Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
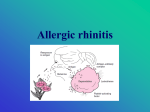
Allergic Rhinitis Megan D. Pendley, RPh, PharmD PPS 946 Spring 2015 Lecture Objectives • • • • • Describe the etiology, risk factors, and pathophysiology of allergic rhinitis Identify common presenting signs and symptoms of allergic rhinitis and distinguish between other types of rhinitis Discuss the pharmacology, side effects, drug interactions, and proper dosing of commonly used medications for allergic rhinitis Given a patient case, select an appropriate treatment regimen, monitoring parameters and patient related consultation recommendations considering the patient's diagnosis and unique characteristics Assess a patient’s pharmacotherapeutic regimen for safety and efficacy using clinical signs, symptoms and laboratory data Counsel patients on the appropriate use of nasal preparations Allergic Rhinitis • • IgE mediated response Characterized by – Sneezing – Nasal itching – Watery rhinorrhea – Nasal congestion – Itching of throat, eyes, & ears Seasonal Symptoms occur at predictable times of the year (spring/fall) Perennial Symptoms are year-round, chronic and subtle Allergens: pollen from trees, grasses and weeds Allergens: NON seasonal antigens (dustmites, animal dander, and molds Why do we care? • • • • VERY COMMON problem 6th most prevalent chronic illness in the US 20-30% of adults affected >40% of children affected • Many complications: – Limited ability to perform ADLs – Mental fatigue/ Insomnia/ Malaise – Poor work/school performance – Loss of smell or taste – Chronic cough, hoarseness, vocal polyps – Anxiety – Depressive disorders – Asthma (more prevalent in perennial AR) – Sinusitis – OM – Nasal polyposis – URIs – Orthodontic problems Predisposing Factors • Genetics • Allergen exposure • Microbial exposure in early life • Eczema • Second hand smoke exposure • Increased levels of IgE before 6 years of age Nasal Physiology Three primary functions in preparing the air for the lungs: Heating Humidifying Cleaning Immediate Reaction • • • • Occurs within minutes Mediators of hypersensitivity: – Histamine – Leukotrienes – Prostaglandins – Tryptase – Kinins Symptoms include: Rhinorrhea Late Phase Reaction • • • • • Occurs in 50% of patients 4 – 8 hours after initial exposure with symptoms peaking within 12-24 hours Due to mast cell cytokine release Persistent, chronic symptoms Primarily nasal congestion • • • • • • Itching Sneezing Nasal obstruction Vasodilation ↑ vascular permeability Production of nasal secretions Allergic Rhinitis Clinical Presentation Symptoms: Clear rhinorrhea Sneezing Nasal congestion Post-nasal drip Pruritic eyes, ears, nose, or palate Physical Exam: Allergic shiners Transverse nasal crease Adenoidal breathing Pale, bluish edematous nasal turbinates coated with thin, clear secretions Tearing and conjunctival injection and edema Periorbital swelling Pharyngeal “cobblestone” appearance Diagnostic Tests: • Nasal cytology – Nasal secretions stained – Eosinophils→allergic – Neutrophils→infection • Skin tests – Scratch test (percutaneous) • Make superficial wound on outermost layer of the skin • A drop of antigen is then placed in the wound – Intradermal • Diluted allergen injected between layers of the skin Common Cold Sore throat and cough predominate +/- Fever Sore or scratchy throat on 1st day and is short lived Nasal symptoms by 2nd or 3rd day and d/c may be purulent Cough predominates by 4th or 5th day Allergic Rhinitis Congestion, rhinorrhea and itching predominate Fever not present Nasal d/c thin and clear Classic PE findings present Pharyngeal cobblestoning Pale, boggy nasal turbinates Conjunctival irritation Allergic shiners Absence of characteristic PE findings found in allergic rhinitis Treatment Goals: – Minimize and prevent symptoms – Maintain a normal lifestyle Three approaches - Allergen avoidance - Pharmacotherapy - Immunotherapy Allergen Avoidance Pollens Keep windows and doors closed during pollen season Avoid fans that draw in outside air Use air conditioning If possible, eliminate outside activities during times of high pollen counts Shower, shampoo, and change clothes following outdoor activity Use a vented dryer rather than an outside clothes line Molds Use similar controls as above Avoid walking through uncut fields, working with compost or dry soil, and raking leaves Clean indoor moldy surfaces Fix all water leaks in home Reduce indoor humidity to <50% if possible House dust mites Encase mattresses, pillows, and box springs in an allergen-impermeable cover Wash bedding in hot water weekly Remove stuffed toys from bedroom Minimize carpet use and upholstered furniture Reduce indoor humidity to <50% if possible Animal allergens (if removal of pets not acceptable) Keep pet out of patient’s bedroom Isolate pet from carpet and upholstered furniture Wash pet weekly Cockroaches Keep food and garbage in tightly closed containers Take out garbage regularly Clean up dirty dishes promptly Use roach traps Other recommendations Do not allow smoking around the patient, in the patient’s home, or in the family car Minimize the use of wood burning stoves and fireplaces Pharmacotherapy Nasal Steroids (See Nasal Steroid Chart provided on Bb) Best choice for perennial rhinitis and good for seasonal when used in advance of symptomatic season The most effective single maintenance therapy for allergic rhinitis and causes few side effects Particularly useful for predominant nasal congestion Produces significantly greater relief of nasal blockage, nasal discharge, sneezing, nasal itch, post-nasal drip, and total nasal symptoms than oral antihistamines Considered 1st line therapy in those with “significant enough” symptoms to seek medical treatment MOA: Binds to glucocorticoid receptors in inflammatory cells ↓ inflammation by decreasing mediator release ↓ neutrophil infiltration ↓intracellular edema, causing mild vasoconstriction Inhibits mast cell mediated late-phase reactions All agents are equally efficacious. Peak response 2-3 weeks HPA Axis issues in children---o Limited to no effect on HPA axis and growth in children o Agents dosed once daily preferred o Agents approved for children ≥ 2 years of age: Fluticasone furoate (Veramyst®) Mometasone (Nasonex®) Triamcinolone (Nasacort AQ) o Additive effects of intranasal steroids with other glucocorticoid preparations Effects on IOP and BMD---- Insignificant data to estimate risk for effects on bone mineral density and intraocular pressure, but may be reasonable to inform patients if they have concerns Side effects: o Sneezing, stinging, HA, epistaxis, drying of nasal mucosa, concern with local infection with Candida (rare) Administration o Start with max dose for age and taper down to lowest effective dose that controls symptoms (usually done at weekly intervals once symptoms are controlled) o Benefits may not be seen for a few days with peak responses observed in 2-3 weeks o May use decongestant 1st to open up nasal passages, then use nasal steroid o Avoid sneezing or blowing nose for at least 10 minutes after administering How to administer the nasal spray o Shake well o Prime (if first time use or more than a week since last use) o Patient can use nasal saline to clean the nose if mucous crusting is present o Hold one nostril closed o Tuck chin slightly with head slightly downward o In opposite nose, place spray tip just inside nose, direct away from septum, and while breathing in actuate spray and sniff slightly o Breathe out through mouth o If using 2 sprays, repeat the above then switch to the other nostril and repeat above Antihistamines: General Information H-1 receptor antagonists- bind to H1 receptors preventing histamine binding and action Available in oral, ophthalmic and intranasal dosage forms Oral antihistamines are most commonly used Agents are more effective in PREVENTING the actions of histamine than in reversing these actions once they have taken place (better at preventing symptoms than reversing them once they start) o Most effective when taken about 1-2 hours before anticipated exposure to allergen Reversal of symptoms primarily due to anticholinergic effects: o Drying effect o Antagonize the increase in capillary hyperpermeability, wheal and flare formation, and itching o Effective at reducing itching, sneezing, and rhinorrhea, with LESS impact on nasal congestion o Considered less effective than intranasal corticosteroids (INCS) at symptom control o In general, these agents are used in combination with INCS for symptom control or alone when symptoms are predictable and intermittent Antihistamines First Generation Adult Child Diphenhydramine 25-50 mg q6-8h 5 mg/kg/day q6-8h Second Generation Adult Child Cetirizine 5-10 mg qd 6-12 mos: 2.5mg qd 12-23 mos: 2.5 mg qd-bid 2-5 yr: 2.5-5 mg qd **Fexofenadine (sometimes called 3rd generation) 60mg bid OR 180mg qd 6 mos - <2 yr: 15mg bid 2-11 yrs: 30 mg bid **Desloratadine (sometimes called 3rd generation) Loratadine 5mg qd 6-11 mos: 1mg qd 1-5 yrs: 1.25 mg qd 6-11 yrs: 2.5 mg qd 10mg qd 2-5 yrs: 5mg qd (up to 25 mg/dose) Chlorpheniramine IR: 4mg q4-6h SR: 8-12mg q812h IR: 2-6 yo: 1mg q4-6h (do not exceed 6 mg in 24 hr) IR: 6-12 yo: 2mg q4-6h (do not exceed 12 mg/day) SR: 6-12 yo: 8 mg HS Hydroxyzine (Rx) 25mg 3-4x/day 2mg/kg/day div q6-8 hrs Brompheniramine See Box Label (dose varies with brand) ER: 6-16mg q12h IR: 4-8mg 3-4 x/day See Box Label (dose varies with brand) Carbinoxamine (Karbinal ER®, Palgic ®, Arbinoxa®) (Rx) ER: 2-<4yo: 3-4mg q12h 4-<6yo: 3-8mg q12h 6-<12: 6-12mg q12h IR: 2-<6yo 1-2mg 3-4 x/day 6-<12yo: 2-4mg 3-4 x/day First Generation Information: Non-selective High incidence of CNS effects, primarily sedation and has been implicated in several MVAs, including several fatal accidents, impaired work and school performance Use prohibited in many states for transportation workers Can cause paradoxical agitation in young children Significant anticholinergic side effects, therefore use with caution in: o ↑ IOP o Hyperthyroidism o Cardiovascular disease Place in therapy: o Considered 2nd line compared with the 2nd generation antihistamines o OK for mild-moderate intermittent symptoms o Symptoms primarily at night interfering with sleep o Patients who have significant cost issues o Patients who can stand a little sedation (i.e. not transportation workers, etc) o Not ideal in the elderly and in children COMBO PRODUCT!! Hydrocodone/Chlorpheneramine (TussiCaps®, Tussionex Pennkinetic ER®, Vituz ®)----available as 5-4mg and 10-8mg ER Capsule, 10-8mg/5mL controlled release liquid; 54mg/5mL Solution. Second Generation Information Peripherally selective Non-sedating (at least less sedating than the 1st generation) Little or no CNS effects Very few anticholinergic effects Tend to be longer acting and are thus dosed once or twice daily Oral preparations are all equally efficacious Oral preparations – all are similarly efficacious o Loratidine, cetirizine o Fexofenadine, desloratidine, levocetirizine – “3rd generation” Topical preparations: o Olopatadine, azelastine Place in therapy: o Considered 1st line among the antihistamines o OK for mild-moderate intermittent –persistent symptoms o Best choice for most patients including children and elderly and those who cannot tolerate sedation o Good for patients in whom cost not an issue (more of a concern for prescription products) Intranasal antihistamines Azelastine (Astelin®, Astepro®) COMBO Product: Azelastine/Fluticasone (Dymista®) o Nasal route is an alternative to switching to another oral route if oral agents have not been effective Pros: o Produces rapid effects o Good for nonallergic rhinitis as well as the allergic type o Good for predominately nasal symptoms (sneezing, postnasal drip, congestion, rhinorrhea) Cons: o Bitter taste in ~20% of patients o Significant drying effects, headache and decreased efficacy over time o Systemic absorption ~40% so can cause drowsiness Additional option for intranasal preparations: Olopatadine (Patanase®) – 2 sprays each nostril bid Ophthalmic antihistamines Used for predominately ocular symptoms (allergic conjunctivitis) Rx: Azelastine (Optivar®): 1 gtt to each affected eye bid Rx: Olopatadine (Patanol®): 1 gtt to each affected eye bid @ intervals of 6-8 hours OTC: Visine® Allergy (naphazoline/ pheniramine) Contains both an antihistamine and ocular decongestant 1-2 gtts in affected eye(s) 3-4 times daily Caution with glaucoma and other eye disorders May cause pupillary enlargement Decongestants Sympathomimetic agents that act on adrenergic receptors in the nasal mucosa, producing vasoconstriction Shrink swollen mucosa Improve ventilation Good in combination with antihistamines Decongestants Topical Systemic Applied directly to swollen nasal mucosa via drops or sprays Results in little to no systemic absorption Available OTC (↓$) Rapid onset of relief Side effects: o Burning, stinging o Sneezing, nasal dryness o Rhinitis medicamentosa (rebound vasodilation) – associated with use beyond 3-5 days Place in therapy: o NOT for routine use o Good for prn occasional congestion relief Counseling points o No more than3-5 days of use (less is better) o Use as small a dose as possible as infrequently as possible and only when absolutely necessary Short Acting Phenylephrine HCl (Neosynephrine®) 1-2 sprays/ drops each nostril q4h prn Lasts up to 4 hours Not as effective on an immediate basis as the topical agents but the effects sometimes last longer and cause less local irritation Rhinitis medicamentosa NOT a problem Side effects: o Mild CNS stimulation o Insomnia, irritability, HA o Stroke a concern in those with HTN &/or vasospasm o Elevates BP o Heart palpitations o Tremor, nervousness o Contraindicated in those taking MAOIs Caution in those with: o Closed angle glaucoma o Cardiovascular or cerebrovascular disease o Hyperthyroidism o Bladder neck obstruction Place in therapy: o Alone for occasional nasal congestion o In combination with antihistamines for relief of rhinitis symptoms where congestion is a predominant problem Intermediate Acting Naphazoline (Privine®) Tetrahydrozoline (Tyzine®)Rx Long Acting Oxymetazoline (Afrin®) 1-2 sprays/ drops each nostril q6h prn Pseudoephedrine 2-5 yrs: 15mg q4-6h 6-12 yrs: 30mg q4-6h Adults: IR: 30-60mg q4-6h SR: 120mg q12h OR 240mg q24h Phenylephrine 2-6 yrs: 1.8-3.75 mg q12h 6-12yrs: 10 mg q4h Adults: 10-20 mg q4h Both last up to 4-6 hours 2-4 drops or 3-4 sprays q3-4h prn 2-3 sprays each nostril bid Lasts up to 12 hours Cromolyn sodium (Nasalcrom®) MOA: mast cell stabilizer o Inhibits allergen triggered mast cell degranulation and release of mediators (including histamine) o Has no DIRECT antihistaminic, anticholinergic or anti-inflammatory properties Available OTC Dose: Adults and children > 2yo: 1 spray each nostril 3-4x/day spaced about q4-6h Side effects: sneezing, irritation, nasal stinging Pearls: o For greatest efficacy, must cover entire nasal lining o Blow nose before administering o Dosing really should be spaced q6h to maintain effect Efficacy: o less effective than nasal steroids or second generation antihistamines o most effective for allergic rhinitis when initiated just prior to the allergy season, rather than after symptoms have begun Place in therapy: o Blocks symptoms associated with the immediate and late phase nasal allergen challenge and is effective in doing so even when used shortly before allergen inhalation. This makes cromolyn particularly useful for individuals who experience episodic symptoms to allergens, such as a cat, where it may be used 30 minutes prior to exposure o Used most commonly in pediatric patients with mild allergic rhinitis whose parents wish to avoid nasal steroids Montelukast (Singulair®) Nasal congestion in experimental allergic rhinitis correlates best with with leukotriene C4 (LTC4) levels, whereas sneezing and nasal itching correlate with histamine levels 1st leukotriene receptor antagonist approved for the treatment of seasonal allergic rhinitis Inhibits inflammatory mediator release from mast cells Dose: o Adults: 10 mg once daily in the evening o 12 – 23 months: 4 mg (oral granules) once daily, in the evening Place in therapy: o Less effective than nasal steroids o In combo with 2nd generation antihistamine: better than any agent alone o Usually reserved for patients who have epistaxis or intolerance to nasal steroids or azelastine o Also useful in people with concomitant asthma (kill two birds with one stone) and in patients who also have nasal polyposis Ipratropium bromide Anticholinergic nasal spray Exhibits drying properties, therefore most effective for symptoms of rhinorrhea Dose: 2 sprays each nostril 2-3 times per day Side effects: HA, epistaxis, nasal dryness Caution in glaucoma and BPH Place in therapy: o not recommended as a first-line drug in allergic rhinitis, but sometimes useful in children or adults who have profuse rhinorrhea not otherwise controlled with topical nasal steroids, a complaint most commonly observed in adult patients with concomitant allergic and nonallergic (or vasomotor) rhinitis. Adjunct Therapy Nasal Saline therapy o Useful with mild symptoms, or for use before using other topical medications o Commonly performed once or twice daily, or as needed Immunotherapy (“Allergy shots”) $$$$ and very time consuming Patients must commit to the time it requires to do this Slow gradual process of injecting increasing doses of antigen responsible for allergic symptoms in the hope of inducing tolerance Several proposed mechanisms: o Induces IgG antibodies o Decreases specific IgE o Decreases recruitment of effector cells o Altered T cell cytokine balance o T cell anergy o Induction of regulatory T cells Start with very dilute solutions 1-2 x/week then increase concentration until max tolerated dose is achieved and continue Immunotherapy usually done for 3-5 years Best in people with: o Strong h/o severe symptoms unsuccessfully controlled by avoidance and PTX o Patients with strong propensity for the development of asthma (allergy shots may postpone the onset or prevent it altogether) o Intolerable side effects to most pharmacotherapy Side effects: o Mild local skin reactions: induration and swelling @ injection site o Generalized urticaria, bronchospasm, laryngospasm, and vascular collapse (rare) o Death from anaphylaxis o Treat with epi, antihistamines, and systemic steroids if occurs Avoid immunotherapy in: o Those unable to tolerate anaphylactic type reaction (usually those with severe, brittle, systemic steroid dependant asthmatics) o Unstable cardiovascular disease o Those on significant doses of beta blockers o Immunocompromise o h/o nonadherence to PTX treatment Summary points: In most pediatric and adult patients, allergic rhinitis is a persistent condition that requires ongoing therapy over a period of years. The current approach to management combines allergen avoidance and pharmacologic therapy, with allergen immunotherapy added for refractory or severe cases. The patient’s specific triggers should be determined whenever possible, either by history or by specific allergy testing. Patients whose symptoms are severe or refractory to pharmacotherapy should be referred to an allergy specialist. Intranasal steroids are the most effective single therapy for allergic rhinitis in most patients with significant or persistent symptoms