Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
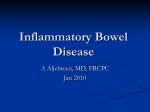
PandMM-CPD August 2010 PJ Online_Layout 1 8/19/2010 2:42 PM Page 1 PJ Online 1 Prescribing & medicines management Mesalazine: is changing to the cheapest really cost-effective? With over a dozen mesalazine products available for ulcerative colitis, choosing between them can be difficult. Anja St.Clair Jones discusses some of the factors that prescribers should consider. Choice should not be based on cost alone, she says, but should take into account current management strategies and adherence .pdf d.pdf Mesalazine is well established as the mainstay of treatment to manage mild to moderate ulcerative colitis (see “Ulcerative colitis: background information” Panel, p2). Most clinicians are familiar with its use but may feel unsure about the different products, their efficacy and their place in therapy. The aim of treatment is: • • • • • Symptom relief Induction and maintenance of remission Mucosal healing Avoiding surgery Reducing the likelihood of cancer A number of reviews have considered the impact of different mesalazine products and a recent one of modified release formulations advocated the substitution of generic versions as a pragmatic, cost-saving approach for the NHS.3 This review, which excluded some preparations owing to their different release mechanisms, suggested that Mesren 400mg tablets be prescribed instead of the market leader Asacol MR for all new patients and those who require a change to their drug regimen. I believe, however, that this proposed approach might only result in short-term savings. Once current strategies in management of ulcerative colitis and adherence issues are taken into account it is possible that change to the cheaper preparation could result in decreased maintenance of remission, more hospital admissions and, perhaps, an increased incidence of colorectal cancer. Recent trials have looked at high-dose or once-daily treatment regimens, or both. The non-inferiority of once-daily regimens together with mounting evidence of the negative impact of non-adherence is changing the way management of ulcerative colitis is approached. There is also a trend in practice towards the use of higher doses. According to the British Society of Gastroenterology, 4g/day of mesalazine is more effective than placebo for inducing remission in mild to moderate ulcerative colitis, and greater clinical improvement (but not necessarily remission) is associated with doses greater than 3g/day. The Ascend II trial, comparing 1,600mg tds with 800mg of Asacol tds for six weeks, indicated that patients with moderate ulcerative colitis did better on the higher dose, with a 72 per cent response compared with 59 per cent (P=0.036).4 Currently, however, for many preparations, the British National Formulary lists the dose for acute attacks as 2.4g/day. And for most preparations, it says that doses for both acute attacks and remission should be divided. The European Crohn’s and Colitis Organisation (ECCO) recommends a minimum daily dose of 1g to maintain remission but evidence is emerging that daily doses of 2g and above may be more effective.5 Non-adherence Non-adherence is generally regarded as taking less than 80 per cent of prescribed medicine. Adherence is a particular issue in patients in remission (in an acute attack patients are more likely to comply with treatment). For example, Kane et al found that overall adherence was around 40 per cent in patients using mesalazine for maintenance of quiescent ulcerative colitis.6 Similar results were shown in the Manitoba inflammatory bowel diseases cohort study, in which about a third of patients were found to be low adherers.7 The clinical impact of non-adherence is considerable. It increases the chance of relapse to 61 per cent in non-adherers compared with 11 per cent in adherers (P=0.001),8 reduces quality of life, and increases colorectal cancer risk to 31 per cent in non-adherers in comparison with 3 per cent in adherers (P=<0.001).9 A review by Hawthorne confirms that adherence to mesalazine therapy reduces the risk of colorectal cancer by 75 per cent and favours a multidisciplinary team approach to improve adherence rates.10 In 2004, the economic cost for caring for patients with inflammatory bowel diseases over six months in the UK ranged from £73 to £33,254, with the mean cost for ulcerative colitis patients being£1,256. Only 14 per cent of patients in the study needed admission to hospital but they accounted for 49 per cent of total secondary care cost.11 Strategies to achieve adherence In a systematic review Kane also found varied factors and reasons for non-adherence, including disease duration, male gender, single status, full-time employment and three times a day dosing.12 Patients gave forgetfulness, questioning the need for medication, inconvenient regimens and having to take many tablets as reasons for non-adherence. In 2009, the National Institute for Health and Clinical Excellence clinical guideline CG76, “Medicines adherence: involving patients in decisions about prescribed medicines and supporting adherence”, recommended simplifying drug regimens in order to tailor therapies to the needs of individual patients, integrating regimens into their lives. Addressing barriers to adherence resulting from patients’ beliefs is complex and proposed interventions are probably of limited benefit, but offering simpler, less intrusive drug delivery methods are of proven value. Patients tend to prefer once daily oral formulations. With the trend of treatment to higher dose regimens tablet burden needs to be reduced to improve compliance. Higher dose preparations, such as Asacol 800mg tablets and Pentasa 2g sachets, have been formulated for the treatment of active disease. Rectal preparations ECCO guidelines advise adding topical (rectal) mesalazine to oral because oral mesalazine alone is less effective in improving symptoms. However, rectal preparations tend to be less acceptable than oral preparations and are associated with leakage, retention issues and bloating, and can reduce adherence to therapy. Therefore they tend to be used in the treatment of active distal disease or in combination with oral formulations for extensive disease. A review of rectal preparations is outside the scope of this article but it should be noted that, as with oral preparations, different rectal formulations deliver mesalazine to different parts of the distal colon, in different concentrations and with variable acceptability to patients. Further considerations Because the action of mesalazine is predominantly topical, the aim is to deliver active drug to the site of inflammation, with minimal systemic absorption. Only 15 per cent of patients initially presenting with August 2010 www.pjonline.com PandMM-CPD August 2010 PJ Online_Layout 1 8/19/2010 2:42 PM Page 2 2 PJ Online Learning & development ULCERATIVE COLITIS: BACKGROUND INFORMATION Ulcerative colitis is a life-long disease arising from interaction between genetic and environmental factors observed predominantly in developed countries. The condition is characterised by diffuse mucosal inflammation which can be divided into distal (proctitis and proctosigmoiditis) or more extensive disease (left sided colitis, extensive colitis and pancolitis). The Montreal classification is favoured by the European Crohn’s and Colitis Organisation (ECCO) to describe the disease extent, as follows: • Proctitis (E1) Limited to the rectum (ie, extent of inflammation is distal to the rectosigmoid junction) • Left-sided (E2) Limited to the proportion of the colon distal to the splenic flexure (analogous to “distal” colitis) • Extensive (E3) Extends proximal to the splenic flexure (includes pancolitis) About the disease In the UK, about one in 1,000 people develop ulcerative colitis, most commonly between the ages of 10 and 40 years. Symptoms and diagnosis Symptoms include: • Mild to severe diarrhoea (which can be watery and contain mucus or blood) or urgency to get to the toilet but with nothing to pass • Cramps in the abdomen • Pain on passing stools • Feeling generally unwell (especially if an attack affects a large portion of the large intestine or is prolonged) Diagnosis usually involves a sigmoidoscopy or colonoscopy to look at the appearance of the lining of the rectum and colon. The mucosa appears inflamed and ulcered. Disease activity Management is dictated not only by disease distribution but by disease activity, which ECCO has classified into four groups: remission, mild, moderate and severe. However, ECCO did not agree criteria to assess these and the Truelove and Witts classification still seems to be a favoured approach. This classes the disease as mild, moderate or severe using the following factors: • Number of bloody stools per day (<4 mild; 4–6 moderate; ≥6 severe) • Pulse (<90bpm mild; ≤90bpm moderate; >90bpm severe) • Temperature (<37.5C mild; ≤37.8C moderate; >37.8C severe) • Haemoglobin (>11.5g/dL mild; ≥10.5g/dL moderate; <10.5g/dLsevere) • Erythrocyte sedimentation rate (<20mm/h mild; ≤30mm/h moderate; >30mm/h severe) or C-reactive protein (<5mg/L mild; ≤30mg/L moderate; >30mg/L severe) August 2010 www.pjonline.com mesalazine is tolerated by 80 per cent of those unable to tolerate sulfsalazine. Balsalazide and olsalazine are Descending Ascending colon alternatives but are not colon always well tolerated and are used in low Caecum Rectosigmoid volumes in the UK. junction Patients taking Sigmoid colon aminosalicylates should Appendix be advised to report any Rectum unexplained bleeding, bruising, sore throat or Proximal (right) side Distal (left) side malaise. Sebastian Kaulitzki | Dreamstime.com Mesalazine is the first-line therapy for induction and maintenance of remission in mild It should be noted that a review in 2007 of to moderate disease. It is safe in long-term use. activity indices (and clinical trial endpoints) The drug has a topical action on epithelial cells concluded that “an optimal scoring instrument and is, therefore, more active in ulcerative colitis for ulcerative colitis is still to be developed and (a mucosal disease) than in Crohn’s disease (a will require validation before extensive use in transmural disease). Oral mesalazine is clinical trials can be promoted”.1 completely absorbed in the small intestine but Ulcerative colitis is a relapsing condition, poorly absorbed in the colon. with acute attacks and periods of remission. To obtain a high concentration of the drug at More than 50 per cent of patients with a flare up the site of inflammation it is essential to have a relapse within a year. The relapse rate for minimise systemic exposure and insure topical patients in remission and not taking any delivery to the affected tissue.2 As for choice of medicine is 38–76 per cent. mesalazine, this cannot be made on grounds of efficacy alone — route of delivery, disease Treatment options pattern, dose frequency, patient acceptability, Treatment goals are to control symptoms and cost and availability are also relevant factors maintain remission. Drugs used include (see main article). aminosalicylates, immunosuppressants, steroids and laxatives (proctitis sufferers resist the urge of a bowel movement because it is Prognosis and lifestyle painful and constipation results) but, with so In most cases ulcerative colitis starts in the many types of ulcerative colitis described rectum (proctitis). In some patients the disease (eg, mild, active, quiescent, left-sided) choice spreads up to affect some, or all, of the colon. can be confused. Rectal preparations are People who have had ulcerative colitis for a usually used during attacks and for proctitis number of years are at a higher risk of (acute and remission). More detailed developing colorectal cancer, especially those recommendations for different types of who have frequent flare-ups affecting the whole ulcerative colitis from ECCO are available at of the large intestine. www.ecco-ibd.eu. In general, however, for mild People with ulcerative colitis do not usually to moderate disease, mesalazine is prescribed need any special diet but a high-fibre diet may initially. If two episodes of steroids are needed help those with proctitis to avoid constipation. within a year, therapy will be stepped up to Iron tablets will be needed in those who develop thiopurines, before an anti-tumour necrosis anaemia (due to blood lost in stools). factor drug. Patients taking steroids, especially those Steroids are only used to induce remission. needing more than two courses per year, In the UK, a recommended steroid regimen is should take calcium and vitamin D. prednisolone 40mg daily for one week, 30mg daily for one week, then 20mg daily for two Resources weeks followed by a review and further step • British Society of Gastroenterology guidelines down, depending on response, until the for the management of inflammatory bowel prednisolone is stopped. A severe attack can be disease in adults are available at life-threatening and must be referred to a www.bsg.org.uk/pdf_word_docs/ibd.pdf. hospital for intravenous steroid therapy. • Standards for NHS services for inflammatory About a quarter of people with ulcerative bowel disease are available at colitis will need surgery. /www.ibdstandards.org.uk. Hepatic flexure Tranverse colon First-line therapy The original treatment was sulfasalazine but side effects, including exfoliating dermatitis, are common. Choice of aminosalicylate is influenced by tolerability and Splenic flexure Signposting • Information and support for people with ulcerative colitis is available from Crohn’s and Colitis UK (www.nacc.org.uk). PandMM-CPD August 2010 PJ Online_Layout 1 8/19/2010 2:42 PM Page 3 PJ Online 3 Prescribing & medicines management PANEL 1: FORMULATION AND RELEASE CHARACTERISTICS OF ORAL MESALAZINE MR * Drug Formulation Optimal drug release pH Site of drug release Asacol MR pH dependent delayed release (>7) Ipocol Mesren MR Mezavant XL 400mg: Enteric coated with Eudragit S; 800mg: Enteric coated with layer of Eudragit S followed by Eudragit S+L Enteric coated with Eudragit S Enteric coated with Eudragit S Film coated with methacrylate copolymers type A, type B Pentasa Ethylcellulose coated microgranules Terminal ileum and large bowel (colon and rectum) Terminal ileum and colon Terminal ileum and colon Colon Colon Duodenum to rectum Salofalk Tablets: Enteric coated with Eudragit L; Granules: Eudragit L plus matrix granule structure >7 >7 Gastroresistant coating with lipophylic and hydrophilic matrix(7) Diffusion through semi-permeable membrane (enteral pH) pH dependent delayed release (>6) Terminal ileum and colon (granules have extra delayed release) *Adapted from UK Medicines Information Q&A 67.2. What are the differences between different brands of mesalazine tablets? PANEL 2: RECENT MESALAZINE TRIALS OF MAINTENANCE OF REMISSION IN MILD TO MODERATE ULCERATIVE COLITIS Sandborne et al 200916 Once a day dosing of Asacol 400mg tablets was compared with twice a day dosing to achieve doses between 1.6g and 2.4g/day for 12 months (n=1,023). Using the simple clinical colitis activity index (SCCAI), maintenance of remission was 85 per cent in both groups. In other words, non-inferiority was found. The study was not powered to prove superiority and 70 per cent of patients were already taking 2.4g/d at the start of the trial. Dignass et al 200917 A dose of 1g twice a day of pentasa granules was compared with 2g daily in 362 patients for 12 months. The ulcerative colitis disease activity index (UCDAI) was used for assessment. At one year, it was found that maintenance of remission in the twice-a-day group was 59 per cent compared with 71 per cent in the once-daily group (P=0.024). However, the trial population was small. Kruise et al 2008 18 Three regimens of Salofalk granules were compared: 3.0g daily, 1.5g daily and 0.5g three times a day, for 12 months (n=647). At one year, maintenance of remission was 75 per cent, 61 per cent and 69 per cent, respectively, suggesting that 3g daily is the more efficacious dosage. However, this research is accessible in abstract form only so in depth analysis of data is not possible. Assessment indices used were clinical activity index (CAI) and endoscopy index (EI). Kamm et al 20084 A regimen of Mezavant tablets 2.4g daily was compared with 1.2g twice a day for 12 months (n=459). Maintenance of remission in the once-daily regimen was 64 per cent compared with 68 per cent in the twice-daily regimen (P=0.351). The UCDAI was used for assessment. ulcerative colitis have disease extending beyond the splenic flexure (ie, extensive, E3). Most have distal disease. However, use of formulations, such as pH dependent release preparations (eg, Asacol, Ipacol, Mesren, Salofalk tablets), that release the drug as a bolus in the proximal colon, and azo-bonded preparations (eg, olsalazine, and sulfasalazine) may mean insufficient concentrations are achieved in the distal part of the colon. Formulations such as MMX Multi Matrix (eg, Mezavant) and pH independent delayed release system (eg, Pentasa and Salofalk granules), which release the drug all the way through the colon might address such problems and, therefore, be better for most patients, but this needs further investigation, taking into account limitations of techniques assessing intra-luminal concentrations. A review of methods of assessing active drug release, intra-luminal concentration and colonic distribution concluded that although assessing drug release was important, due to the limitations of the individual techniques, randomised clinical trials remain the best guide for dosing and treatment regimen decisions.13 Panel 1 gives a summary of formulations of modified release oral mesalazine products and their characteristics. Both Mesren and Ipocol are generics of Asacol and studies indicate that the in vitro dissolution profile of Mesren MR seems to be nearly identical to that of Asacol MR 400mg while the Ipocol dissolution profile seems to be slightly different.3,13,14 However, a study comparing Ipocol with Asacol MR 400mg in 88 patients with mild to moderate relapse of ulcerative colitis found both preparations to be equally effective.1 Mesren has not been clinically compared with other preparations (it is not a requirement for licensing because the product has the same bioequivalence as Asacol MR). It is also worth noting that Asacol formulations in different countries are not equivalent due to different manufacturing processes and coating so, for example, US trial data might not be valid for comparison with UK data. Recent evidence Despite individual trial results, systematic reviews fail to find conclusive dose-dependent responses to mesalazine therapies, partly due to study designs and partly due to the fact that attainment of remission is affected by disease severity, duration and interpatient variability. This might reflect the inability of current formulations to deliver consistently therapeutic drug levels to affected tissue — gut function, distribution of gut content and effect of the drug on gut flora is still poorly understood and these factors may all affect efficacy. A Cochrane review in 2009 concluded that the differences in efficacy are likely to be marginal and further trials should look at enhancing patient adherence with medication rather than comparing the efficacy of various mesalazine agents.15 Recent studies on maintenance of remission in quiescent disease are outlined in Panel 2. Remission rates between studies cannot be compared due to difficulties in interpretation and differences of study design. Furthermore, unlike Crohn’s disease, the lack Anja St.Clair Jones will be available to answer questions online on the topic of this article until 6 September 2010 Ask the expert www.pjonline.com August 2010 www.pjonline.com PandMM-CPD August 2010 PJ Online_Layout 1 8/19/2010 2:42 PM Page 4 4 PJ Online Learning & development of standard indices for ulcerative colitis (see “Ulcerative colitis” Panel) precludes the collection of consistent treatment efficacy data. It should be noted that most of the assessment indices used in these recent studies are unvalidated (with the exception of clinical activity index, which was validated in one study) or not formally validated (ulcerated colitis activity index). Moreover, because assessment indices are inconsistent, as was the selection of patient groups and subgroups, comparisons across these studies are difficult. Recent research is mainly concerned with increased dose range and formulations that reduce the pill burden on patients. Adherence is increasingly included as secondary endpoints in the maintenance of quiescent ulcerative colitis studies underlining the increasing importance of this factor on maintenance of remission. The need to develop standard assessment indices for ulcerative colitis is paramount to evaluate the efficacy of different formulations because only trial data can accurately determine the effect of formulation on response. Intraluminal concentration assessment methods remain limited in their usefulness. Costs Panel 3 compares pill burden, dosage and cost of recommended regimens. Asacol 800mg tablets are large and may not be acceptable to all patients. Pentasa may be a preferable option for maintenance of remission in view of cost and adherence issues as discussed — one 2g sachet once daily compares favourably to Mesren and Asacol MR, in terms of reduced unit load burden. Salofalk has limited data but those reported so far seem to favour higher doses of 3g. Currently, it is a patient-centred approach to management that will result in long-term cost-effectiveness. Conclusion Adherence to mesalazine treatment in is complex and multifactorial, and differs with time.18 Studies of several formulations of once daily dosing in induction and in maintenance therapy have shown that oncedaily dosing is efficacious and safe, that formulations are probably not of significant importance to the effect of mesalazine but that high strength and once-daily dosing may improve adherence. Research has shown that divergence of adherence at month three (when maintenance treatment begins)16,19 affects the maintenance of remission so it is imperative to reduce pill burden. It is questionable if generic low-dose tablets offer a patient-centred reliable alternative — like Asacol MR, they are not licensed to be used once a day. It remains to be investigated if a change to once-daily dosing and low tablet loads reduces hospital admissions and long-term incidence of colorectal cancer. Anecdotal reports exist but this must be a priority area of research in the future. August 2010 www.pjonline.com PANEL 3: DOSE AND COST COMPARISON OF ORAL MESALAZINE Asacol MR Active disease (higher dose) Unit load/day Dose Cost* 6x800mg tabs ii tds (4.8g/d) £224 Mezavant XL 4x1.2g tabs Mesren MR 12x400mg tabs iv tds‡ (4.8g/d) £140 Pentasa granules 2x2g sachets Salofalk granules 2x1.5g sachets ii od (3g/d) iv od (4.8g/d) £233 i bd (4g/d) Maintenance of remission Unit load/day Dose Cost† 3x800mg tabs i tds (2.4g/d) £730 2x1.2g tabs ii od (2.4g/d) £759 6x400mg tabs ii tds (2.4g/d) £475 £135 1x2g sachets i od (2g/d) £92 2x1g sachets ii od (2g/d)‡ £428 £438 * Eight weeks BNF 59 March 2010; †12 months BNF 59 March 2010; ‡ unlicensed DECLARATION OF INTEREST The author has provided training support work to Ferring in the past. References 1 D’Haens G, Sandborn WJ, Feagan BG, Geboes K, Hanauer SB, Irvine EJ et al. A review of activity indices and efficacy end points for clinical trials of medical therapy in adults with ulcerative colitis. Gastroenterology 2007;132:763–86. 2 Travis SPL. Therapy update: which 5-ASA? Gut 2002;51:548–9. 3 Grosso A, Bodalia P, Shah M. A review of mesalazine MR formulations in ulcerative colitis. The British Journal of Clinical Pharmacy 2009;1:333–6. 4 Kamm MA, Lichtenstein GR, Sandborn WJ, Schreiber S, Lees K, Barrett K et al. Randomised trial of once- or twice daily MMX mesalazine for the maintenance of remission in ulcerative colitis. Gut 2008;57:893–902. 5 European Crohn’s and Colitis Organisation Ulcerative Colitis Guidelines: current management. Available at www.ecco-ibd.eu (accessed on 11 august 2010). 6 Kane SV, Cohen RD, Aikens JE, Hanauer SB.. Prevalence of non adherence with maintenance mesalamine in quiescent ulcerative colitis. American Journal of Gastroenterology 2001;96:2929–33. 7 Ediger J, Walker JR, Graff L, Lix L, Clara I, Rawsthorne P et al. Predictors of medication adherence in inflammatory bowel disease. American Journal of Gastroenterology 2007;102:1417–26. 8 Kane SV. Systematic review: Adherence issues in the treatment of ulcerative colitis. Alimentary Pharmacology & Therapeutics 2006;23:577-587:1207–14. 9 Kane SV, Huo D, Aikens J, Hanauer S. Medication nonadherence and the outcomes of patient with quiescent ulcerative colitis. American Journal of Medicine 2003;114:39–43. 10 Hawthorne A, Rubin G, Ghosh S. Medication non-adherence in ulcerative colitis — strategies to improve adherence with mesalazine and other maintenance therapies. Alimentary Pharmacology & Therapeutics 2008;27:1157–66. 11 Bassi A, Dodd S, Williamson P, Bodger K. Cost of illness of inflammatory bowel disease in the UK: a single centre retrospective study. Gut 2004;53:1471–8. 12 Lichtenstein GR, Kamm MA. Review article: 5aminosalicylate formulations for the treatment of ulcerative colitis – methods of comparing release rates and delivery of 5-aminosalicylate to the colonic mucosa. Alimentary Pharmacology & Therapeutics 2008;28:663–73. 13 Enteric coated mesalazine: Ipocol and Asacol. Trent Medicines Information Service, 2003. Available at www.ukmicentral.nhs.uk (accessed on 10 August 2010). 14 Mesren: Clinical information. Ivax Pharmaceuticals, January 2005 15 Sutherland LR, MacDonald JK. Oral 5aminosalicylic acid for maintenance of remission in ulcerative colitis (Review) 2009. Available at http://onlinelibrary.wiley.com (accessed on 16 August 2010). 16 Dignass AU, Bokemeyer B, Adamek H, Mross M, Vinter-Jensen L, Börner N et al. Mesalamine once daily is more effective than twice daily in patients with quiescent ulcerative colitis. Clinical Gastroenterolgy and Hepatology 2009;7:762–9. 17 Kruis W, Jonaitis L, Pokromieks J, Acute G, Mikhailova TL et al. Once daily 3g mesalamine is the optimal dose for maintaining clinical remission in ulcerative colitis: a double blind, double-dummy, randomized, controlled, dose-ranging study. Gastroenterology 2008:134:A489. Abstract. 18 Kane S, Accortt NA, Magowan S, Brixner D. Predictors of persistence with 5aminosalicylic acid therapy ulcerative colitis. Alimentary Pharmacology & Therapeutics 2009;29:855–62. This article has not been peer-reviewed. The author Anja St.Clair Jones, MRPharmS, is lead pharmacist, surgery and digestive diseases, at Brighton and Sussex University Hospitals NHS Trust