Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
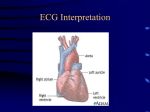
Electrophysiology of the Heart ECG Monitoring • The ECG is a graphic representation of the heart's electrical activity generated by depolarization and repolarization of the atria and ventricles ECG Monitoring • Valuable diagnostic tool for identifying cardiac abnormalities including: – – – – Abnormal heart rates and rhythms Abnormal conduction pathways Hypertrophy or atrophy of portions of the heart Approximate location of ischemic or infarcted cardiac muscle ECG Monitoring • The ECG tracing is only a reflection of the heart's electrical activity • It does not provide information regarding mechanical events such as force of contraction or blood pressure Voltage • Voltage may be: – Positive--seen as an upward deflection on the ECG tracing – Negative--seen as a downward deflection on the ECG tracing – Isoelectric--no electrical current detected • Seen as a straight baseline on the ECG Application of Monitoring Electrodes • Electrodes are pre-gelled, stick-on disks that can easily be applied to the chest wall • When applying electrodes: – Cleanse the area with alcohol to remove dirt and body oil – Use the inner surfaces of the arms and legs when attaching electrodes to extremities Application of Monitoring Electrodes • When applying electrodes: – Trim excess body hair (if necessary) before placing the electrodes – Attach the electrodes to the prepared site – Attach the ECG cables to electrodes – Turn on the ECG monitor and obtain a baseline tracing Monitoring Electrodes • If the signal is poor, recheck the cable connections and electrode contact with the patient's skin • Other causes of a poor signal include: – – – – Excessive body hair Dried conductive gel Poor electrode placement Diaphoresis ECG Monitoring ECG Monitoring ECG Monitoring Calibration • The sensitivity of the 12-lead ECG machine is standardized • When properly calibrated, a 1-mV electrical signal produces a 10-mm deflection (two large squares) on the ECG tracing Figure 28-21 The Electrocardiogram The Electrocardiogram The Electrocardiogram The Electrocardiogram The Electrocardiogram The Electrocardiogram The Electrocardiogram The Electrocardiogram – Refractory Periods • Absolute – no other electrical impulse can be generated • Relative – very dangerous time another electrical impulse can interfere with the rhythm – V Tach can occur or V Fib Conduction System of the Heart • Sinoatrial (SA) node • Atrioventricular (AV) node / bundle of His • Purkinje fibers Figure 6-41 Normal Conduction • Sequence of normal impulse conduction – SA node – Both atria • Atrial contraction – – – – AV node Bundle of His Purkinje fibers Both ventricles • Ventricular contraction Figure 6-41 Inherent Rates • SA node – 60-100 • AV node – 40-60 • Ventricular – 20-40 P Wave • First positive (upward) deflection on ECG • Represents atrial depolarization • Usually rounded and precedes the QRS complex – Begins with first positive deflection from baseline – Ends at point where wave returns to baseline Figure 28-22 P Wave • Duration normally 0.10 second or less • Amplitude normally 0.5 to 2.5 mm • Usually followed by a QRS complex unless conduction disturbances are present Figure 28-22 PR Interval • Represents the time it takes for an electrical impulse to be conducted through the atria and the AV node up to the instant of ventricular depolarization – Measured from the beginning of the P wave to the beginning of the next deflection on the baseline (the onset of the QRS complex) • Normal is 0.12-0.20 second Figure 28-25 PR Interval • A normal PR interval indicates that the electrical impulse has been conducted through the atria, AV node, and bundle of His normally and without delay • PRI < 0.2 secs Figure 28-25 QRS Complex • Generally composed of three individual waves: the Q, R, and S waves • Begins at the point where the first wave of the complex deviates from the baseline • Ends where the last wave of the complex begins to flatten at, above, or below the baseline Figure 28-25 QRS Complex • Direction of the QRS complex may be: – Predominantly positive (upright) – Predominantly negative (inverted) – Biphasic (partly positive, partly negative) QRS Complex • The normal QRS complex is narrow and sharply pointed • Duration is generally 0.08 to 0.12 second • Amplitude normally varies from less than 5 mm to more than 15 mm Figure 28-25 Q Wave • The first negative (downward) deflection of the QRS complex on the ECG – May not be present in all leads • Represents depolarization of the interventricular septum Figure 28-25 R Wave • First positive deflection after the P wave – Subsequent positive deflections in the QRS complex that extend above the baseline and that are taller than the first R wave are called R prime (R’), R double prime (R’’), and so on Figure 28-23 S Wave • Negative deflection that follows the R wave – Subsequent negative deflections are called S prime (S’), S double prime (S”), and so on • R and S waves represent the sum of electrical forces resulting from depolarization of the right and left ventricles Figure 28-25 QRS Complex • Follows the P wave • Marks the approximate beginning of mechanical systole of the ventricles, which continues through the onset of the T wave • Represents ventricular depolarization – Conduction of an electrical impulse from the AV node through the bundle of His, Purkinje fibers, and the right and left bundle branches QRS Complex Figure 28-22 ST Segment • Represents the early phase of repolarization of the right and left ventricles • Immediately follows the QRS complex and ends with the onset of the T wave Figure 28-24 A ST Segment • The point at which the ST segment “takes off” from the QRS complex is called the J point Figure 28-24 D ST Segment • The position of the ST segment is commonly judged as normal or abnormal using the baseline of the PR or TP interval as a reference – ST segment elevation – ST segment depression Figure 28-24 A, B, & C ST Segment • Abnormal ST segments may be seen in: – – – – – Infarction Ischemia Pericarditis After digitalis administration Other disease states T Wave • Represents repolarization of ventricular myocardial cells • Occurs during the last part of ventricular systole • May be above or below the isoelectric line and is usually slightly rounded and slightly asymmetrical Figure 28-25 T Wave • Deep and symmetrically inverted T waves may suggest cardiac ischemia • A T wave elevated more than half the height of the QRS complex (peaked T wave) may indicate a new onset of myocardial ischemia or hyperkalemia Artifact • A series of deflections on the ECG display or tracing produced by factors other than the heart's electrical activity • Common causes of artifact: – – – – – Improper grounding of the ECG machine Patient movement Loss of electrode contact with the patient's skin Patient shivering or tremors External chest compressions Artifact - Muscle Tremors Figure 28-26 A Artifact - AC (60 cycle) Interference Figure 28-26 B Artifact – Loose Electrode Figure 28-26 C Reading ECG’s ECG Measurements 1 sec 0.20 sec 0.04 sec 5 large squares= 25 mm = 1 second 1 large square = 5 mm = 5 small squares =0.20 seconds 1 small square = 1 mm = 0.04seconds 0.1 mV Voltage Standard calibration for an ecg is 10mm=1 mV, or 1mm = 0.1mV Time Rate Determination The Six Second Method 1. ECG paper is marked at three second intervals (15 large boxes) 2. Count the R Waves in 6 seconds (30 large boxes/two 3-second intervals) 3. Multiply the number of complexes by 10 to determine the rate (in this example 7 X 10 = 70) 1 2 3 4 5 6 7 Interpreting ECG’s • Questions to ask – – – – – – – – Are there P waves? Do they all look alike? PRI – short or long? QRS – tight or wide? Any extra P waves? Any extra QRS complexes? What is the rate? WHAT IS THE UNDERLYING RHYTHM? Atrial Rhythms • Sinus rhythm – – – – P waves PRI – normal No extra beats Rate 60 - 100 • Sinus Bradycardia – – – – P waves PRI – normal No extra beats Rate is < 60 • Sinus Tachycardia – – – – P waves PRI – normal No extra beats Rate is 100-150 • Wandering Atrial Pacemaker – P waves are present but they do not look alike – QRS intervals are regular • Wolfe-Parkinson-White – P waves are present – Delta wave – Reentry rhythm • Sinus Rhythm with unifocal Premature Ventricular Contractions (PVC) – – – – – P waves are present PRI is normal Some QRS complexes come early and are wide Premature QRS complexes look alike Must differentiate whether the PVC’s look alike or not • Sinus Rhythm with multifocal PVC’s – – – – – P waves are present PRI is normal Some QRS complexes come early and are wide Early QRS complexes are different Must differentiate whether the PVC’s look alike or not • Sinus Rhythm with couplets – P waves are present – PRI is normal – 2 QRS complexes come early together and are wide • Sinus Rhythm with a run of V Tach – P waves are present – PRI is normal – 3 or more PVC’s together • Sinus Rhythm with R on T phenomenon – P waves are present – PRI is normal – Can go into V Fib • Sinus Rhythm with bigeminy – Underlying rhythm is a SR – Every other QRS complex is a PVC • Sinus Rhythm with an aberrant conduction or Bundle Branch Block – P waves are present – PRI is normal – QRS complex is wide • Atrial fibrillation – No discernable P waves – QRS – irregularly irregular • Atrial Flutter – P waves are flutter waves or “sawtooth pattern” – QRS can be regular or irregular Heart Blocks • Sinus Rhythm with 1st degree HB – – – – P waves are present PRI – longer than normal QRS complex is usually narrow MUST GIVE AN UNDERLYING RHYTHM • 2nd degree HB Type I or Wenckebach – P waves are present – Extra P waves – PRI gets progressively longer then you get a “dropped QRS” • 2nd degree HB Type II or Classic 2nd degree HB – P waves are present – Extra P waves – PRI stays the same but then you get a “dropped QRS” • 3rd degree HB or Complete HB – – – – – – – P waves are present P waves map out QRS complexes are usually wide QRS complexes map out P waves do not map out with the QRS complexes PRI has no consistency Sometimes it looks like the P waves are marching towards the QRS Junctional Rhythms • Junctional Rhythm – No P waves – QRS complex is tight – Rate 40-60 • Junctional Bradycardia – No P waves – QRS complex is tight – Rate < 40 • Accelerated Junctional Rhythm – No P waves – QRS complex is tight – Rate 60-100 • Junctional Tachycardia – No P waves – QRS complex is tight – Rate 100-150 Ventricular Rhythms • Idioventricular Rhythm – – – – No P waves QRS complex is wide Rhythm is regular Rate 20-40 • Agonal Idioventricular Rhythm – – – – No P waves QRS complex is extremely wide Will not produce a pulse Rate < 20 • Accelerated Idioventricular Rhythm – – – – No P waves QRS complex is wide Rhythm is regular Rate 40-100 • “Slow” Ventricular Tachycardia – – – – No P waves QRS complex is wide Rhythm is regular Rate 100-150 • Ventricular Tachycardia – – – – No P waves QRS complex is wide Rhythm is regular Rate > 150 • Ventricular Fibrillation – – – – No P waves QRS complex is wide and bizarre Rhythm is erratic Rate > 150 • Fine Ventricular Fibrillation – – – – No P waves QRS complex is wide, bizarre and small Rhythm is erratic Rate > 150 • Coarse Ventricular Fibrillation – – – – No P waves QRS complex is wide, bizarre and large Rhythm is erratic Rate > 150 • Torsades de Pointes (Turning of the Points) – – – – – No P waves QRS complex is wide, bizarre and large QRS complexes seem to face different directions Rhythm is erratic Rate > 150 • Asystole – – – – No P waves No QRS complexes “Flatline” Must confirm in at least two leads • Ventricular Pacemaker – P waves may or may not be present – Pacemaker spikes just prior to QRS complex – QRS complexes are wide • Atrial Pacemaker – Pacemaker spikes just prior to P waves – QRS complexes are narrow • Atrial Ventricular Pacemaker or AV Sequential Pacemaker – Pacemaker spikes just prior to P wave – Pacemaker spikes just prior to QRS complex – QRS complexes are wide Any Questions???