Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Polysubstance dependence wikipedia , lookup
Neuropharmacology wikipedia , lookup
Pharmacognosy wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Prescription costs wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Drug interaction wikipedia , lookup
Paracetamol wikipedia , lookup
Pharmacogenomics wikipedia , lookup
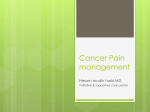
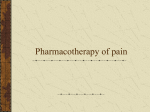
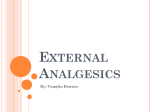
SF September 2012_Sept 2004.qxd 2012/09/12 6:00 PM Page 49 Pain Compound analgesics and the management of pain Prof CL Odendaal Department of anaesthesiology University of the Free State, Bloemfontein Introduction Despite advances in modern medical and supplementary therapies, the numbers of patients who are suffering from pain are still very high. Albert Schweitzer once said: “We must all die. But that I can save him from days of torture, that is what I feel as my great and ever new privilege. Pain is a more terrible lord of mankind than even death itself.” The definition of pain as defined by the International Association for the Study of Pain (IASP) involves sensory and emotional experiences, with or without actual tissue damage. In modern surgery we all strive to achieve ‘balanced anaesthesia’ but the concept of ‘balanced analgesia’ has also been propagated. Possibly this concept led to the development of the ‘multi-substance analgesics’ or ‘multi-compound analgesics’ that have overflowed the markets in SA. SA has the highest number of multicompound analgesics in the world, and it must be asked if this is good or bad. Goals of treating pain • • • • Initiate the safest, simplest, most cost effective therapy Multiple substance therapy is at the same time a ‘shotgun’ approach and makes it impossible to evaluate an individual therapy aimed at safety and efficacy Therapeutic goals must be education and determination to achieve minimisation of pain Treat but do not over-treat. What do we want to achieve? The objective of treating pain is to have the concentration of the substance varying in the therapeutic window of the body (see Figure 1). The Specialist Forum | September 2012 Figure 1 This is easily obtained in post-operative pain by using a PCA-apparatus where the patient controls his/her own pain by pressing a button. However, it is also possible to maintain an effective blood concentration by administering the drug orally at specific time intervals e.g. four hourly, six hourly or eight hourly for 24 or 48 hours. Reassess the situation again and if not effective, change either the time interval or the dose for the next controlled period. When the concentration goes above the line, side effects will occur or below the line, it will be ineffective. Classification of pain Pain is usually classified as acute, chronic and cancer pain. It can be also be classified as nociceptive pain or neuropathic pain, which will make pharmacological treatment more understandable. Nociceptive pain occurs when there is tissue damage with the release of the so-called ‘inflammatory soup’. The release of these substances either stimulate the free nerve endings directly or indirectly through the action of mediators on the nociceptors. Important here is that the pain pathways in these types of pain are intact. Conduction of impulses is usually through the fast tracts or Ad fibres and also by, to a certain extent, the c-fibres. For the treatment of such pain, one should adhere to the basis of the WHO Analgesic ladder. Stuck to the principle of the ladder, pain can be effectively treated in 80-90% of pain sufferers. Page 49 SF September 2012_Sept 2004.qxd 2012/09/12 6:00 PM Page 50 Pain Compound analgesics and the management of pain Neuropathic pain is a type of pain in which there is definite dysfunction or damage to the pain pathways. These are usually conducted by c-fibres. Ordinary analgesics and NSAID’s have little or no effect. This type of pain is usually treated with the first generation antidepressants e.g. amitryptaline or the anticonvulsants e.g. carbamazepine or lately the GABA-agonists, gabapentin or pre-gaballin. Pathophysiology of pain Pain is caused by the stimulation of free nerve endings called nociceptors. Nociceptors present as: • Somatic nociceptors - in the skin and connective tissue • Visceral nociceptors - intra-abdominal or pelvic tissue. Nociceptors may be stimulated by: • Physical stimuli - pressure, heat or visceral distension • Chemical stimuli - due to tissue damage or inflammation. Tissue damage results in the production and accumulation of algesic substances which have been shown to affect nociceptors. Such substances are prostaglandins, bradikinin, serotonin, histamine, potassium and hydrogen ions. Figure 2 Stimulation of these nociceptors causes impulses to be carried along the peripheral nerve to the Wide Dynamic Range cells in the dorsal horn of the spinal column. In the dorsal horn, a synapse is formed with cells of the spino-thalamic tract. They carry impulses up the spinal cord, through the brain to the thalamus where the next synapse is formed. From the thalamus, impulses are delivered to several areas of the cerebral cortex where ‘pain’ is interpreted. Page 50 The dorsal horn is the major site of pain modulation. This is the site where the mechanism of the ‘Gate-theory’ by Wall and Melzack is applied. This is a complex system of interneurons which may be inhibitory or facilitatory. The inhibitory neurons have endorphins as neurotransmitters. Facilitatory neurons have sP (substance P) as neurotransmitter. Too often patients are labelled as neurotic, hysterical or over-reactors because of the lack of understanding of pain and realising that there is a scientific basis for individual variation in the perception of pain. Figure 3 Treatment regimens Pain should be treated starting with the first step of the ladder or basic substance e.g. paracetamol. Dosage: 300-1000mg every 4-6 hours. Daily dose should not exceed 4-6g per day. If that isn’t successful, a NSAIM or a weak opioid could be added. Best example of this is a combination of paracetamol + codeiene; a very effective analgesic. Dosage: paracetamol 450 mg + codeine 30 mg. Dolorol Forte. A still stronger analgesic could be the combination of the three steps above e.g. paracetamol, codeine and ibuprofen. Here we have a • Central-acting drug: paracetamol; • m-receptor-agonist: codeine • peripheral acting drug: NSAIM viz ibuprofen. The above-mentioned combinations are logical and very effective. Any pain caused by tissue damage can be treated with this in mind. Pharmacology Paracetamol Central acting analgesic and antipyretic drug used for mild to moderate pain. The mechanism of action of paracetamol still remains unresolved. The greater sensitivity of cells containing COX-3 to paracetamol is currently accepted as the action of paracetamol. September 2012 | The Specialist Forum SF September 2012_Sept 2004.qxd 2012/09/12 6:00 PM Page 52 Pain Compound analgesics and the management of pain It was shown that paracetamol inhibits neural cells that have a low synthesis rate and containing low levels of peroxide. It appears that when arachidonic acid levels are low paracetamol acts as a specific COX-2 inhibitor. Thus paracetamol has predominant effects on cells in the CNS because peroxide levels and arachidonic levels are lower than in the peripheral tissues where an inflammatory process may be going on. Although it has been accepted as a safe analgesic, the incidence of hepatic toxicity has risen during the past few years due to over dosage. This happens as a result of ingesting 5-8g daily over an extended period of time. Side effects: • • • • anorexia nausea and vomiting later jaundice increase in AST and ALT liver enzymes. Drug interactions • Favourable with NSAIDs and opioids works synergistically. Non-steroid anti-inflammatory drugs These drugs are used regularly alone or in combination with other analgesics. The effects of these drugs are as follows, and may appear in a more or lesser degree with all the NSAIDs. • These drugs alter the nociceptive response caused by bradykinin • Inhibit prostaglandin E synthesis • Have a direct analgesic action on higher centres • Reduce platelet aggregation • May cause hypoprothrombinaemia • Reduce body temperature in low dosages • Reduce blood sugar concentrations. • Induce acid-base imbalance and acidosis. Included in the group are: lornoxicam (Xefo®), indomethacin (Indocid®), ibuprofen, diclofenac (Voltaren®). These agents are used mainly for treatment of skeletal pain. Selective COX-2 inhibitors (Celecoxib, Etoricoxib) inhibit only the COX 2 enzyme thus have less side effects on platelet and renal function. Codeine This is an opiate with the same m-receptor action as morphine. Its action is approximately 10% of that of morphine. It is extremely well absorbed orally. It is used in mild to moderate pain. Page 52 Side effects • • • Serious additive effects with phenothiazines, tranquilisers, sedative-hypnotics, alcohol Respiratory depression, hypotension, profound sedation with over-use Dependency. Combination drugs The main reason for development of combination drugs is to gain efficacy, reduce toxicity, interact pharmaco-kinetically and dynamically or both, positively or negatively. Thus, combinations should display either additive or synergistic analgesia in which a lower dose of each substance should increase efficacy without harm to the patient. 1 Combinations in all literature are aimed at analgesic receptors only i.e.: • opioids - μ receptors • paracetamol - central PGE3 • NSAIDs - peripheral • Tramadol - partial opioid + antiserotonin and noradrenaline inhibitor effects. Until recently only a few oral combinations were approved in US by the FDA containing only opioids and/or NSAID’s i.e. ibuprofen and hydrocodone. The WHO recognise the efficacy of combinations and based on extensive evidence of the 200 top prescribers only nine opioid/acetaminophen/NSAID combinations were recommended by WHO for treatment of moderate severe pain. SA is the country with the most multi-substance analgesics in the world. It contains analgesics and many other substances. Almost every firm produces its own version of ‘the best analgesic’. There are 89 different multisubstance analgesics in SA.These tablets/capsules contain a wide variety of substances that have nothing to do with management of pain i.e. antihistamines. The question can therefore be asked: is this ‘the good, the bad or the ugly?’ No single analgesic is perfect and no single analgesic can treat all types of pain. Yet each agent has distinct advantages and disadvantages compared to others.2 Already in 1998 it has been stated that many of the combination analgesic preparations available in South Africa are patently irrational, that their efficacy as analgesics is suspect, that their potential toxicity is great, and that a potential for abuse exists because of their `psychic cocktail’ constituents.3 September 2012 | The Specialist Forum SF September 2012_Sept 2004.qxd 2012/09/12 6:00 PM Page 53 Pain Compound analgesics and the management of pain Rational combinations of analgesic drugs offer a viable approach to managing persistent pain that involves multiple sites or pathways.4 Pharmacology of substances used in combination drugs in South Africa Propoxyphene This drug has now been banned in most of the countries of the world. In South Africa there was also huge outcry. The case still continues. Propoxyphene is a relatively weak opioid. The weight of evidence to the recommended doses of propoxyphene states that it is no more and probably less effective than the usual doses of paracetamol, aspirin or any other NSAID. Bearing this in mind, it must be appreciated that the adverse effects are dose dependent and as far as for the other opioid analgesics, include the risk for dependence and abuse. Over dosage is a serious problem and has proved fatal. Overdose causes respiratory depression and cardiac dysrhythmias. Accumulation of an active metabolite has local anaesthetic effects. DXP is a more potent LA than propoxyphene, and is more potent than lignocaine. It is this metabolite that is responsible for cardiac dysrhythmias because of its potent cardiac membrane and Na+ channel blocking effects. It has the characteristics of Vaughn-Williams, class 1c classification. It is also not reversible by naloxone. Most dangerous aspect of DPX is the active metabolite - norpropoxyphene which is highly cardiotoxic; it blocks both IK & hERG channels (K+), leading to QT interval prolongation, leading to torsade des pointes and sudden death. It is doubtful that propoxyphene hydrochloride 65mg provides an analgesic effect equal to that of 650mg aspirin In a critical analysis of information on propoxyphene that has been published since the drug’s introduction, the following conclusion has been reached: It is doubtful that propoxyphene hydrochloride 65mg provides an analgesic effect equal to that of 650mg aspirin. There is no conclusive evidence that combinations of propoxyphene with other analgesics are more effective than propoxyphene alone or even other analgesics alone. Caffeine Caffeine is a methylxanthine structurally related to theophylline. It is a stimulant and has been used to restore mental alertness and wakefulness. It is well absorbed from the gut with peak levels occurring within 15-45 minutes. Elimination half-life is approximately 3-5 hours. It is also recognised as an effective analgesic adjunct. There is some evidence that IV caffeine sodium benzoate or even oral caffeine preparations may have some efficacy in the treatment of PDPH. Side effects • • • • • • • Gastrointestinal disturbances Nervousness Diuresis Irritability Dysrhythmias, tachycardia and palpitations Tremulouses Muscle twitching. Meprobamate Carbamate derivative. Used as anxiolytic. Doses: 1.2-1.6g per day given in 3-4 divided doses. Elimination half-life is 6-18 hours. Serum concentrations in excess of 12mg/dl are associated with coma. Meprobamate has been reported to have some muscle relaxant properties with associated pain relief in the treatment of musculoskeletal symptoms. However, many reports have indicated that other agents are much more effective in the treatment of these symptoms.5 Adverse effects Propoxyphene interacts with several other drugs through inhibition of liver enzymes and there have been occasional reports of jaundice with its use. Fatal interactions are with carbamazepine and alcohol in normal dose range. The Specialist Forum | September 2012 • • • • • • Thrombocytopenia Leucopoenia Agranulocytosis Hypotension Drowsiness Dizziness Page 53 SF September 2012_Sept 2004.qxd 2012/09/12 6:00 PM Page 54 Pain Compound analgesics and the management of pain • • • • Vertigo Seizures Blurred vision Cutaneous reactions. Most serious side effect is the potent addiction potential with marked withdrawal reactions. This makes it a dangerous drug.6 Phenyltoloxamine/ diphenhydramine Effective antihistaminic drugs. Although phenyltoloxamine has been associated with independent analgesic activity and adjuvant analgesic effects in combination with acetaminophen, the benefits achieved with the drug in most were minimal and of questionable clinical importance.7 The conventional combination of phenyltoloxamine/acetaminophen 60/650 mg offers no advantage over maximal doses of acetaminophen alone (1g). As a matter of fact, in a study of post-oral surgery patients, the combination as mentioned above was less effective than acetaminophen alone. Improvement seen with its use may be due to the sedative effects in settings where anxiety or tension is a component of the pain picture. Side effects • • • • • • • Drowsiness Dizziness Gastrointestinal disturbances Blurred vision Tachycardia Diaphoresis Atrio-ventricular heart block. Orphenadrine Indicated for relief of pain associated with acute musculoskeletal conditions. With the addition of acetaminophen 450mg and orphenadrine 35mg tds effective analgesia was encountered in myalgia secondary to tension of the cervical and upper thoracic muscle spasm. It should be used alone and no other analgesics added.8 Adverse effects • • • • • • • • • Light headedness Syncope Dizziness Mental confusion Drowsiness Hallucinations Agitation Tremor Dependence (Shariatmadari, 1975). Combination therapy Combinations of drugs with different analgesic properties. Literature reports confirm beneficial effects with opioid/NSAID combinations. • Fewer opioid dosages • Reduced opioid requirements • Shorter duration of post-operative opioid therapy • Significant increases in analgesic potency • Combinations more effective than single agents alone • Reduced adverse effects. Combinations with other substances The multi-substance combinations are sometimes totally illogical and include substances which have no proven benefit. These compounds may be harmful and can worsen the patient’s condition. The most often used drugs include pemoline, propoxyphene, meprobamate, caffeine and diphenhydramine. Diphenhydramine is known to delay absorption of other orally administered drugs.9 Conclusion We should seriously rethink our management of pain - acute/chronic. The prescription should be scientifically and pharmacological correctly worked out. Most importantly always keep side effects in mind. I am not asking you to stop prescribing. I am asking you to think about what you are giving your patient. Do you know what the effects are? Do you know what the side effects are? Hippocrates, the father of medicine said, “Above all, do no harm.” Remember, no drug in the world is free of side effects, even the ‘doctor’s friend’. Be careful. References 1. Raffa RB, Pergolizzi JV, Tallarida RJ. “The determination and application of fixed-dose analgesic combinations fot treating multimodal pain. The Journal of Pain; Vol11; No 8, 2010. 701-709 2. Raffa RB, Pharmacology of oral combination analgesics: rational therapy for pain. J of Clin Pharmacy and Therapeutics. 2001, 26, 257-264 3. Truter I; “An Investigation into Compound Analgesic Prescribing in South Africa, with special emphasis on Meprobamate-containing Analgesics. Pharmacoepidemiology and Drug Safety; 7: 91-97 (1998) 4. Raffa RB, Clin Rheumatol; 2006, 25 (Suppl 1): S9 – S15 5. Winkelman & Richards, 1975 6. Truter I; “An Investigation into Compound Analgesic Prescribing in South Africa, with special emphasis on Meprobamate-containing Analgesics. Pharmacoepidemiology and Drug Safety; 7: 91-97 (1998) 7. Raffa RB; Antihistamines as analgesics. J of Clinical Pharmacy and Therapeutics; 2001; 26, 81-85 8. Hoivik & Moe, 1983 9. Raffa RB; Antihistamines as analgesics. J of Clinical Pharmacy and Therapeutics; 2001; 26, 81-85 • SF Page 54 September 2012 | The Specialist Forum