Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
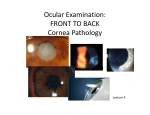
Corneal dystrophies & other miscellaneous corneal conditions MBBS KGMU Common corneal disorders • Keratitis/ corneal ulcer. • Corneal trauma. • Keratomalacia. • Ectatic conditions. • Corneal dystrophies. • Corneal degenerations. Differences between dystrophy & degeneration Corneal dystrophy • Bilaterally symmetrical. • Often hereditary. • Limited to a particular corneal layer. • Non-inflammatory. Corneal degeneration • Non-hereditary. • Usually unilateral sometimes bilateral. • Not strictly limited to a particular corneal layer. • Non inflammatory Corneal dystrophies Corneal Dystrophies • Epithelial & sub-epithelial. • Bowman’s membrane. • Stromal. • Endothelial. Epithelial, sub-epith & Bowman’s corneal dystrophies • Epithelial & sub-epithelial – manifest in adults. • Epithelial basement membrane dystrophy. • Meesman dystrophy. • Bowman’s layer dystrophies – manifest in childhood. • Thiel Behnke corneal dystrophy. • Reis-Bucklers corneal dystrophy. Comparison between epithelial, subepithelial, Bowman’s dystrophies • Similarities: • Symptoms: • Asymptomatic / associated with recurrent corneal erosions. • Foreign body sensation & watering. • Treatment by PTK –photo-therapeutic keratectomy by EXCIMER LASER. • Difference: Slit lamp examination shows patterns typical for each one. Meesman’s dystrophy (intra-epithelial microcystic appearance) Stromal Dystrophies • Granular form • Lattice form • Macular form Bilateral. Manifest at puberty. Diminution of vision is the presenting complaint. Central cornea. Granular stromal dystrophy AD. Crumb-like accumulation of hyaline material Lattice dystrophy (AD. Criss-cross lines). Macular Dystophy AR Opacities dispersed throughout stroma. Endothelial dystrophies • Fuchs endothelial dystrophy – AD. Elderly. • CHED – Congenital hereditary endothelial dystrophy. AD/AR. • PPMD –Posterior polymorphous dystrophy. AD. Features common to all endothelial dystrophies • Limbus-to-limbus corneal clouding • Bilateral. • Endothelium is attenuated or even absent • Oedematous cornea may be 2-3 times normal thickness. • Generalised haze or diffuse ground glass appearance. • Photophobia and lacrimation in late stages due to bullous keratopathy. Specular microscopy in endothelial dystrophy Normal endothelim Decreased cell count, pleomorphism, polymegathism Congenital hereditary endothelial dystrophy (CHED) • Autosomal dominant (later in infancy). • Autosomal recessive • Earlier presentation (at birth; nystagmus). CHED Posterior polymorphous dystrophy • Autosomal dominant. • Bilateral. • 2nd or 3rd decade….rarely -in early infancy. • Vesicle like lesions in non-banded part of Descemet’s membrane. • Periph ant synechiae & raised IOP may be present. Management of endothelial dystrophies • Specular microscopy – for endothelial cell count. • Pachymetry –corneal thickness. Treatment required if symptomatic. Symptomatic treatment: • Hypertonic saline eye drops. • Bandage contact lens. Definitive treatment: Endothelial keratoplasty (DSAEK). Penetrating keratoplasty. Corneal degenerations Corneal degenerations • Arcus senilis / juvenilis. • Band shaped keratopathy. • Terriens marginal degeneration. • Salzmann nodular degeneration. • Spheroidal degeneration. Arcus senilis Terrien marginal degeneration • Bilateral. • Progressive thinning of superior peripheral cornea. • No inflammation. • Presents with myopia or astigmatism. Band shaped keratopathy • Horizontal opacification in palpebral aperture. • Chronic uveitis, silicon oil. • Blind shrunken eyes. • Hyperparathyroidism, sarcoidosis. • Treatment – chelation with EDTA. • PTK ?? Ectatic conditions Ectatic conditions (non inflammatory) • Keratoconus. • Pellucid marginal degeneration. • Keratoglobus. Keratoconus • Congenital weakess of corneal collagen. • Conical shape of cornea because of central thinning and bulging (Munson sign). • Manifests after puberty. • High myopia & astigmatism. • Treatment options: • Rigid contact lens. • Corneal cross linking (C3R). • Keratoplasty. Keratoconus Pellucid marginal degeneration • Painless bilateral thinning of inferior peripheral cornea. • Myopia & astigmatism. • It is probably a variant of keratoconus. Keratomalacia Keratomalacia • Bilateral. • Rapidly increasing clouding of cornea. • No congestion. • Melting of cornea. • Night blindness +/• Other features of malnutrition / diarrhoea. • Timely injecs of Vit A & control of malnutrition. Corneal injuries • Best possible repair also ends up in subnormal visual gain. • Timely keratoplasty is required in visually significant opacity to prevent amblyopia. • Donor tissue selection should be very carefully done - good endothelial count. Need of the hour • Proper education of medical personnel, school teachers and health workers regarding causes and prevention of childhood blindness. • Training of medical personnel at primary and secondary health care centres regarding early diagnosis of treatable conditions and suitable management. • To know ‘when to refer’ to higher centre. • Over-the-counter sale of corticosteroid eye drops to be stopped. Our students are the future of this beautiful institution Do your best always text