the normal heart. In the last 25 years, numerous investigations have been performed to identify the pathophysiological bases responsible for the diminished ability of the aged heart to sustain increases in pressure and volume loads.58,96 –100 Moreover, the adaptation of the coronary vasculature and microvasculature with aging has been characterized functionally and structurally.43,54,96,101–103 Effort has also been made to identify the molecular mechanisms implicated in the limitations of the aged heart to adapt to stressful conditions.104,105 However, to the best of our knowledge, there are only 2 studies in which the alterations in the number of ventricular myocytes with aging alone have been measured in the male46,47 and female47 human heart. In the male heart, from 17 to 89 years of age, the absolute number of myocytes decreases by 45 million per year in the left ventricle and by 19 million per year in the right ventricle. In contrast, the number of myocytes in the left and right ventricles remains essentially constant in women from 20 to 95 years of age. Myocyte loss in the male heart is associated with hypertrophy of the remaining cells. Cell volume is not altered in women. Importantly, the etiology of myocyte death in the aging human heart remains to be determined. The bases for the differential effects of aging on ventricular myocytes in men and women are currently unknown. Although cardiovascular events in women increase after menopause,100,106 sex hormones do not appear to influence myocyte loss with aging. The number of myocytes in the myocardium does not decrease in women from 55 to 95 years.47 It is surprising that no information is available concerning the influence of gender on the volume composition of the myocardium and quantitative structural properties of the capillary network controlling tissue oxygenation as a function of aging. However, apoptosis of myocytes occurs in both men and women under pathological conditions,107–110 suggesting that the female heart is not protected from this form of cell death. Similarly, cell necrosis is present in women with ischemic cardiomyopathy.111,112 It is unlikely that cell death is not a component of the aging female heart. Conversely, the hypothesis may be advanced that the regenerative capacity of myocytes is greater in women, maintaining the number of myocytes constant. Additionally, when normal aging is not distinguished from the superimposition of hypertension, valvular disorders, diabetes, amyloidosis, and ischemic heart disease, which all increase in the elderly,113 no difference is detected between the sexes, and cardiac weights increase up to 110 years of age.114 The inclusion of myocardial hypertrophy of various origin in the study of the aging heart has indicated that the number of myocytes does not change in the left and right ventricles up to 90 years.51,115 These apparent contradictory observations are difficult to explain. However, the suggestion can be made that myocyte proliferation may occur in the hypertrophied ventricles,116 masking the phenomenon of cell loss. In view of the difficulty in identifying the mechanisms of myocyte loss and the potential of cell proliferation in the human heart with age, these cellular processes have been studied in aging male Fischer 344 rats. In this strain and sex, cell death has been detected as early as 3 months after birth in the left and right ventricles. However, myocyte necrosis and apoptosis are both present in the left ventricle, whereas myocyte necrosis exclusively affects the right ventricle.117 This distinction in the forms of cell death between the ventricles persists throughout life. Myocyte death increases with age, but a reduction in the total number of myocytes of nearly 19% occurs biventricularly only at 12 months.118 Myocyte number in the left ventricle does not change from 12 to 29 months, and a 1.8-fold increase takes place in the right ventricle during this interval. The preservation of the aggregate number of muscle cells in the left and the increase in the right ventricle with age occur in spite of the concurrent loss of myocytes in the entire heart.117 Myocyte death and regen- Anversa and Kajstura July 13, 1998 5 Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 Figure 2. A and B, DNA synthesis in a myocyte nucleus from the left ventricle of a male 4-month-old Fischer 344 rat. Bromodeoxyuridine labeling of the nucleus is shown by green fluorescence (A), and the localization of the bromodeoxyuridine-stained nucleus in the myocyte is illustrated by a combination of phase-contrast microscopy and bisbenzimide fluorescence (B). Arrows indicate the labeled nucleus. Small fluorescence dots in panel A correspond to lipofuscin. C and D, Nuclear mitotic division in a myocyte nucleus from the left ventricle of a male 4-month-old Fischer 344 rat. Metaphase chromosomes (arrows) are shown by bisbenzimide fluorescence (C), and myocytes are recognized by the red fluorescence of a-sarcomeric actin labeling of the cytoplasm (D). Arrowheads indicate nondividing myocyte nuclei. Original magnification 31200 (A and B) and 31400 (C and D). eration are easily identified in adult rats at 3 to 4 months, since not only are apoptosis and necrosis present, but BrdU labeling and nuclear mitotic division are also observed in these cells (Figure 2). Ventricular dysfunction and failure in this model become apparent at 24 to 29 months,97,98,117,118 minimizing the role of hemodynamic factors in cell death and proliferation in young animals. Thus, adult myocytes are not immortal and may have a predetermined life span, and new cells can be made by mitotic division. However, whether old cells are more predisposed to die cannot be established at present. There are no markers of myocyte aging, and the acquisition of tools capable of discriminating senescent from young cells99,119 may be a major challenge of future research. The combination of cell death, DNA replication, and myocyte nuclear mitotic division is not restricted to Fischer 344 rats. BrdU labeling of myocyte nuclei73–75 and mitotic images are characteristic aspects of male Sprague-Dawley rats as well.79 Mitoses in adult myocytes79 and cell loss80 have been reported in this strain, suggesting that a balance between cell growth and cell death may be present in adult animals. In this model, as in the Fischer rat, myocyte cell loss precedes the occurrence of ventricular dysfunction.80 These experimental findings and the results in humans are consistent with the contention that myocyte cell death is a typical feature of the detrimental effect of aging on the male mammalian heart. Additionally, a slow rate of myocyte turnover may be implemented in the rat heart, but no information is available to indicate that a similar phenomenon occurs in humans. Whether sex differences are important variables that influence the susceptibility of myocytes to die and regenerate in adulthood and aging is currently unknown. Although heart failure is a disease of the elderly, with 3.2 million patients older than 65 years of age,120 the results discussed above46,47 do not support the concept that aging, per se, leads to an impairment in pump performance. In the population examined, stringent criteria for inclusion were followed, excluding all hearts with any form of functional or histologically detectable myocardial damage.46,47 However, whether heart failure in an aged individual is always attributable to a secondary disease of the myocardium and coronary vasculature or whether, at times, aging may be regarded as the primary cause of the abnormality in cardiac hemodynamics remains to be determined clinically. This is a relevant issue, since heart failure is the major cause of death in the elderly.58 Moreover, severe ventricular dysfunction develops in Fischer 344 rats late in life97,98,117,118; this deleterious impact of aging in the animal model is characterized by a high level of mitosis and myocyte proliferation.80,121 Flow cytometric analyses of DNA content in myocyte nuclei have been consistent with these results.122 Preliminary observations by confocal microscopy of BrdU-labeled myocyte nuclei in the tissue and mitoses in isolated myocyte preparations confirm active DNA replication (Figure 3) and nuclear mitotic division (Figure 4) in aged animals. Conversely, it is not clear 6 Myocyte Proliferation Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 Figure 3. DNA synthesis in myocyte nuclei from the left ventricle of a male 27-month-old Fischer 344 rat. Bromodeoxyuridine labeling of nuclei (arrows) is shown by the green fluorescence (A and D), and myocytes are identified by the red fluorescence of a-sarcomeric actin staining of the cytoplasm (B and E). These images are combined in panels C and F. Original magnification (by confocal microscopy) 32000 (A to C) and 31400 (D to F). whether these findings in male Fischer 344 rats are actually applicable to the aged, senescent, failing human heart. Heart Failure The possibility that cardiac hypertrophy in humans is the result of myocyte hypertrophy and hyperplasia was advanced .40 years ago by Linzbach.45,60 The critical heart weight theory introduced by this author in the late 1940s and early 1950s has suggested that, in the presence of a cardiac weight of $500 g, myocyte proliferation begins and that this cellular process constitutes the prevailing mechanism of additional growth of the heart.116 These findings were restricted to the left ventricle, but subsequent observations have demonstrated that a similar response occurs in the right ventricle.123 The Anversa and Kajstura July 13, 1998 7 Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 Figure 4. Metaphase chromosomes (arrows) in a binucleated myocyte are shown separately by blue fluorescence in panels A and D and in combination in panel G. Myocytes are recognized by the red fluorescence of a-sarcomeric actin labeling of the myofibrils located at the periphery of the cell. The empty area in the center corresponds to undifferentiated cytoplasm (B, E, and H). Arrows in these 3 panels point to the localization of metaphase chromosomes. These images are combined in panels C, F, and I. The 2 nuclei undergoing mitosis were 11 mm apart. Original magnification (by confocal microscopy) 31400. existence of myocyte proliferation in the human heart was challenged in 1972,51,115 but several more recent studies have confirmed Linzbach’s results.50,124 –130 However, the morphometric data supporting cellular hyperplasia have been based mostly on the assumption that myocytes are mononucleated cells and that an increase in the total number of myocyte nuclei in the ventricle corresponds to an identical increase in the aggregate number of cells in the heart. Different proportions of mononucleated and multinucleated myocytes may be present in the myocardium during normal and pathological 8 Myocyte Proliferation Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 states, and this raises the question of the distinction between nuclear hyperplasia without cytokinesis, ie, increased number of nuclei per cell, and cellular hyperplasia, ie, increased number of myocytes. This critical issue has recently been addressed by examining the distribution of nuclei in myocytes isolated from 72 normal and 176 pathological hearts.130 Aging, cardiac hypertrophy, and ischemic cardiomyopathy do not change the fraction of mononucleated and multinucleated myocytes in the ventricular myocardium. The documentation that conditions of overload, aging, and ischemic heart disease do not alter the relative proportion of the various myocyte populations130 strongly suggests that the demonstrations of myocyte cellular hyperplasia obtained initially by Linzbach45,60 and subsequently by other investigators50,124 –130 are valid. Additionally, mononucleated cells represent 3/4 of the myocytes of the human heart, differing significantly from other mammals, such as mice,68 rats,64 and dogs.81 Whether this cellular characteristic may influence the ability of myocytes to reenter the cell cycle and ultimately divide is currently unknown. Similarly, it is not clear whether the massive cardiac hypertrophy that can be achieved in the human heart116,125,130 is related, at least in part, to the high percentage of mononucleated myocytes. Heart weight in humans may increase 3-fold, reaching values of $1000 g.60,116,125,130 Decompensated eccentric hypertrophy in humans is characterized by increases in myocyte number that vary from 20% to .100%.60,116,123–130 This phenomenon does not seem to be affected by aging,129 although difficulties exist in establishing whether myocyte proliferation in the aged pathological heart occurred at a younger age. In an analysis of 7112 human hearts from birth to 110 years of age, Linzbach114 has shown that extreme forms of cardiac hypertrophy are detectable up to the ninth decade of life, and heart weights of 500 and 600 g are present in patients at 100 years and older. The morphometric results in the human heart have been questioned repeatedly, and the ability of adult myocytes to undergo hyperplasia has been a matter of controversy for several decades and still persists in the scientific community. The bases for the opposition to these quantitative findings are difficult to understand because the issue of the existence or absence of an increase in the number of myocytes in the hypertrophied decompensated human heart can be addressed only by morphometric methodologies. There is no alternative technique that can be used. Moreover, scar formation and myocyte loss are typical aspects of cardiac failure, suggesting that the measurements of myocytes in the pathological heart are underestimations of the actual number of cells that has been formed in the course of the disease. Cell death by apoptosis is present in the terminal phases of heart failure,108,110 and this ongoing process, distinct from myocyte necrosis and tissue fibrosis,131 further affects the aggregate number of cells in the ventricle. This may not be the case when cardiac hypertrophy is in its compensated stage.132 We will now consider the determinant factor on which the dogma that ventricular myocytes are terminally differentiated cells was based in 1925.38 As indicated earlier, this consisted of the inability to detect mitotic figures in myocytes of hypertrophied hearts. However, in the last few years, such documentation has been obtained in patients affected by acute and chronic intractable cardiac failure,21,133 and a new example is illustrated in Figure 5. For the first time, a mitotic index has been measured.133 The demonstration that 11 myocyte nuclei per 1 million cells, or 59 000 nuclei in the entire left ventricle, exhibit mitotic images in the failing heart may explain why difficulties exist in identifying mitoses with routine microscopic sampling. Moreover, in most cell systems, the 4 phases of mitosis are completed in 1 hour.6 Since there is no logical reason to assume that the duration of mitosis is different in myocytes, the chances of its detection in this cell population are extremely limited. The impossibility of seeing prophase in tissue sections may reduce further our time of recognition of mitosis. However, the low frequency of mitosis should not suggest that this cellular process is of minor importance in the generation of new muscle cells: in a 45-year-old man with 5.23109 nuclei in the left ventricle,47 a mitotic index of 11 nuclei per 106 and a mitotic time of 1 hour will generate 10% new myocytes in 1 year and almost double, 1.96-fold, the entire number of ventricular myocytes over a period of 10 years. These calculations assume that myocytes divide only once and are consistent with quantitative results in the severely hypertrophied human heart.60,116,124,125 Experimentally, results concerning the terminal and nonterminal differentiation of ventricular myocytes in the adult heart have been contradictory. Initial observations in the late 1960s and early 1970s challenged not only the existence of myocyte proliferation but also the sequence of events postulated by Linzbach45,60,116 in which myocyte hyperplasia was regarded as a late response of the myocardium preceded by cellular hypertrophy. This is because short-term cardiac hypertrophy in the rat is characterized by enlargement of preexisting myocytes with little or no DNA synthesis in myocyte nuclei, possibly representing polyploid cells.40 – 42 However, these studies neglected the role of time and the condition of the overload. It is rather surprising that no functional measurements were obtained in these and more recent investigations to establish whether ventricular dysfunction and failure were present in the animal models. In the absence of these criteria, comparisons with the decompensated human heart are impossible. The magnitude of the hemodynamic stress may be the most critical variable in the initiation of myocyte hypertrophy or hyperplasia in the pathological heart. After a gradual and moderate increase in workload on the heart, myocyte cellular hypertrophy predominates,41,42,65,134 –136 whereas a severe increase in ventricular loading, acute and chronic in nature, may engender DNA synthesis, mitosis, and myocyte proliferation.83,86,137–139 DNA replication and mitotic divisions in myocytes are apparent in the decompensated postinfarcted rat heart (Figure 6). Moreover, quantitative analysis in rats86,118 and dogs81,139 has documented that the number of nuclei per cell does not change in the failing heart, indicating that increases in the number of myocyte nuclei in the ventricle correspond to identical increases in myocyte number. Similarly, nuclear mitotic divisions reflect the generation of new myocytes. These conclusions are in contrast with observations in the mouse Anversa and Kajstura July 13, 1998 9 Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 Figure 5. Mitotic figure in a left ventricular myocyte of a patient affected by ischemic cardiomyopathy. Metaphase chromosomes (arrows) are illustrated by blue fluorescence (A). Myocytes are recognized by the red fluorescence of a-sarcomeric actin antibody labeling of the cytoplasm (B). These 2 images are combined to demonstrate the localization of mitosis in a myocyte (C). Original magnification (by confocal microscopy) 31400. heart, in which isoproterenol-induced cardiac hypertrophy did not show DNA replication in myocyte nuclei.140 This apparent discrepancy may be due to the preservation of function in this model. Conversely, BrdU labeling of myocyte nuclei is present in the surviving myocardium after infarction and ventricular failure in the mouse (not shown). In this regard, cyclin D1 overexpression in myocytes in vivo is coupled with DNA synthesis and multinucleation.141 Whether these transgenic mice are characterized by myocyte proliferation remains to be determined. Increases in the number of myocytes in the overloaded rat heart vary from 20% to 45%.86,89,118 These values are lower than those detected in humans but may be influenced by the simultaneous occurrence of myocardial damage and cell death. Myocyte loss complicates the estimation of the real number of newly formed myocytes in the ventricle; myocyte loss results in an underestimation of myocyte cellular hyperplasia, whereas myocyte hyperplasia leads to an underestimation of the magnitude of myocyte death in the myocardium. Thus, myocyte proliferation may be obscured by myocyte loss, and the measurement of cell number may not provide evidence of cell regeneration. This seems to be the case in the failing left ventricle of rats after coronary artery constriction86 and of dogs after ventricular pacing.81,139 Prolonged systemic hypertension in rats is associated with cellular hyperplasia142,143 in spite of diffuse tissue injury.143 10 Myocyte Proliferation Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 Figure 6. Nuclear mitotic divisions in myocytes located in the region adjacent to (A and B) and distant from (C and D) the infarcted portion of the left ventricle in rats 7 days after coronary artery occlusion. Late prophase with the appearance of chromosomes and loss of nuclear membrane is apparent in panels A and B. Metaphase chromosomes are evident in panels C and D. Mitoses are shown by blue fluorescence, and myocytes are identified by the red fluorescence of a-sarcomeric actin antibody labeling of the cytoplasm. Original magnification (by confocal microscopy) 31400. IGF-1 and Myocyte Growth Several studies from our laboratory have raised the possibility that the reentry of myocytes into the cell cycle occurs in the adult rat heart in the presence of cardiac failure.86,118,143 Such a response of the overloaded heart is characterized by the stimulation of IGF-1 and IGF-1 receptors in the cells, which precedes the expression of late growth-related genes, DNA replication, myocyte nuclear mitotic division, and cell division.86,137,138,144 Moreover, the quantity of cyclins E, A, and B and cyclin-dependent kinases, cdk2 and cdc2, is enhanced in combination with their associated histone H1 kinase activity.145 These latter observations are consistent with the con- tention that myocytes can synthesize nuclear proteins, modulating the progression of these cells through the cell cycle and mitosis. Conversely, the suggestion has been made that cyclin A disappears during early postnatal life in the rat, becoming undetectable by day 14 after birth.146 Such a phenomenon has been implicated in the permanent withdrawal of myocytes from the cell cycle. The discrepancy between these results is difficult to explain, because the lack of this cyclin has been claimed after analyzing tissue samples that contain fibroblasts and endothelial cells that actively proliferate with maturation.73 Additionally, numerous reports have shown the persistence of low levels of DNA replication Anversa and Kajstura July 13, 1998 11 of myocyte volume and number or of indices of cell proliferation. Importantly, mice overexpressing IGF-1 characteristically show an attenuation in ventricular dilation and myocardial loading after infarction,154 but whether this beneficial effect is mediated by the increased number of ventricular myocytes and/or reduction of myocyte death in the surviving myocardium remains to be determined. Acknowledgments Figure 7. Effects of postnatal maturation on the aggregate number of myocytes in the heart of wild-type (open bars) and IGF-1 transgenic (solid bars) mice. Results are presented as mean6SD. d indicates days of age. *P,0.05 vs corresponding value in wild-type mice. Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 in adult myocytes.73–75 Attenuation of the IGF-1–IGF-1 receptor autocrine system in the cells appears to be coupled with the decline in myocyte proliferation with cardiac development.73,147 The in vivo results suggesting a potential link between IGF-1 and multiplication of myocytes have not been paralleled by similar observations in vitro. Culture studies of adult myocytes have documented that IGF-1 activates DNA synthesis148,149 and the expression of structural proteins, which are consonant with a hyperplastic and hypertrophic response of these cells.148 Moreover, IGF-1 increases the formation of myofibrils only in long-term cultures of matured myocytes.150 When myocytes surviving an acute myocardial infarction are stimulated by IGF-1 in vitro, the quantities of cyclin D1, E, A, and B are upregulated, and this adaptation may reflect the increase in IGF-1 receptors on the cells.149 Cyclin D1, E, and A kinase activity also increases, but cyclin B kinase activity is not enhanced by IGF-1. Concurrently, DNA replication in myocyte nuclei is detected, whereas mitotic division is not observed. Several phenomena may be involved in this block of the cell cycle in vitro. Myocardial loading may be critical for the progression of myocytes through mitosis, and mechanical forces are abolished in culture. Alternatively, other growth factors may be implicated in combination with IGF-1 in the regulation of mitosis in this cell population. To characterize more directly the growth-promoting effect of IGF-1 on myocytes in vivo, transgenic mice have been obtained in which the cDNA for the human IGF-1B was placed under the control of a rat a-myosin heavy chain promoter.68 In mice heterozygous for the transgene, the aggregate number of myocytes in the heart is identical to that in nontransgenic littermates at birth but increases 21%, 31%, and 55% at 45, 75, and 210 days of age (Figure 7). This increase in cell number involves mostly binucleated myocytes. By use of confocal microscopy, the average volume of mononucleated, binucleated, trinucleated, and tetranucleated myocytes has been measured for the first time. Overexpression of IGF-1 appears to have no influence on cell volume, further suggesting that this growth factor sustains cell division in myocytes of the adult heart. These results are in contrast with the contention that IGF-1 induces only cellular hypertrophy in vivo in the overloaded heart.151–153 This conclusion has been reached in the absence of any measurements This study was supported by grants HL-38132, HL-39902, HL43023, and AG-15746 from the National Institutes of Health and by a Grant-in-Aid from the American Heart Association (No. 950321). The expert technical assistance of Maria Feliciano is greatly appreciated. References 1. Ham RG. Clonal growth of mammalian cells in a chemically defined, synthetic medium. Proc Natl Acad Sci U S A. 1965;53:288 –293. 2. Loo DT, Fuquay JI, Rawson CL, Barnes DW. Extended culture of mouse embryo cells without senescence: inhibition by serum. Science. 1987;236:200 –202. 3. Brooks RF. Regulation of the fibroblast cell cycle by serum. Nature. 1976;260:248 –250. 4. Mercer WE, Schlegel RA. Cell-cycle re-entry of quiescent mammalian nuclei following heterokaryon formation. Exp Cell Res. 1980;128: 431– 438. 5. Rao PN, Smith ML. Differential response of cycling and noncycling cells to inducers of DNA synthesis and mitosis. J Cell Biol. 1981;88: 649 – 653. 6. Baserga R. The Biology of Cell Reproduction. Cambridge, Mass/ London, England: Harvard University Press; 1985:chaps 1, 2, and 4. 7. Fry RJM, Lesher S, Kisieleski WE, Sacher G. Cell proliferation in the small intestine. In: Lamerton LF, Fry RJM, eds. Cell Proliferation. Oxford, UK: Blackwell; 1963. 8. Richardson G. Hair-cell regeneration: keep the noise down. Curr Biol. 1993;3:759 –762. 9. Iversen OH, Bjerknes R, Devik F. Kinetics of cell renewal, cell migration and cell loss in the hairless mouse dorsal epidermis. Cell Tissue Kinet. 1968;1:351–356. 10. Grisharn JW. A morphologic study of deoxyribonucleic acid synthesis and cell proliferation in regenerating rat liver: autoradiography with thymidine-H3. Cancer Res. 1962;22:842– 849. 11. Fabrikant JI. The kinetics of cellular proliferation in regenerating liver. J Cell Biol. 1968;36:551–565. 12. Michalopoulos GK, DeFrances MC. Liver regeneration. Science. 1997; 276:60 – 65. 13. Prockop, DJ. Marrow stromal cells as stem cells for nonhematopoietic tissues. Science. 1997;276:71–74. 14. Martin P. Wound healing: aiming for perfect skin regeneration. Science. 1997;267:75– 81. 15. McKay R. Stem cells in the central nervous system. Science. 1997;276: 66 –71. 16. Mauro A. Satellite cell of skeletal muscle fibers. J Biophys Biochem Cytol. 1961;9:493– 497. 17. Snow MH. Myogenic cell formation in regenerating rat skeletal muscle injured by mincing, I: a fine structural study. Anat Rec. 1977;188: 181–200. 18. Snow MH. Myogenic cell formation in regenerating rat skeletal muscle injured by mincing, II: an autoradiographic study. Anat Rec. 1977;188: 201–218. 19. Zak R. Development and proliferative capacity of cardiac muscle cells. Circ Res. 1974;35(suppl II):II-17–II-26. 20. Anversa P, Kajstura J, Cheng W, Reiss K, Cigola E, Olivetti G. Insulin-like growth factor-1 and myocyte growth: the danger of a dogma, I: postnatal myocardial development: normal growth. Cardiovasc Res. 1996;32:219 –225. 21. Anversa P, Kajstura J, Cheng W, Reiss K, Cigola E, Olivetti G. Insulin-like growth factor-1 and myocyte growth: the danger of a dogma, II: induced myocardial growth: pathologic hypertrophy. Cardiovasc Res. 1996;32:484 – 495. 22. Sen A, Dunnmon P, Henderson SA, Gerard RD, Chien KR. Terminally differentiated neonatal rat myocardial cells proliferate and maintain 12 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. 54. Myocyte Proliferation specific differentiated functions following expression of SV40 large T antigen. J Biol Chem. 1988;263:19132–19136. Thorburn A, Thorburn J, Chen S-Y, Powers S, Shubeita HE, Feramisco JR, Chien KR. HRas-dependent pathways can activate morphological and genetic markers of cardiac muscle cell hypertrophy. J Biol Chem. 1993;268:2244 –2249. Kirshenbaum LA, Schneider MD. The cardiac cell cycle, pocket proteins, and p300. Trends Cardiovasc Med. 1995;5:230 –235. Gu W, Schneider JW, Condorelli G, Kaushal S, Mahdavi V, NadalGinard B. Interaction of myogenic factors and the retinoblastoma protein mediates muscle cell commitment and differentiation. Cell. 1993;72: 309 –324. Köllicker A. Handbuch der Gewebelehre. Leipzig, Germany: 1852. Foerster A. Handbuch der speciellen pathologischen Anatomie. Leipzig, Germany: 1852. Vogl J. Pathologische Anatomie. Leipzig, Germany: 1854. Rokitansky von C. Lehrbuch der pathologischen Anatomie. Vienna, Austria: 1856. Friedreich N, Krankheiten des Herzens. Virchows Handbuch der speciellen Pathologie und Therapie. Erlangen, Germany: 1861. Paget J. Lectures on Surgical Pathology. Philadelphia, Pa: 1865. Rindfleisch E. Lehrbuch der pathologischen Gewebelehre. Leipzig, Germany: 1867. Zielonko G. Pathologische Anatomie und experimentelle Studie über Hypertrophie des Herzens. Virchows Arch Pathol Anat. 1875; 62:29 –55. Orth J. Lehrbuch der speciellen pathologischen Anatomie. Berlin, Germany: 1887. Wideroe S. Histologische Studien über die Muskulatur des Herzens. Virchows Arch Pathol Anat. 1911;204:190 –196. Aschoff L. Pathologische Anatomie. Jena, Germany: 1921. Kaufmann E. Specielle pathologische Anatomie. Berlin/Leipzig, Germany: 1922. Karsner HT, Saphir O, Todd TW. The state of the cardiac muscle in hypertrophy and atrophy. Am J Pathol. 1925;1:351–371. Petersen RO, Baserga R. Nucleic acid and protein synthesis in cardiac muscle of growing and adult mice. Exp Cell Res. 1965;40:340 –352. Morkin E, Ashford TP. Myocardial DNA synthesis in experimental cardiac hypertrophy. Am J Physiol. 1968;215:1409 –1413. Grove D, Nair KG, Zak R. Biochemical correlates of cardiac hypertrophy, III: changes in DNA content: the relative contributions of polyploidy and mitotic activity. Circ Res. 1969;25:463– 471. Grove D, Zak R, Nair KG, Aschenbrenner V. Biochemical correlates of cardiac hypertrophy, IV: observations on the cellular organization of growth during myocardial hypertrophy in the rat. Circ Res. 1969;25: 473– 485. Rakusan K. Cardiac growth, maturation, and aging. In: Zak R, ed. Growth of the Heart in Health and Disease. New York, NY: Raven Press Publishers; 1984:131–164. Ashley LM. A determination of the diameters of myocardial fibers in man and other mammals. J Anat. 1945;77:325–347. Linzbach AJ. Muskelfaserkonstante und das Wachstumsgesetz der menschlichen Herzkammern. Virchows Arch. 1950;318:575– 618. Olivetti G, Melissari M, Capasso JM, Anversa P. Cardiomyopathy of the aging human heart. Circ Res. 1991;68:1560 –1568. Olivetti G, Giordano G, Corradi D, Melissari M, Lagrasta C, Gambert SR, Anversa P. Gender differences and aging: effects on the human heart. J Am Coll Cardiol. 1995;26:1068 –1079. Adler CP, Costabel U. Cell number in human heart in atrophy, hypertrophy, and under the influence of cytostatics. Recent Adv Stud Cardiac Struct Metab. 1975;6:343–355. Adler CP, Costabel U. Myocardial DNA and cell number under the influence of cytostatics, I. post-mortem investigations of human hearts. Virchows Arch Cell Pathol. 1980;32:109 –125. Sandritter W, Adler CP. Numerical hyperplasia in human heart hypertrophy. Experientia. 1971;27:1435–1437. Arai S, Machida A. Myocardial cell in left ventricular hypertrophy. Tohoku J Exp Med. 1972;108:361–367. Hort W. Quantitative histologische Untersuchungen an wachsenden Herzen. Virchows Arch. 1953;323:223–242. Austin A, Fagan DG, Mayhew TM. A stereological method for estimating the total number of ventricular myocyte nuclei in fetal and postnatal hearts. J Anat. 1995;187:641– 647. Rakusan K, Flanagan MF, Geve T, Southern J, Van Praagh R. Morphometry of human coronary capillaries during normal growth and the 55. 56. 57. 58. 59. 60. 61. 62. 63. 64. 65. 66. 67. 68. 69. 70. 71. 72. 73. 74. 75. 76. 77. 78. 79. 80. effects of age in left ventricular pressure overload hypertrophy. Circulation. 1992;86:38 – 46. McKee PA, Castelli WP, McNamara PM, Kannel WB. The natural history of congestive heart failure: the Framingham Study. N Engl J Med. 1971;285:1441–1446. O’Rourke RA, Chatterjee K, Wei JY. Cardiovascular heart disease in the elderly: coronary heart disease. J Am Coll Cardiol. 1987;10:A52–A56. Frohlich ED, Apstein C, Chobanian AV, Devereux RB, Dustan HP, Dzau V, Fouad-Tarazi F, Horan MJ, Marcus M, Massie B, Pfeffer MA, Re RN, Roccella EJ, Savage D, Shub C. The heart in hypertension. N Engl J Med. 1992;327:998 –1008. Wei JY. Age and the cardiovascular system. N Engl J Med. 1992;327: 1735–1739. Arai S, Machida A, Nakamura T. Myocardial structure and vascularization of hypertrophied hearts. Tohoku J Exp Med. 1968;95:35–54. Linzbach AJ. Mikrometrische und histologische Analyse hypertropher menschlicher Herzen. Virchow Arch Pathol Anat Physiol. 1947;314: 534 –594. Alberts B, Bray D, Lewis J, Raff M, Roberts K, Watson JD. Molecular Biology of the Cell. 3rd ed. New York, NY/London, UK: Garland Publishing Inc; 1994:1142–1143. Sasaki R, Morishita T, Yamagata S. Mitosis of heart muscle cells in normal rats. Tohoku J Exp Med. 1968;96:405– 411. Sasaki R, Watanabe Y, Morishita T, Yamagata S. Estimation of the cell number of heart muscles in normal rats. Tohoku J Exp Med. 1968;95: 177–184. Katzberg AA, Fanner BB, Harris RA. The predominance of binucleation in isolated rat heart myocytes. Am J Anat. 1977;149:489 –500. Korecky B, Rakusan K. Normal and hypertrophic growth of the rat heart: changes in cell dimensions and number. Am J Physiol. 1978;234: H123–H128. Anversa P, Ricci R, Olivetti G. Quantitative structural analysis of the myocardium during physiologic growth and induced cardiac hypertrophy: a review. J Am Coll Cardiol. 1986;7:1140 –1149. Clubb FJ Jr, Bishop SP. Formation of binucleated myocardial cells in the neonatal rat: an index for growth hypertrophy. Lab Invest. 1984;50: 571–577. Reiss K, Cheng W, Ferber A, Kajstura J, Li P, Li B, Olivetti G, Homcy CJ, Baserga R, Anversa P. Overexpression of insulin-like growth factor-1 in the heart is coupled with myocyte proliferation in transgenic mice. Proc Natl Acad Sci U S A. 1996;93:8630 – 8635. Soonpaa MH, Kim KK, Pajak L, Franklin M, Field LJ. Cardiomyocyte DNA synthesis and binucleation during murine development. Am J Physiol. 1996;271:H2183–H2189. Page E, Earley J, Power B. Normal growth of ultrastructures in rat left ventricular myocardial cells. Circ Res. 1974;35(suppl II):II-12–II-16. Anversa P, Vitali-Mazza L, Loud AV. Morphometric and autoradiographic study of developing ventricular and atrial myocardium in fetal rats. Lab Invest. 1975;33:696 –705. Anversa P, Olivetti G, Bracchi PG, Loud AV. Postnatal development of the M-band in rat cardiac myofibrils. Circ Res. 1981;48:561–568. Cheng W, Reiss K, Kajstura J, Kowal K, Quaini F, Anversa P. Downregulation of the IGF1 system parallels the attenuation in the proliferative capacity of rat ventricular myocytes during postnatal development. Lab Invest. 1995;72:646 – 655. Marino TA, Haldar S, Williamson EC, Beaverson K, Walter RA, Marino DR, Beatty C, Lipson KE. Proliferating cell nuclear antigen in developing and adult rat cardiac muscle cells. Circ Res. 1991;69: 1353–1360. Dowell RT, McManus RE III. Pressure-induced cardiac enlargement in neonatal and adult rats: left ventricular functional characteristics and evidence of cardiac muscle cell proliferation in the neonate. Circ Res. 1978;42:303–310. MacDonald RA, Mallory GK. Autoradiography using tritiated thymidine. Lab Invest. 1959;8:1547–1562. Walker BE, Adrian EK. DNA synthesis in the myocardium of growing mature, senescent and dystrophic mice. Cardiologia. 1966;49:319 –328. Kranz D, Fuhrmann I, Keim U. Ein Beitrag zum physiologischen Herzwachstum. Z Mikrosk Anat Forsch. 1975;89:207–218. Overy HR, Priest RE. Mitotic cell division in postnatal cardiac growth. Lab Invest. 1966;15:1100 –1103. Anversa P, Hiler B, Ricci R, Guideri G, Olivetti G. Myocyte cell loss and myocyte hypertrophy in the aging rat heart. J Am Coll Cardiol. 1986;8:1441–1448. Anversa and Kajstura Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 81. Kajstura J, Zhang X, Liu Y, Szoke E, Cheng W, Olivetti G, Hintze TH, Anversa P. The cellular basis of pacing-induced dilated cardiomyopathy: myocyte cell loss and myocyte cellular reactive hypertrophy. Circulation. 1995;92:2306 –2317. 82. Wegner C, Mö1bert E. Das Verhalten des Myokards bei der experimentellen supravalvularen Aortenstenose: autoradiographische und elektronenmikroskopische Untersuchungen an Ratten-herzen. Virchows Arch A Pathol Anat. 1966;341:54 – 63. 83. Rumyantsev PP, Kassem AM. Cumulative indices of DNA synthesizing myocytes in different compartments of the working myocardium and conductive system of the rat’s heart muscle following extensive left ventricle infarction. Virchows Arch B Cell Pathol. 1976;20:329 –342. 84. van Krimpen C, Smits JFM, Cleutjens JPM, Debets JJM, Schoemaker RG, Struyker Boudier HAJ, Bosman FT, Daemen MJAP. DNA synthesis in the non-infarcted cardiac interstitium after left coronary artery ligation in the rat: effects of captopril. J Mol Cell Cardiol. 1991;23: 1245–1253. 85. Tachibana H, Inoue S, Oki H, Andou H, Katagiri T. Sequences in DNA synthetic phase ratio of spontaneous hypertensive rat (SHR) myocardium: study on development of cardiomegaly. Jpn Circ J. 1993;57: 442– 448. 86. Kajstura J, Zhang X, Reiss K, Szoke E, Li P, Lagrasta C, Cheng W, Darzynkiewicz Z, Olivetti G, Anversa P. Myocyte cellular hyperplasia and myocyte cellular hypertrophy contribute to chronic ventricular remodeling in coronary artery narrowing–induced cardiomyopathy in rats. Circ Res. 1994;74:383– 400. 87. Li F, Wang X, Capasso JM, Gerdes AM. Rapid transition of cardiac myocytes from hyperplasia to hypertrophy during postnatal development. J Mol Cell Cardiol. 1996;28:1737–1746. 88. Anversa P, Olivetti G, Loud AV. Morphometric study of early postnatal development in the left and right ventricular myocardium of the rat, I: hypertrophy, hyperplasia, and binucleation of myocytes. Circ Res. 1980; 46:495–502. 89. Olivetti G, Quaini F, Lagrasta C, Ricci R, Tiberti G, Capasso JM, Anversa P. Myocyte cellular hypertrophy and hyperplasia contribute to ventricular wall remodeling in anemia-induced cardiac hypertrophy in rats. Am J Pathol. 1992;141:227–239. 90. Gerdes AM, Moore JA, Hines JM. Regional changes in myocyte size and number in propranolol-treated hyperthyroid rats. Lab Invest. 1987; 57:708 –713. 91. Rakusan K, Raman S, Layberry R, Korecky B. The influence of aging and growth on the postnatal development of cardiac muscle in rats. Circ Res. 1978;42:212–218. 92. Bai S, Campbell SE, Moore JA, Morales MC, Gerdes AM. Influence of age, growth, and sex on cardiac myocyte size and number in rats. Anat Rec. 1990;226:207–212. 93. Brodsky WY, Tsirekidze NN, Arefyeva AM. Mitotic-cyclic and cycleindependent growth of cardiomyocytes. J Mol Cell Cardiol. 1985;17: 445– 455. 94. Loud AV, Anversa P. Morphometric analysis of biologic processes. Lab Invest. 1984;50:250 –261. 95. Anversa P, Olivetti G. Cellular basis of physiologic and pathologic myocardial growth. In: Page E, Fozzard HA, Solaro RJ, eds. Handbook of Physiology, Section 2: The Cardiovascular System, Volume 1, The Heart. New York, NY: Oxford University Press. In press. 96. Weisfeldt ML, Wright JR, Shreiner DP, Lakatta E, Shock NW. Coronary flow and oxygen extraction in the perfused heart of senescent male rats. J Appl Physiol. 1971;30:44 – 49. 97. Isoyama S, Wei JY, Izumo S, Fort P, Schoen FJ, Grossman W. Effect of age on the development of cardiac hypertrophy produced by aortic constriction in the rat. Circ Res. 1987;61:337–345. 98. Isoyama S, Grossman W, Wei JY. Effect of age on myocardial adaptation to volume overload in the rat. J Clin Invest. 1988;81:1850 –1857. 99. Lakatta EG. Cardiovascular regulatory mechanisms in advanced age. Physiol Rev. 1993;73:413– 467. 100. Wissler RW, Robert L. Aging and cardiovascular disease: a summary of the Eighth Münster International Arteriosclerosis Symposium. Circulation. 1996;93:1608 –1612. 101. Hachamovitch R, Wicker P, Capasso JM, Anversa P. Alterations in coronary blood flow and reserve with aging in Fischer 344 rats. Am J Physiol. 1989;256:H66 –H73. 102. Tomanek RJ, Aydelotte MR, Torry RJ. Remodeling of coronary vessels during aging in purebred beagles. Circ Res. 1991;69:1068 –1074. July 13, 1998 13 103. Anversa P, Li P, Sonnenblick EH, Olivetti G. Effects of aging on quantitative structural properties of coronary vasculature and microvasculature in rats. Am J Physiol. 1994;267:H1062–H1073. 104. Takahashi T, Schunkert H, Isoyama S, Wei JY, Nadal-Ginard B, Grossman W, Izumo S. Age related differences in the expression of proto-oncogene and contractile protein genes in response to pressure overload in the rat myocardium. J Clin Invest. 1992;89:939 –946. 105. Cheng W, Reiss K, Li P, Chun MJ, Kajstura J, Olivetti G, Anversa P. Aging does not affect the activation of the myocyte insulin-like growth factor-1 autocrine system after infarction and ventricular failure in Fischer 344 rats. Circ Res. 1996;78:536 –546. 106. Messerli FH, Ryan M. Pathophysiological and pathogenetic aspects of essential hypertension. In: Punri HA, Flamenbaum W, eds. Clinical Cardiovascular Therapeutics, Volume 1: Hypertension. Mount Kisco, NY: Futura; 1989:1–22. 107. Olivetti G, Quaini F, Sala R, Lagrasta C, Corradi D, Bonacina E, Gambert SR, Cigola E, Anversa P. Acute myocardial infarction in humans is associated with activation of programmed myocyte cell death in the surviving portion of the heart. J Mol Cell Cardiol. 1996;28: 2005–2016. 108. Narula J, Haider N, Virmani R, Di Salvo TG, Kolodgie FD, Hajjar RJ, Schmidt U, Semigran MJ, Dec GW, Khaw B-A. Apoptosis in myocytes in end-stage heart failure. N Engl J Med. 1996;335:1182–1189. 109. Mallat Z, Tedgui A, Fontaliran F, Frank R, Durigon M, Fontaine G. Evidence of apoptosis in arrhythmogenic right ventricular dysplasia. N Engl J Med. 1996;335:1190 –1196. 110. Olivetti G, Abbi R, Quaini F, Kajstura J, Cheng W, Nitahara JA, Quaini E, Di Loreto C, Beltrami CA, Krajewski S, Reed JC, Anversa P. Apoptosis in the failing human heart. N Engl J Med. 1997;336: 1131–1141. 111. Itoh G, Tamura J, Suzuki M, Suzuki Y, Ikeda H, Koike M, Nomura M, Jie T, Ito K. DNA fragmentation of human infarcted myocardial cells demonstrated by the nick end labeling method and DNA agarose gel electrophoresis. Am J Pathol. 1995;146:1325–1331. 112. Bardales RH, Hailey LS, Xie SS, Schaefer RF, Hsu SM. In situ apoptosis assay for the detection of early acute myocardial infarction. Am J Pathol. 1996;149:821– 829. 113. Linzbach AJ, Akuamoa-Boateng E. Die Alternsveränderungen des menschlichen Herzens II. Die Polypathie des Herzens im Alter. Klin Wochenschr. 1973;51:164 –175. 114. Linzbach AJ, Akuamoa-Boateng E. Die Alternsveränderungen des menschlichen Herzens I. Die Herzgewicht im Alter. Klin Wochenschr. 1973; 51:156 –163. 115. Tadokoro M, Arai S. Myocardial cell in right ventricular hypertrophy. Tohoku J Exp Med. 1972;106:5–16. 116. Linzbach AJ. Heart failure from the point of view of quantitative anatomy. Am J Cardiol. 1960;5:370 –382. 117. Kajstura J, Cheng W, Sarangarajan R, Li P, Li B, Nitahara JA, Chapnick S, Reiss K, Olivetti G, Anversa P. Necrotic and apoptotic myocyte cell death in the aging heart of Fischer 344 rats. Am J Physiol. 1996;271: H1215–H1228. 118. Anversa P, Palackal T, Sonnenblick EH, Olivetti G, Meggs LG, Capasso JM. Myocyte cell loss and myocyte cellular hyperplasia in the hypertrophied aging rat heart. Circ Res. 1990;67:871– 885. 119. Dimri GP, Lee X, Basile G, Acosta M, Scott G, Roskelley C, Medrano EE, Linskens M, Rubelj I, Pereira-Smith O, Peacocke M, Campisi J. A biomarker that identifies senescent human cells in culture and in aging skin in vivo. Proc Natl Acad Sci U S A. 1995;92:9363–9367. 120. Cohn JN, Bristow MR, Chien KR, Colucci WS, Frazier OH, Leinwand LA, Lorell BH, Moss AJ, Sonnenblick EH, Walsh RA, Mockrin SC, Reinlib L. Report of the National Heart, Lung, and Blood Institute special emphasis panel on heart failure research. Circulation. 1997;95: 766 –770. 121. Anversa P, Fitzpatrick D, Argani S, Capasso JM. Myocyte mitotic division in the aging mammalian rat heart. Circ Res. 1991;69: 1159 –1164. 122. Capasso JM, Bruno S, Cheng W, Li P, Rodgers R, Darzynkiewicz Z, Anversa P. Ventricular loading is coupled with DNA synthesis in adult cardiac myocytes after acute and chronic myocardial infarction in rats. Circ Res. 1992;71:1379 –1389. 123. Astorri E, Chizzola A, Visioli O, Anversa P, Olivetti G, Vitali-Mazza L. Right ventricular hypertrophy: a cytometric study on 55 human hearts. J Mol Cell Cardiol. 1971;2:99 –110. 124. Adler C-P, Costabel U. Cell number in human heart in atrophy, hypertrophy, and under the influence of cytostatics. In: Fleckenstein A, Rona 14 125. 126. 127. 128. 129. 130. Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 131. 132. 133. 134. 135. 136. 137. 138. 139. 140. Myocyte Proliferation G, eds. Recent Advances in Studies on Cardiac Structure and Metabolism, Volume 6: Pathophysiology and Morphology of Myocardial Cell Alteration. Baltimore, Md: University Park Press; 1975:343–355. Astorri E, Bolognesi R, Colla B, Chizzola A, Visioli O. Left ventricular hypertrophy: a cytometric study on 42 human hearts. J Mol Cell Cardiol. 1977;9:763–775. Adler CP, Friedburg H. Myocardial DNA content, ploidy level and cell number in geriatric hearts: post-mortem examinations of human myocardium in old age. J Mol Cell Cardiol. 1986;18:39 –53. Vliegen HW, van der Laarse A, Cornelisse CJ, Eulderink F. Myocardial changes in pressure overload-induced left ventricular hypertrophy: a study on tissue composition, polyploidization and multinucleation. Eur Heart J. 1991;12:488 – 494. Grajek S, Lesiak M, Pyda M, Zajac M, Paradowski S, Kaczmarek E. Hypertrophy or hyperplasia in cardiac muscle: postmortem human morphometric study. Eur Heart J. 1993;14:40 – 47. Olivetti G, Melissari M, Balbi T, Quaini F, Sonnenblick EH, Anversa P. Myocyte nuclear and possible cellular hyperplasia contribute to ventricular remodeling in the hypertrophic senescent heart in humans. J Am Coll Cardiol. 1994;24:140 –149. Olivetti G, Cigola E, Maestri R, Corradi D, Lagrasta C, Gambert SR, Anversa P. Aging, cardiac hypertrophy and ischemic cardiomyopathy do not affect the proportion of mononucleated and multinucleated myocytes in the human heart. J Mol Cell Cardiol. 1996;28:1463–1477. Gerschenson LE, Rotello RJ. Apoptosis: a different type of cell death. FASEB J. 1992;6:2450 –2455. Olivetti G, Melissari M, Balbi T, Quaini F, Cigola E, Sonnenblick EH, Anversa P. Myocyte cellular hypertrophy is responsible for ventricular remodeling in the hypertrophied heart of middle aged individuals in the absence of cardiac failure. Cardiovasc Res. 1994;28:1199 –1208. Quaini F, Cigola E, Lagrasta C, Saccani G, Quaini E, Rossi C, Olivetti G, Anversa P. End-stage cardiac failure in humans is coupled with the induction of proliferating cell nuclear antigen and nuclear mitotic division in ventricular myocytes. Circ Res. 1994;75:1050 –1063. Anversa P, Loud AV, Giacomelli F, Wiener J. Absolute morphometric study of myocardial hypertrophy in experimental hypertension, II: ultrastructure of myocytes and interstitium. Lab Invest. 1978;38:597– 609. Bishop SP, Oparil S, Reynolds RH, Drummond JL. Regional myocyte size in normotensive and spontaneously hypertensive rats. Hypertension. 1979;1:378 –383. Marino TS, Kent RL, Uboh CE, Fernandez E, Thompson EW, Cooper G. Structural analysis of pressure versus volume overload hypertrophy of cat right ventricle. Am J Physiol. 1985;249:H371–H379. Reiss K, Kajstura J, Capasso JM, Marino TA, Anversa P. Impairment of myocyte contractility following coronary artery narrowing is associated with activation of the myocyte IGF-1 autocrine system, enhanced expression of late growth related genes, DNA-synthesis and myocyte nuclear mitotic division in rats. Exp Cell Res. 1993;207:348 –360. Reiss K, Kajstura J, Zhang X, Li P, Szoke E, Olivetti G, Anversa P. Acute myocardial infarction leads to upregulation of the IGF-1 autocrine system, DNA replication, and nuclear mitotic division in the remaining viable cardiac myocytes. Exp Cell Res. 1994;213:463– 472. Liu Y, Cigola E, Cheng W, Kajstura J, Olivetti G, Hintze TH, Anversa P. Myocyte nuclear mitotic division and programmed myocyte cell death characterize the cardiac myopathy induced by rapid ventricular pacing in dogs. Lab Invest. 1995;73:771–787. Soonpaa MH, Field LJ. Assessment of cardiomyocyte DNA synthesis during hypertrophy in adult mice. Am J Physiol. 1994;266: H1439 –H1445. 141. Soonpaa MH, Koh GY, Pajak L, Jing S, Wang H, Franklin MT, Kim KK, Field LJ. Cyclin D1 overexpression promotes cardiomyocyte DNA synthesis and multinucleation in transgenic mice. J Clin Invest. 1997; 99:2644 –2654. 142. Olivetti G, Ricci R, Anversa P. Hyperplasia of myocyte nuclei in long-term cardiac hypertrophy in rats. J Clin Invest. 1987;80: 1818 –1821. 143. Anversa P, Palackal T, Sonnenblick EH, Olivetti G, Capasso JM. Hypertensive cardiomyopathy: myocyte nuclei hyperplasia in the mammalian rat heart. J Clin Invest. 1990;85:994 –997. 144. Reiss K, Meggs LG, Li P, Olivetti G, Capasso JM, Anversa P. Upregulation of IGF1, IGF1-receptor and late growth related genes in ventricular myocytes acutely after infarction in rats. J Cell Physiol. 1994;158: 160 –168. 145. Reiss K, Cheng W, Giordano A, De Luca A, Li B, Kajstura J, Anversa P. Myocardial infarction is coupled with the activation of cyclins and cyclin-dependent kinases in myocytes. Exp Cell Res. 1996;225:44 –54. 146. Yoshizumi M, Lee W-S, Hsieh C-M, Tsai J-C, Li J, Perrella MA, Patterson C, Endege WO, Schlegel R, Lee M-E. Disappearance of cyclin A correlates with permanent withdrawal of cardiomyocytes from the cell cycle in human and rat hearts. J Clin Invest. 1995;95:2275–2280. 147. Engelmann GL, Boehm KD, Haskell JF. Insulin-like growth factors and neonatal cardiomyocyte development: ventricular gene expression and membrane receptor variations in normotensive and hypertensive rats. Mol Cell Endocrinol. 1989;63:1–14. 148. Decker RS, Cook MG, Behnke-Barclay M, Decker ML. Some growth factors stimulate cultured adult rabbit ventricular myocyte hypertrophy in the absence of mechanical loading. Circ Res. 1995;77:544 –555. 149. Reiss K, Cheng W, Pierzchalski P, Kodali S, Li B, Wang S, Anversa P. Insulin-like growth factor-1 receptor and its ligand regulate the reentry of adult ventricular myocytes into the cell cycle. Exp Cell Res. 1997; 235:198 –209. 150. Donath MY, Azpf J, Eppenberger-Eberhardt M, Froesch EF, Eppenberger HM. Insulin-like growth factor I stimulates myofibril development and decreases smooth muscle a -actin of adult cardiomyocytes. Proc Natl Acad Sci U S A. 1994;19:1686–1690. 151. Toyozaki T, Hiroe M, Hasumi M, Horie T, Hosoda S, Tsushima T, Sekiguchi M. Insulinlike growth factor 1 receptors in human cardiac myocytes and their relation to myocardial hypertrophy. Jpn Circ J. 1993;57:1120 –1127. 152. Donohue TJ, Dworkin LD, Lango MN, Fliegner K, Lango RP, Benstein JA, Slater WR, Catanese VM. Induction of myocardial insulin-like growth factor-1 gene expression in left ventricular hypertrophy. Circulation. 1994;89:799 – 809. 153. Duerr RL, Huang S, Miraliakbar HR, Clark R, Chien KR, Ross J Jr. Insulin-like growth factor-1 enhances ventricular hypertrophy and function during the onset of experimental cardiac failure. J Clin Invest. 1995;95:619 – 627. 154. Li Q, Li B, Wang X, Leri A, Jana KP, Liu Y, Kajstura J, Baserga R, Anversa P. Overexpression of insulin-like growth factor-1 in mice protects from myocyte death after infarction, attenuating ventricular dilation, wall stress, and cardiac hypertrophy. J Clin Invest. 1997;100:1991–1999. KEY WORDS: cell proliferation n cell cycle n cell death n insulin-like growth factor-1 Ventricular Myocytes Are Not Terminally Differentiated in the Adult Mammalian Heart Piero Anversa and Jan Kajstura Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 Circ Res. 1998;83:1-14 doi: 10.1161/01.RES.83.1.1 Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1998 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7330. Online ISSN: 1524-4571 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circres.ahajournals.org/content/83/1/1 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation Research is online at: http://circres.ahajournals.org//subscriptions/