Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
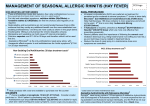
Cetirizine Removal from the List Peer Feedback: “Available OTC” Note: other allergy medications are included on the list (budesonide, diphenhydramine). Comment was vague, so review will focus on efficacy. Literature Review Question: What is the efficacy of cetirizine and other anti-allergy medications? Literature Search: eCPS - Respiratory Disorders: Allergic Rhinitis References taken from eCPS page Pubmed – ‘allergic rhinitis AND comparison AND efficacy AND antihistamine AND (Review OR Meta-Analysis’ The diagnosis and management of rhinitis (2008) Note: Letter at end of paragraph indicates strength of recommendation (see below for chart explanation) Pharmacologic therapy Oral antihistamines 61. Second-generation antihistamines are generally preferred over first-generation antihistamines for the treatment of allergic rhinitis. First-generation antihistamines have significant potential to cause sedation, performance impairment, and anticholinergic effects. Although occasionally advantageous (eg, sleep induction when taken at bedtime or a reduction in rhinorrhea), these properties are usually undesirable and are potentially dangerous. Second-generation antihistamines have less or no tendency to cause these effects. B 62. Before prescribing or recommending a first-generation antihistamine, the physician should ensure that the patient understands both the potential for adverse effects and the availability of alternative antihistamines with a lower likelihood of adverse effects. D 63. There are important differences among the second-generation antihistamines in regard to their sedative properties: fexofenadine, loratadine, and desloratadine do not cause sedation at recommended doses; loratadine and desloratadine may cause sedation at doses exceeding the recommended dose; cetirizine and intranasal azelastine may cause sedation at recommended doses. A 64. Among the newer, nonsedating antihistamines, no single agent has been conclusively found to achieve superior overall response rates. C Second-generation oral antihistamines [Summary Statements 61-64] Second-generation antihistamines are generally preferred over first-generation antihistamines for treatment of allergic rhinitis because they have less tendency to cause sedation, performance impairment, and/or anticholinergic adverse effects.307-311 First-generation antihistamines may produce performance impairment in school176,312,313 and driving314-318 that can exist without subjective awareness of sedation;310 and the use of first-generation antihistamines has been associated with increased automobile and occupational accidents.314-319 Individual variation exists with respect to development of sedative effects with first-generation antihistamines.307,309,313 Concomitant use of other central nervous system (CNS)–active substances, such as alcohol and sedatives, may further enhance performance impairment from these antihistamines.307,309 In part because of prolonged plasma half-life and metabolites (Table VII), these undesirable and potentially dangerous side effects cannot be eliminated by administration of first-generation antihistamines only at bedtime.320-325 Anticholinergic effects include dryness of mouth and eyes, constipation, inhibition of micturition, and an increased risk for provocation of narrow-angle glaucoma. Increased sensitivity and a greater incidence of preexisting comorbid conditions, such as prostatic hypertrophy, elevated IOP, and cognitive impairment, place older adults in a high-risk category for the side effects of first-generation antihistamines. The anticholinergic effects of the first-generation antihistamines may explain the reported better control of rhinorrhea compared with the second-generation antihistamines. The overall efficacy of first-generation antihistamines compared with second generation for the management of allergic rhinitis symptoms has not been adequately studied. Second-generation antihistamines differ in their onset of action, sedation properties, skin test suppression, and dosing guidelines (Table VIII). No single agent has been conclusively shown to have superior efficacy.326,327 Exceeding the recommended dosage may result in increased sedation with many of these products309,323,328-330 that do not produce sedation at recommended doses. Although antihistamines can be used on an intermittent basis, such as for episodic allergic rhinitis, it has been shown that continuous treatment for seasonal or perennial allergic rhinitis is more effective,331 primarily because of unavoidable, ongoing allergen exposure. Intranasal corticosteroids 74. Intranasal corticosteroids are the most effective medication class for controlling symptoms of allergic rhinitis. A 75. In most studies, intranasal corticosteroids have been shown to be more effective than the combined use of an antihistamine and leukotriene (LT) antagonist in the treatment of seasonal allergic rhinitis. A 76. Intranasal corticosteroids may provide significant relief of symptoms of seasonal allergic rhinitis when used not only on a regular basis but also on an as-needed basis. B However, asneeded use may not be as effective as continuous use of intranasal corticosteroids. D 77. When comparing the available intranasal corticosteroids, the overall clinical response does not appear to vary significantly between products irrespective of the differences in topical potency, lipid solubility, and binding affinity. C 78. Intranasal corticosteroids may be useful in the treatment of some forms of non-allergic rhinitis. A 79. Intranasal corticosteroids when given in recommended doses are not generally associated with clinically significant systemic side effects. A 80. Although local side effects are typically minimal with the use of intranasal corticosteroids, nasal irritation and bleeding may occur. Nasal septal perforation is rarely reported. B Intranasal corticosteroids [Summary Statements 74-80] Intranasal corticosteroids are the most effective medications for treating allergic rhinitis. In most studies, intranasal corticosteroids are more effective than the combined use of an antihistamine and a LT antagonist.375-379 The clinical response does not appear to vary significantly between intranasal corticosteroids that are currently available (Table VIII).53,380-382 The onset of therapeutic effect of intranasal corticosteroid occurs between 3 and 12 hours.383-385 The asneeded dosing (which equated to 55% to 62% of days) of an intranasal corticosteroid (fluticasone propionate) has been shown to be effective in the treatment of seasonal allergic rhinitis380,386,387 but may not be as efficacious as continuous use. In 1 study, PRN use of an intranasal corticosteroid (fluticasone propionate) was superior to PRN use of an oral antihistamine (loratadine) for seasonal allergic rhinitis.380 Intranasal corticosteroids are also effective in the treatment of nonallergic rhinitis, especially NARES388-390 and vasomotor rhinitis.389,391,392 Intranasal corticosteroids may also benefit ocular allergy symptoms associated with allergic rhinitis (see Summary Statement 19). Intranasal corticosteroids when given in recommended doses are not generally associated with clinically significant systemic side effects. Studies in both children and adults have failed to demonstrate any consistent, clinically relevant effect from intranasal corticosteroids on the hypothalamic-pituitary-adrenal (HPA) axis,393-401 ocular pressure or cataract formation,393,402-404 or bone density.405-407 In children, growth effect may be a better indicator of systemic effect than HPA axis suppression. The transient effect on growth suppression that has been demonstrated in children after administration of intranasal corticosteroids is dependent on the specific intranasal corticosteroid, and the dose administered, technique used for measuring growth, time of administration, and concomitant use of oral or inhaled corticosteroid. Studies with intranasal fluticasone propionate, mometasone furoate, and budesonide have shown no effect on growth at recommended doses compared with placebo408-410 and reference values (at as much as 2 times the recommended doses).400 Growth suppression from intranasal corticosteroids has been reported only with longterm use of beclomethasone dipropionate that exceeded recommended doses409 or administration to toddlers.411 Local side effects of intranasal corticosteroids such as nasal irritation, bleeding, and nasal septal perforation412,413 are rare and can be avoided with proper administration technique. The patient should be periodically examined to assure that these side effects are not present. Preparations containing propylene glycol and benzalkonium chloride may result in local irritation or ciliary dysfunction, respectively414,415 (Table VIII). Classification of recommendations and evidence Category of evidence Strength of Recommendation Ia. Evidence from meta-analysis of randomized controlled trials A Directly based on category I evidence Ib. Evidence from at least 1 randomized controlled trial B Directly based on category II evidence or extrapolated recommendation from category I evidence IIa. Evidence from at least 1 controlled study without randomization C Directly based on category III evidence or extrapolated recommendation from category I or II evidence IIb. Evidence from at least 1 other type of quasiexperimental study D Directly based on category IV evidence or extrapolated recommendation from category I, II, or III evidence III. Evidence from nonexperimental descriptive studies, such as comparative studies IV. Evidence from expert committee reports or opinions or clinical experience of respected authorities, or both Wallace, Dana V., et al. "The diagnosis and management of rhinitis: an updated practice parameter." Journal of allergy and clinical immunology 122.2 (2008): S1-S84. Inhaled Corticosteroids in Allergic Rhinitis (2007) Note: allergic rhinitis (AR); budesonide aqueous nasal spray (BANS), fluticasone propionate nasal spray (FPNS), mometasone furoate nasal spray (MFNS), and triamcinolone aqueous nasal spray (TANS); intranasal corticosteroid (INS) Proper management of AR, as with any chronic disease, is determined in part by patients’ acceptance and adherence to their treatment regimen, which is affected by factors such as efficacy, safety, dosing regimens, patient preference, and cost of treatment. Analysis of oncedaily administration of BANS, FPNS, MFNS, and TANS show their clinical efficacy in AR treatment. Although there are a limited number of comparative studies, results suggest that there is little overall difference between INSs in terms of their efficacy. All once-daily INSs (BANS, MFNS, FPNS, and TANS) appear to be well tolerated, with comparable adverse event profiles. Healthy volunteers treated with FPNS did show significantly lower overnight urinary cortisol levels compared with placebo treatment,48 but no significant effects on HPA axis function, markers of bone formation, and white blood cell count were seen with BANS, MFNS, or TANS.49 In the studies reviewed, the four leading INSs (BANS, FPNS, MFNS, and TANS) administered once daily are effective and well tolerated for the treatment of SAR and PAR in adult patients. All four INSs showed similar efficacy. There was little indication of any difference between INSs in systemic effects; however, BANS is the only INS currently rated pregnancy category B and may be preferred for use during pregnancy. The inert ingredients in BANS and TANS are very similar and are likely responsible for the greater patient preference compared with that observed for FPNS and MFNS. Although BANS and TANS may be preferred by a greater percentage of patients based on their attributes, it should be noted that some patients do express a preference for the sensory attributes of FPNS and MFNS. When selecting an appropriate INS for patients, factors preferred by each patient should be considered to help promote patient acceptance of treatment and better adherence to therapy Herman, Howard. "Once-daily administration of intranasal corticosteroids for allergic rhinitis: a comparative review of efficacy, safety, patient preference, and cost." American journal of rhinology 21.1 (2007): 70-79. eCPS (2014) Antihistamines help relieve most symptoms of acute allergic rhinitis such as sneezing, rhinorrhea, nasal itch and conjunctivitis, but are not usually recommended for the treatment of nasal congestion. Desloratadine has demonstrated modest improvement in the symptom of nasal congestion, and is indicated for relief of this symptom.4 There is some evidence to suggest similar results for fexofenadine;5 however, fexofenadine is not indicated for the relief of congestion. Antihistamines are most effective if used prophylactically; however, onset of action is fast enough such that they are also effective when used on an as-needed basis. Once-daily dosing of the newer antihistamines is usually sufficient. Although sedation and anticholinergic side effects are common with the older antihistamines (also known as first-generation or sedating antihistamines), these side effects are usually not seen with newer agents (second-generation or nonsedating antihistamines). Patients who are unaware of sedation may be impaired with respect to attention, memory, vigilance and speed. These effects persist into the next day. Caution is advised in the elderly as they may be more susceptible to the anticholinergic effects of the first-generation antihistamines. Patients whose occupations require vigilance or concentration should receive only nonsedating antihistamines, as they do not affect performance and have no anticholinergic effects.2,6,7,8,9 Of the newer antihistamines, cetirizine is more likely to cause some sedation, especially at higher doses. Patients with hepatic impairment may be at increased risk of adverse effects, and dosage modification may be required (seeTable 2). The currently available second-generation antihistamines have not caused QT c interval prolongation.2 Although older studies of long-term dosing with first-generation antihistamines have demonstrated loss of effectiveness, they are flawed by lack of evidence of adherence to therapy. No loss of effectiveness has been shown up to 1 year. 10 Intranasal corticosteroids are the mainstay of therapy for moderate to severe rhinitis symptoms. Indeed, intranasal corticosteroids as monotherapy have been shown to be more effective than combined use of an antihistamine and leukotriene antagonist.11 They can be given on an as-needed basis in seasonal allergic rhinitis; however, continuous use more effectively provides symptom relief. In addition, they are effective in managing ocular symptoms associated with allergic rhinitis. Newer preparations have a lower spray volume, which may be preferred by some. Budesonide is available as a dry powder nasal inhaler and offers an alternative for those who dislike aqueous sprays. A 2- to 4-week trial may be needed to see maximal effect although benefit is seen in the first day of therapy compared to placebo in controlled trials. Class Antihistamines, Ethanolamines, first-generation Drug Dosage Adverse Effects Drug Interactions Comments Costa diphenhydramine Benadryl Preparations, genericsb Adults and children≥12 y: 25–50 mg TID–QID; maximum4 doses/day or300 mg/day Children 6–<12 y:12.5– 25 mg Q4–6H; maximum 150 mg/day Children 2–5 y:6.25 mg Q4–6H; maximum37.5 mg/day CNS: sedation, fatigue, dizziness, impairment of cognition and performance (the patient may be unaware of impairment).2 Anticholinergic: dryness of the mouth and eyes, constipation, inhibition of micturition, potential precipitation of narrow-angle glaucoma, thickening Increased CNS depression: alcohol, sedatives, tranquilizers, barbiturates. Increased anticholinergic side effects: TCAs, scopolamine. May increase levels of CYP2D6 substrates, e.g., metoprolol, Use with caution in the elderly as they may be more susceptible to side effects such as sedation and syncope. Avoid in patients with narrow-angle glaucoma (increased IOP), urinary obstruction (prostatic hypertrophy), bladder neck obstruction (can cause urinary retention), GIobstruction. Observe infants and young children for paradoxical excitation. Discontinue 3 days before skin testing procedure for allergy. Administer with food to decrease GI distress. Thickening of bronchial secretions. Available in chewable tablets, elixir $ Class Drug Dosage Drug Interactions Comments of bronchial secretions. venlafaxine. and liquid. Increased CNS depression: alcohol, sedatives, tranquilizers, barbiturates. Increased anticholinergic side effects: TCAs, scopolamine. Safe and well tolerated in children. Discontinue 3 days before skin testing procedure for allergy. Metabolite of hydroxyzine. Avoid in patients with a hypersensitivity to hydroxyzine. $ Use at regular intervals. Slow onset (7–14 days for maximal effect). Drug may fail to reach the site of action if excessive nasal mucus secretion or edema of the nasal mucosa is present. May use a vasoconstrictor (intranasal decongestant) 2–3 days prior to the suspension. Aim spray up towards turbinates and away from septum. Liquid forms may be more effective than metereddose inhalers. For the nasal suspension, initial priming needed. Re-prime if not used ≥4 days. $$$$$ Adverse Effects Antihistamines, Piperidines, secondgeneration cetirizine Reactine, genericsb Adults and children >12 y: 5–10 mg/day;maximum 20 mg/day Children 6–12 y:5–10 mg/day 2–6 y: 2.5–5 mg/day 12–23 months: 2.5 mgonce daily; maximum2.5 mg BID Infants 6–11 months:0.25 mg/kg Q12H42 Moderate renal/hepatic impairment: ≥12 y:5 mg/day 6–11 y: <2.5 mg/day Somnolence (with high dose), fatigue, dry mouth, dizziness, headache, diarrhea, nausea, vomiting, pharyngitis. Corticosteroids budesonide Nasal suspension: Adults and children≥6 y (64 µg/metered dose): initial dose 2 sprays in each nostril daily or 1 spray in each nostril BID; may decrease maintenance dose to 1 spray in each nostril daily Nasal powder: Adults and children≥6 y (100 µg/dose): initial dose: 2 applications in each nostril in the morning or 1 application in each nostril BID; maximum 400 µg/day Burning or stinging, nosebleeds. Rhinocort Aqua,Rhinocort Turbuhaler, generics Legend: $ < $10 $$ 10–20 $$-$$$ 10–30 Costa $$$ 20–30 Respiratory Disorders: Allergic Rhinitis; Paul Keith, MD, MSc, FRCPC; Date of Revision: June 2014 Medication Uses Contraindications (CI), drug interactions (DI) or cautions Adverse Effects (common and severe) cetirizine antihistami ne - allergic rhinitis CI: hypersensitivity, severe renal impairment DI: sedatives, alcohol headaches, dry mouth, sleepiness Initial dose; typical dose 10mg; 10mg one time a day Monitoring budesoni de seasonal allergic and allergic/ non-allergic perennial and vasomotor rhinitis CI: fungal or tuberculosis infection DI: cimetidine, ketoconazole, omperazole itching throat, sore throat, cough, fatigue, nausea, dizziness, and headache 100g/metered dose nasal spray; 2 sprays per nostril one time a day diphenhy dramine antihistami ne – allergic reactions, upper respiratory allergies CI: neonates and premature infants, breast feeding DI: MAOIs, Sedatives sedation, sleepiness, dizziness, disturbed coordination, epigastric distress, thickening of bronchial secretions, drug rash, hypotension, hemolytic anemia, urinary frequency 25mg; 25-50mg CBC with every 6 hours differntial, or as needed LFTs, RFT