Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Management of acute coronary syndrome wikipedia , lookup
Cardiac surgery wikipedia , lookup
Coronary artery disease wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
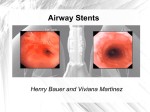
Technical Developments and Instrumentation Feasibility of a Technique for Branch Pulmonary Artery Stent Implantation1 Olga H. Salazar, MD Kimberly A. Krabill, MD David W. Hunter, MD Michael 5 . Vance, MD Albert P. Rocchini, MD Index terms: Children, cardiovascular system, 59.1552,944.7229 Interventional procedures, in infants and children, 944.1268 Pulmonary arteries, stenosis or obstruction, 59 1552,944.7229 Stents and prostheses JVIR 1996; 7:41-46 ' From the Divisions of Pediatric Cardiology (O.H.S., K.A.K.,M.S.V.,A.P.R.)and Radiology (D.W.H.), University of Minnesota Hospital and Clinic, Box 94-UMHC, 420 Delaware S t SE, Minneapolis, MN 55455. Received March 29, 1995; revision requested May 24; revision received July 17; accepted July 20. Address correspondence to O.H.S. O SCVIR, 1996 BALLOON-expandable stainless steel stents have become a n important tool in the treatment of stenosis in branch pulmonary arteries. Previous reports have described the safety and efficacy of use of these stents (Palmaz stent; Johnson & Johnson Interventional Systems, Warren, N J ) in the treatment of congenital heart disease (1-6). The current delivery technique is complicated by the inability to advance a large sheath or stent across branch pulmonary arteries that are severely stenotic. I t is also complicated by kinking of the sheath during stent passage, which results in a long procedure time and may cause premature dislodgment of the stent from the balloon catheter. The use of a 10- or 11-F sheath precludes stent placement in many small children. This study describes a n alternative method of endovascular stent implantation t h a t can help resolve some of these technical difficulties. This method is especially useful in smaller patients, in whom venous access is frequently a problem. The purpose of this study was to evaluate the efficacy and safety of a method of endovascular stent implantation in a dog model and to determine the feasibility of using this alternative technique in children with stenosis of a branch pulmonary artery. METHODS The method presented here and old methods of stent delivery initially were assessed in nine mongrel dogs that weighed 12.9-20.2 kg. Isolated stenosis of the left pulmonary artery was created by placing two pieces of 2-0 Vicryl suture (Davis & Geck, Wayne, NJ) around the branch pulmonary artery (3). The sutures were tightened so that the pulmonary artery was narrowed 40%-50%. After surgery, all dogs were given intramuscular antibiotics for 3 days to prevent infection, and they were given morphine sulfate to prevent pain. Cardiac catheterization was performed 3-6 months after the creation of t h e stenosis, with the dogs under anesthesia. After the stenosis was hemodynamically and angiographically assessed, stent placement was attempted (Fig 1). Five dogs were randomly assigned to treatment with the old method, and four were assigned to the new method. The animal component of this study conformed to the guiding principles of the American Physiological Society (7). In determining the efficacy of the method, two factors were evaluated: The first was the ability to place a stent. The second was the time required for stent placement, which was defined as the time that elapsed from the placement of a n exchange guide wire in the branch pulmonary artery to the expansion of the stent across the stenotic lesion. Old Method of Stent Delivery In the old method, a 0.038-inch Amplatz Superstiff Teflon-coated exchange wire (Medi-tech/Boston Scientific, Watertown, Mass) was positioned in the distal branch pulmonary artery. An 11- or 12-F long sheath (Mullins sheath; USCI Angiographic Systems Division, C R Bard, Billerica, Mass) and a dilator were advanced beyond the stenosis, and the dilator was removed from the sheath. The P308 Palmaz stent was mounted on a n 8-10-mm polyethylene balloon catheter ( ~ e d i - t e c h b o s t b nScientific) and was advanced through the sheath until it reached the site of stenosis in the branch pulmonary artery. An 11-F sheath was used for the 8-mm balloon catheter, and a 12-F sheath was used for the 10-mm balloon catheter. The balloons selected were the same size a s or slightly larger than the diameter of the pulmonary artery distal to t h e stenosis. The sheath was partially withdrawn over the stent, and centering of the stent across the stenosis was confirmed by means of a small injection of contrast material into the sheath. The sheath was then withdrawn completely from the stent, and the balloon was inflated until the stent was fully expanded. The balloon was withdrawn, and if necessary, a 42 Journal of Vascular and Interventional Radiology January-February 1996 Figure 1. Angiograms show (a) isolated left pulmonary artery stenosis (arrowhead) surgically created in a dog and (b) a stainless steel stent (arrowhead) placed at the site of a previously created left pulmonary artery stenosis. r, a. Table 1 Patient Demographic and Technical Data Patient No./Sexl Age (y) Weight (kg) Diagnosis Approach Type of Sheath Size of Olbert Balloon l"M2.3 1*M2.5 2M3.0 3M3.5 4M4.5 10.2 10.6 13.4 13.5 16.3 TOF PA TOF PA PO Glenn anastomoses PO Glenn anastomoses PO Glenn anastomoses RFV RFV RIJ LIJ RIJ 8-F Mullins 8-F Mullins 7-F Cordis 7-F Cordis 7-F Cordis 81415.8190 81415.8190 81415.8190 81415.8190 81415.8190 5Fl15.5 6M15.0 51.3 56.5 PPS PO HT RFV RFV 8-5' Mullins 8-F Mullins 81415.8190 81415.8190 Size and Type of Redilation Balloon 101417175VC 1014/7/75 VC 101417175VC 1014/7/75 VC 1214171100 BX 1214/7/100 BX 1214171100 BX Note.-BX = Blue Max, HT = heart transplant, LIJ = left internal jugular vein, PA = pulmonary atresia, PO = postoperative, PPS = peripheral pulmonary stenosis, RFV = right femoral vein, RIJ = right internal jugular vein, TOF = tetralogy of Fallot, and VC = Vast-cath. *Data in regard to stent placement in the right (row 1)and left (row 2) pulmonary arteries in patient 1 are given. larger angioplasty balloon was used to further dilate the stent. The balloon was then deflated and exchanged for an endhole catheter, and the expanded stent was left across the area of stenosis. Repeated hemodynamic and angiographic evaluations were performed. New Method of Stent Delivery In the new method, a 0.035-inch Superstiff exchange guide wire was positioned in the distal pulmonary artery well across the narrow area. The Palmaz stent was mounted by hand onto an 01bert 81415.8190 (balloon outer diameter [millimetersl/balloon length [centimeters1French sizelusable length [centimeters]) balloon catheter (Meadox Medicals, Surgimed, Oakland, NJ) and was pressed firmly onto the middle of the balloon. The Olbert balloon catheter is made of a material that allows a tight bond to be formed between the stent and the balloon and thus makes premature dislodgment of the stent from the balloon almost impossible. The Palmaz P308 stents were 3 cm long with a 3.4mm nominal outer diameter (Table 1). A Touhey-Borst type of adapter (Intenentional Medical, Subsidiary of Medtronic, Danvers, Mass) was Luer-locked to the sheath hub to prevent movement of the balloon catheter and to permit injection of the contrast medium into the sheath to confirm stent position (Fig 2). The stent mounted on the Olbert balloon catheter was preloaded into an 8-F long sheath (Mullins sheath), and this unit was advanced into the stenosis in the distal pulmonary artery. The sheath was withdrawn and the stent was deployed in a fashion similar to that used in the old method. If the pulmonary artery distal to the stent was greater than 8 mm in diameter, then the stent was dilated further by advancing a 10-mm balloon catheter (Opti-Plast; Vas-Cath, Mississauga, Ontario, Canada) over the exchange guide wire. After we had demonstrated its efficacy in the dog model, we used this method to place seven stents in six children (five boys, one girl) with stenosis of a branch pulmonary artery. The patients were aged 2.3-15.5 years (mean, 6.6 years f 5.9 [standard deviation]), and weighed 10.2-56.5 kg (mean, 24.5 kg 20.2). Informed consent was obtained from all patients (Table 1). The study protocol was approved by the institutional committee on human research. All patients who had stenosis or hypoplasia of a branch pulmonary artery * Salazar et a1 - 43 Volume 7 Number 1 Statistical Analysis All data are presented as the mean f standard error. Statistical analysis was performed with the unpaired Student t test. I RESULTS Figure 2. Photographs of the Palmaz stent mounted on an 8-mm Olbert angioplasty balloon catheter. (a) Combination of preloaded Olbert balloon, Palmaz P308 stent, and 8-F sheath is shown. A Y hemostatic valve was attached to the sheath hub to prevent movement of the catheter. (b) Palmaz P308 stent is mounted on an 8 mm x 4 cm Olbert balloon catheter on a 5.8-F shaft. were considered eligible. Diagnoses included tetralogy of Fallot with pulmonary atresia, univentricular heart physiology and a previous caval-pulmonary anastomosis, isolated branch puln~onary artery stenosis, and in one patient branch pulmonary artery stenosis after heart transplantation (Table 1). Patients 1 , 4 , and 5 underwent numerous procedures during which both balloon and surgical angioplasty were used to try to enlarge and unifocalize their hypoplastic pulmonary arteries before stent placement. Patients 2, 3, and 4 had surgically induced stenoses of branch pulmonary arteries after aortopulmonary shunt placement and had previously undergone unsuccessful attempts to enlarge their stenotic pulmonary arteries with both balloon and surgical angioplasty. The patients were examined clinically and appropriate laboratory studies were obtained before cardiac catheterization. Right heart catheterization was performed from the femoral approach in four patients and from the left internal or right internal jugular vein in three patients with Glenn anastomoses (Table 1). The areas of stenosis were defined with angiography. Systemic anticoagulants were administered routinely by means of a heparin bolus (100 Ukg). After stent placement, all patients were given 80 mg of aspirin per day for 1 month. A specially ordered 8-F Mullins long sheath (80 cm long) was used when the femoral vein approach was employed. When the internal jugular vein approach was used (patients with Glenn anastomoses), a 7-F, 23-cm-long Cordis Plus sheath (Cordis, Miami, Fla) was used (Table 1). Redilation was performed with a balloon catheter with a larger diameter when indicated. Opti-plast 10/4/7/75 and BlueMax 12/4/7/100 balloon catheters (Medi-tech/Boston Scientific) were used for redilation to 10 and 12 mm, respectively (Table 1).When redilation with a larger balloon catheter was required, the long sheath was exchanged for a balloon catheter with a larger diameter; this catheter was advanced directly through the skin, without a sheath. All stents were dilated to a size equal to or slightly greater than the diameter of the pulmonary artery distal to the stenosis. In patients 1 and 2, the stents developed stenoses because of patient growth and were successfully redilated to a larger size 2-3 years after the original stent placement. Experimental Data Before stent placement, the peak systolic gradients across the stenoses were similar in the two groups of dogs (Table 2). Stents were placed successfully in three of five dogs with the old method and in four of four dogs with the new method. The old method failed in one dog because we were unable to advance the large sheath from the right ventricular outflow tract and across a distal pulmonary artery stenosis; it failed in the second dog because we were unable to advance the stent through the sheath at the level of the stenotic pulmonary artery, despite previous dilation with an 8mm angioplasty balloon catheter. In both of these dogs, the stents were successfully placed by means of second catheterization with the new method. In all cases in which stent delivery was successful, the gradient across the stenosis was abolished. They were no major complications associated with stent placement with either method. Significantly less time was required for stent placement with the new method (13 minutes k 3) compared with the old method (39 minutes k 5) ( P = ,009). Dogs in whom the stent could not be placed with the old method were not included in this analysis of time. Patient Data Seven stents were successfully delivered in six patients with stenoses of branch pulmonary arteries by using the new method. Stent placement resulted in a significant reduction in systolic gradient across the stenosis (from 37 mm H g k 3 9 to l l m m H g + 1 6 ) a n d a marked increase in vessel diameter (from 3 mm + 1 to 9 mm f 2) ( P < .001). The time required to place the stents in these children ranged from 7 minutes f 18 to 13.5 minutes 2 (mean, 13 minutes f 4) (Table 3). There were no complications related to the procedure. + I DISCUSSION In 1985, Julio Palmaz and colleagues (8) developed an expandable intraluminal graft in an attempt to overcome the elastic recoil that occurs in lesions refractory to balloon dilation. Balloon-ex- 44 Journal of Vascular and Interventional Radiology January-February 1996 pandable intravascular stents were initially used to support vessel walls in coronary arteries in adults (9). In 1988, Mullins et a1 (1)and Charnsangavej et a1 (10) . . evaluated the efficacv of im~lantinn expandable stents in pulmonary arteries and systemic veins. Twenty-seven balloon-expandable stents were placed in 13 mongrel dogs with good results and few complications. In 1991, O'Laughlin et a1 (2) described the successful placement of 36 stents in 23 patients with stenoses of branch pulmonary arteries and reported a substantial reduction in the pressure gradient and an increase in vessel diameter. The feasibility of repeated dilation of the Palmaz stent in growing pulmonary arteries was recently studied by Trerotola et a1 (6). They placed 23 stents in 20 newborn lambs and redilated the Palmaz stents after 4 months, when vessel growth had created a stenosis. The process of repeated dilation of stents in pulmonary arteries proved to be relatively straightforward, without major complications. A more recent report on intermediate follow-up after endovascular stent placement in patients with congenital heart disease described a combined experience in 85 patients in Houston and Boston who underwent placement of 121 stents (5). Follow-up revealed stent fracture in one patient, restenosis in one patient, and sudden death in one patient. There was no statistically significant change in luminal diameter or pressure madient at follow-up catheterization (average of 8.6 months after stent placement) compared with findings at immediate postimplantation catheterization. Redilation was performed in 14 patients (mean of 10.2 months after implantation) who had stenoses with a residual waist or who needed a larger arterial diameter, with good results. Some of the problems associated with the current technique of stent placement are related to technical difficulties in delivering the stent to the area of stenosis. These problems are also related to the large size of the sheath required, which results in limitations on venous access in smaller patients. In the past, patient selection has been important, with the most favorable candidates being adults or adolescent-sized patients because of technical ease of implantation and ability to dilate the stent to,a size appropriate for an adult (5). We conducted the animal study to determine the feasibility of this new technique of stent placement, and we com- Table 2 Experimental Results in a Dog Model Old Method New Method P 16f2 25f 2 16f3 26 2 + NS NS 0.3 f 0.6 0.3 f 0.5 NS 60% (3 of 5) 38.3 f 6 100% (4 of 4) 12.3 3 ,009 L, Mean weight of dogs (kg) Gradient before stent placement (mm Hg) Gradient after stent placement (mm Hg) Success rate Time ( m i d * + ... Note.-NS = not significant. *The time required, after placement of a Superstiff exchange guide wire into the branch pulmonary artery, to position the expanded stent across the stenotic lesion. pared our ability to place the stent and the time required for stent placement with each method. We chose a randomized study design to eliminate investigator bias in the selection of animals for each group and to ensure that the experience of the cardiologist with the various stent-placement techniques did not bias the results. All stents were positioned by one primary operator (A.P.R.) with an assistant (O.H.S., D.W.H., M.V., or K.A.K.). Until 1991 when we completed the animal component of this study, the old method was the standard technique used for endovascular stent implantation at our institution. We did not perform a randomized trial comparing the old and new methods in patients because of the success of the new method in our animal studies and the small number of patients who undergo this procedure. The new technique was especially advantageous in smaller patients, in whom the low-profile balloon catheter permitted the use of a smaller sheath. The use of the smaller sheath was especially desirable in the patients with a Glenn anastomosis in whom placement of a P308 stent from an internal jugular approach was required. The results of this method of placing stents in branch pulmonary arteries appear to be encouraging. By using the stent-mounted balloon catheter as the "dilator" for the sheath and simultaneously advancing the sheath, balloon, and stent into the branch pulmonary artery, the time required for the procedure is decreased and stent delivery to even severely stenotic vessels is facilitated. Problems such us kinking of the sheath during stent passage and dislodgment of the stent from the balloon catheter are essentially eliminated. We have not en- countered any stent-related complications such as distortion fracture or stress fatigue as a result of reexpansion of the stent after it has been crimped onto the 8-mm, 5.6-F-shaft Olbert balloon catheter. The use of a smaller balloon did not interfere with our ability to redilate the stent up to 12 mm when indicated. In older patients in whom redilation of the stents to 15 or 18 mm may be indicated, the 8-F long sheath can be exchanged for a larger-diameter balloon catheter, which is advanced directly through the skin without a sheath. One disadvantage of our method is that when the final desired stent diameter is known to be greater than 10 mm, redilation of the stent is required after initial placement. In some such patients, a modification of the new method of stent placement in which the appropriate-size balloon is used as the dilator for a larger sheath may be preferable. Given the limited amount of data available in regard to stress fatigue and stent integrity with overexpansion of the Palmaz stent, as well as the continued advice from the manufacturer that the stent not be expanded more than 12 mm, such overdilation should be performed with caution until more data are obtained or larger stents become available. We used the Cordis Plus 7-F sheath in patients with a Glenn anastomosis in whom the internal jugular approach was used. The Cordis Plus sheath is used with the 8-mm Olbert balloon and stent but is only 23 cm long. Because the 8mm Olbert balloon and stent will not fit through a 7-F Mullins sheath and a n 80cm-long sheath is necessary when the leg approach is used, the Cordis sheath could not be used. The preferred ap- Salazar et a1 45 Volume 7 Number 1 Table 3 Results in Patients Pressure Gradient (mm Hg) Patient No. Site 1 1 2 3 4 5 6 RPA LPA RPA LPA RPA LPA LPA Mean + SE Note.-LPA *P < .05. = left Before Stent Placement After Stent Placement Change in Gradient (mm Hg) 89 92 2 4 4 41 25 36.7 39.4 44 20 0 0 0 4 9 1l * 16.6 45 72 2 4 4 37 16 25.7 26.6 Stenosis Diameter (mm) Before Stent Placement After Stent Placement Change in Diameter (mm) Time (min) 2.3 2.4 2 3.9 3.2 4 4 3.1 0.88 7 8.9 9 8 11 12 8.2 9.2* 1.8 4.7 6.5 7 4.1 7.8 8 4.2 6.0 1.7 14 13 18 7 10 14 17 13.3 3.8 pulmonary artery, RPA = right pulmonary artery, and SE = standard error. proach for stent implantation in the pulmonary artery is from the right femoral vein to facilitate catheter manipulation and provide a more straight catheter course. This approach also avoids the need for general anesthesia in smaller children. The Olbert balloon has several unique features (low profile before and after deflation and balloon material) that make it ideal for placement of the Palmaz stent. The low-profile characteristics of the Olbert balloon allow delivery of the balloon and stent into the branch pulmonary artery with only a 7-8-F sheath. The Olbert balloon catheter is constructed of a material that allows formation of a tight bond between stent and balloon; we have found that this bond makes premature dislodgment of the stent from the balloon uncommon. Finally, unlike other angioplasty balloons that develop "wings" after deflation, the Olbert balloon retains its low profile after deflation, and inadvertent dislodgment of the expanded stent during balloon removal is virtually eliminated. Because of its coaxial design, the Olbert balloon inflates by shortening as the tip of the catheter retracts. At the time of inflation, the leading edge of the balloon (and therefore the stent) is moved 5-8 mm back toward the catheter hub. To compensate for this movement the stent should be positioned 5-6 mm above the final desired position, and the position of the stent should be corrected a t a partially inflated state (4-6 atm) (11). If the stent is crimped onto the balloon near its trailing edge, the stent will move less (1-3 mm) as the balloon in- flates, but this implies that the balloon catheter must be advanced farther past the lesion, and advancing the catheter may be difficult. We have found the use of a TouheyBorst type of adapter, Luer-locked to the sheath hub and holding firm to the shaft of the balloon catheter, to be helpful in preventing dislodgment of the stentmounted balloon catheter from the sheath before crossing the stenosis. Use of this adapter also obviates the need for a second catheter for confirmation of stent position because the adapter allows injection of contrast media through the sheath. Bjarnason et a1 (11)recently described placement of 19 Palmaz P308 stents by using the same size balloon and a similar method in 11patients with atherosclerotic lesions in the iliac arteries. They reported no complications or difficulties with the technique. In their series, the Palmaz stent was also crimped onto the balloon by means of only finger pressure, and there were no reported instances of distorted slits or asymmetric expansion. We believe that this new method of stent placement represents a useful alternative for endovascular stent implantation in smaller patients. The use of a smaller sheath and a single-unit delivery system allows adequate stent positioning and redilation to up to 12 mm in diameter when indicated. This technique also may prove advantageous when a difficult catheter course is anticipated because it allows simultaneous passage of sheath, balloon, and stent across the stenotic lesion. In our experience, this new method of stent placement decreases the time re- quired for the procedure and improves the ease and success rate of stent placement in stenoses of the branch pulmonary artery. It has become our method of choice, especially in young children. Acknowledgments: We are grateful to J u a n Salazar, MD, and Kurt Amplatz, MD, for their technical assistance. References 1. Mullins CE, O'Laughlin MP, Vick GW 111, et al. Implantation of balloon expandable intravascular grafts by catheterization in pulmonary arteries and systemic veins. Circulation 1988; 77: 188-199. 2. O'Laughlin MP, Perry SB, Lock JE, Mullins CE. Use of endovascular stents in congenital heart disease. Circulation 1990; 83:1923-1939. 3. Rocchini AP, Meliones JN, Beekman RH, Moorehead C, London M. Use of balloon-expandable stents to treat experimental peripheral pulmonary artery and superior vena caval stenosis: preliminary experience. Pediatr Cardiol 1992; 13:92-96. 4. Lock JE, Keane JF, Fellows KE. Diagnostic and interventional catheterization in congenital heart disease. Boston, Mass: Martinus Nijhoff, 1986; 72-95. 5. O'Laughlin MP, Slack MC, Grifka RG, P e n y SB, Lock JE, Mullins CE. Implantation and intermediate-term follow-up of stents in congenital heart disease. Circulation 1993; 88:605-614. 6. Trerotola SO, Lund GB, Newman J, et al. Repeat dilation of Palmaz stents in pulmonary arteries: study of safety and effectiveness in a growing animal model. JVIR 1994; 5425-492. 7. Animal Care and Experimentation Committee. Source book for the use of 46 Journal of Vascular and Interventional Radiology January-February 1996 animals in physiological research and teaching. Bethesda, Md: The American Physiological Society, 1993. 8. Palmaz JC, Sibbitt RR, Tio FO, Reuter SR, Peters JE, Garcia F. Expandable intraluminal vascular graft: a feasibility study. Surgery 1986; 99:199-205. 9. Levine MJ, Leonard BM, Burke JA, et al. Clinical and angiographic results of balloon expandable intracoronary stents in right coronary artery stenoses. J Am Coll Cardiol 1990; 2:332-339. 10. Charnsangavej CH, Carrasco H, Wallace S, et al. Stenosis of the vena cava: preliminary assessment of treatment with expandable metallic stents. Radiology 1986; 161:295-298. 11. Bjarnason H, Hunter DW, Ferral H, et al. Placement of the Palmaz stent with the use of a n 8-F introducer sheath and Olbert balloons. JVIR 1993; 4435-439.