Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Electrocardiography wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Echocardiography wikipedia , lookup
―Original―
Early Detection of Subclinical Anthracycline Cardiotoxicity
on the Basis of QT Dispersion
Yohko Uchikoba, Ryuji Fukazawa, Takashi Ohkubo,
Miho Maeda and Shunichi Ogawa
Department of Pediatrics, Graduate School of Medicine, Nippon Medical School
Abstract
Background: We examined whether dobutamine-stress QT dispersion (QTd) and heartrate corrected QT dispersion (QTcd) are useful for detecting subclinical anthracycline
cardiotoxicity.
Methods: The subjects were10 control subjects and 37 patients divided into 4 groups
according to cumulative anthracycline dose: non-anthracycline group (group N), 7 patients; low
anthracycline cumulative dose group (group L), 8 patients (<200 mg!
m2); medium anthracycline
cumulative dose group (group M), 16 patients (200 to <400 mg!
m2); and high cumulative group
(group H), 6 patients ("400 mg!
m2). Standard 12-lead electrocardiograms were recorded. QTd
and QTcd were measured and calculated at rest and after administration of dobutamine at 5
or 30 μg!
kg!
min. We also estimated cardiac function and cardiac reserve function at rest and
after administration of dobutamine at a dose of 5 or 30 μg!
kg!
min.
Results: At rest, QTd and QTcd were significantly greater in groups M and H. After
administration of dobutamine at 30 μg!
kg!
min, QTd and QTcd were significantly greater in
groups L, M, and H. There was good correlation between QTd and the cumulative
anthracycline dose; the correlation formula was y=0.051x + 42.2 (r=0.81, p<0.001). The
cumulative anthracycline dose of 152.9 mg!
m2, calculated from the correlation formula, was the
cut-off for detection of electrophysiological cardiac abnormalities. Cardiac performance data at
rest and dobutamine stress by echocardiography and pulsed Doppler echocardiography are
less sensitive for detecting cardiac abnormalities than are QTd and QTcd.
Conclusions: Dobutamine-stress QTd and QTcd are useful for detecting anthracycline
cardiotoxicity and subclinical cardiac abnormality at low cumulative anthracycline doses. We
must be aware of the possibility of subclinical myocardial abnormalities in patients with a
cumulative anthracycline dose of "150 mg!
m2 .
(J Nippon Med Sch 2010; 77: 234―243)
Key words: anthracycline cardiotoxicity, QT dispersion, heart-rate corrected QT dispersion,
dobutamine, malignancy
Correspondence to Shunichi Ogawa, MD, Department of Pediatrics, Nippon Medical School, 1―1―5 Sendagi, Bunkyoku, Tokyo 113―8603, Japan
E-mail: [email protected]
Journal Website (http:!
!
www.nms.ac.jp!
jnms!
)
234
J Nippon Med Sch 2010; 77 (5)
Anthracycline Cardiotoxicity
durations on 12-lead standard electrocardiography
(ECG), and is considered to reflect local differences in
Introduction
the repolarization of the myocardium. QT dispersion,
Anthracyclines,
doxorubicin,
are
such
as
daunorubicin
highly
effective
and
which
reflects
cardiac
autonomic
imbalance 13,
antineoplastic
increases in various cardiac diseases, such as heart
agents in the treatment of solid tumors and
failure6, cardiomyopathy7, ischemic heart disease8,
hematological malignancies and form an important
hypertension10,
long-QT
syndrome11,12,
and
after
9
component of many antineoplastic chemotherapeutic
myocardial infarction . QT dispersion is useful for
regimens. Unfortunately, because anthracycline have
determining prognosis in these diseases.
acute and chronic effects on the myocardium, their
use
is
limited
by
their
hypothesize
that
dobutamine-stress
QT
Acute
dispersion (QTd) can be
causes
ventricular spatial heterogeneity of repolarization,
electrocardiographic abnormalities, such as sinus
which is a sign of anthracycline cardiotoxicity at
tachycardia, ST depression, and arrhythmias, during
lower cumulative doses in long-term survivors after
administration or several hours to several days after
early-stage treatment for childhood malignancies.
administration.
This study presents data to test this hypothesis.
anthracycline
cardiotoxicity.
We
cardiotoxicity
However,
most
of
the
acute
used
to
detect
the
cardiotoxic effects of anthracycline are transient and
reversible 1.
In
contrast,
chronic
Patients and Methods
anthracycline
cardiotoxicity causes irreversible cardiomyopathies
and congestive heart failure that can restrict
Subjects
physical
The subjects were 37 long-term survivors of
activity.
anthracycline
The
incidence
cardiotoxicity
of
chronic
depends
on
the
childhood
malignancies
who
underwent
cumulative anthracycline dose administered. For
anthracycline therapy from 1998 through 2003 at
example, the incidence of congestive heart failure is
our hospital (17 female and 20 male; present age
0.01% to 0.27% for cumulative anthracycline doses
range, 3 years 7 months to 28 years 3 months), and
< 550 mg !m ,
cumulative
10 volunteer healthy control subjects (control group;
. Even at low
age range, 17―28 years). Of the 37 patients, 24 had
2
and
is
> 30%
for
anthracycline doses >550 mg!
m
doses,
anthracyclines
myocardial
damage
can
with
2 2,3
cause
late
subclinical
fibrosis
of
the
had acute lymphoblastic leukemia, 5 had had acute
non-lymphoblastic leukemia, 2
had
had
Ewing
specimens 4.
sarcoma, 3 had had non-Hodgkin s lymphoma, 1 had
Therefore, effective monitoring of the cardiotoxic
had neuroblastoma, 1 had had Wilms tumor, and 1
effects of anthracycline requires early assessment of
had
both cardiac function and cardiac reserve function.
cumulative anthracycline doses of the patients
This form of assessment may involve an exercise
ranged from 0 to 840 mg!
m2 (Table 1). None of the
test.
patients had symptoms of congestive heart failure.
myocardium,
We
as
seen
previously
echocardiography
in
biopsy
performed
The
to their cumulative anthracycline dose, based on our
therapy, and detected cardiac dysfunction even in
previous findings14. The groups were the non-
children
anthracycline
received
receiving
low-dose
bicycle
histiocytosis.
anthracycline
who
supine
cell
The patients were divided into 4 groups according
patients
a
Langerhans
for
asymptomatic
using
exercise-stress
had
anthracycline
(group
N,
7
patients);
the
low
therapy (175 mg!
m2)5. For patients with a low
cumulative anthracycline dose group (group L, <200
tolerance for physical exercise, such as infants and
mg!m 2 ;
small
anthracycline dose group (group M, 200―<400 mg!
children,
monitoring
of
cardiac
function
8
patients ) ;
the
middle
cumulative
requires an alternative exercise test, such as a drug-
m2;
induced exercise test.
anthracycline dose group (group H, "400 mg!
m2 ; 6
QT
dispersion
is
defined
as
the
difference
between the maximum and minimum QT interval
J Nippon Med Sch 2010; 77 (5)
16
patients);
and
the
high
cumulative
patients) (Table 1). Informed consent was obtained
for all subjects.
235
Y. Uchikoba, et al
Ta
bl
e1 Pa
t
i
e
ntc
ha
r
a
c
t
e
r
i
s
t
i
c
s
Ca
s
e
No
Gr
o
up
s
e
x
ATCc
umul
a
t
i
vedo
s
e
(
mg/
m2)
1
2
3
4
5
6
7
8
9
1
0
1
1
1
2
1
3
1
4
1
5
1
6
1
7
1
8
1
9
2
0
N
N
N
N
N
N
N
L
L
L
L
L
L
L
L
M
M
M
M
M
M
F
M
M
M
M
M
F
M
M
F
F
M
M
M
M
F
F
F
F
0
0
0
0
0
0
0
8
0(
THP:
8
0
)
1
0
0(
THP:
1
0
0
)
1
7
5(
ADM:
7
5
,
DXR:
1
0
0
)
1
8
0(
ADM:
1
8
0
)
1
4
0(
ADM:
1
4
0
)
1
3
0(
THP:
1
0
0
,
ACR:
3
0
)
1
0
0(
THP:
1
0
0
)
1
7
0(
THP:
1
2
0
,
MI
T:
2
0
,
ACR:
3
0
)
2
0
0(
ADM:
2
0
0
)
2
2
0(
THP:
2
2
0
)
2
2
0(
I
DAR:
1
2
0
,
THP:
2
0
)
2
5
0(
DNR:
5
0
,
ADM:
2
0
0
)
2
7
0(
ADM:
2
7
0
)
2
1
2
2
M
M
F
F
3
0
0(
ADM:
2
0
0
,
DNR:
1
0
0
)
3
0
0(
ADM:
3
0
0
)
2
3
2
4
2
5
2
6
2
7
M
M
M
M
M
F
F
M
M
F
3
0
0(
ADM:
2
0
0
,
DNR:
1
0
0
)
3
0
5(
THP:
9
0
,
MI
T:
3
5
,
ACR:
1
8
0
)
3
3
0(
DNR:
1
8
0
,
ACR:
1
5
0
)
3
3
0(
DNR:
1
8
0
,
ACR:
1
5
0
)
3
6
0(
ADM:
3
6
0
)
2
8
2
9
3
0
3
1
3
2
3
3
3
4
3
5
3
6
3
7
M
M
M
M
H
H
H
H
H
H
F
M
M
F
M
M
F
M
M
F
2
2
0(
THP:
2
2
0
)
2
3
2(
THP:
1
0
0
,
I
DAR:
1
3
2
)
3
0
0(
ADM:
2
0
0
,
DNR:
1
0
0
)
3
7
5(
THP:
3
7
5
)
4
2
0(
ADM:
4
2
0
)
4
9
0(
ADM:
5
0
,
EPR:
4
4
0
)
5
4
0(
ADM:
3
6
0
,
THP:
1
8
0
)
6
0
0(
DNR:
6
0
,
THP:
3
6
0
,
ACR:
1
8
0
)
8
4
0(
DNR:
1
4
0
,
THP:
7
2
0
)
4
6
0(
ADM:
3
6
0
,
THP:
1
0
0
)
a
gea
tt
e
s
t
di
a
gno
s
i
s
8
y1
1
m
1
5
y9
m
1
2
y2
m
1
6
y8
m
1
4
y6
m
1
3
y2
m
1
1
y2
m
1
3
y2
m
8
y1
1
m
2
8
y3
m
1
7
y9
m
3
y7
m
1
2
y1
0
m
6
y9
m
1
8
y0
m
9
y5
m
1
1
y0
m
1
1
y0
m
7
y5
m
3
y8
m
ALL
ALL
ALL
ALL
ALL
ALL
ALL
ALL
ALL
ALL
ALL
LCH
ALL
ALL
ALL
NHL
ALL
ALL
ALL
Ewi
ng
s
a
r
c
o
ma
ALL
Wi
l
ms
t
umo
r
ALL
ANLL
ALL
ALL
Ewi
ng
s
a
r
c
o
ma
ALL
ALL
ALL
ANLL
Ne
ur
o
bl
a
s
t
o
ma
NHL
ANLL
ANLL
NHL
ANLL
7
y0
m
9
y5
m
8
y0
m
1
5
y1
1
m
1
8
y4
m
1
5
y5
m
8
y1
0
m
7
y0
m
1
5
y0
m
1
6
y9
m
1
3
y0
m
1
3
y3
m
9
y6
m
1
8
y4
m
1
8
y0
m
6
y8
m
1
6
y8
m
dur
a
t
i
o
npo
s
t
ATCt
he
r
a
py
5
y7
mo
s
6
y7
mo
s
5
y6
mo
s
4
y7
mo
s
4
y8
mo
s
7
y2
mo
s
6
y2
mo
s
5
y1
1
mo
s
5
y7
mo
s
1
0
y2
mo
s
1
3
y0
mo
s
1
y6
mo
s
8
y1
1
mo
s
3
y9
mo
s
4
y8
mo
s
2
y8
mo
s
2
y4
mo
s
4
y3
mo
s
3
y6
mo
s
1
y4
mo
s
4
y2
mo
s
5
y6
mo
s
4
y6
mo
s
4
y9
mo
s
1
2
y7
mo
s
1
1
y1
0
mo
s
3
y8
mo
s
3
y2
mo
s
3
y6
mo
s
3
y5
mo
s
9
y1
mo
s
8
y4
mo
s
4
y2
mo
s
9
y2
mo
s
4
y6
mo
s
2
y3
mo
s
8
y1
0
mo
s
M:ma
l
e
,F:f
e
ma
l
e
,ATC:a
nt
hr
a
c
yc
l
i
ne
,ALL:a
c
ut
el
ympho
bl
a
s
t
i
cl
e
uke
mi
a
,ANLL:a
c
ut
e no
nl
ympho
bl
a
s
t
i
c
,LCH:La
nge
r
ha
ns c
e
l
l hi
s
t
i
o
c
yt
o
s
i
s
,NHL:no
nHo
dgi
ki
n’
sl
ympho
ma
.ADM:do
xo
r
ubi
c
i
n,DNR:
l
e
uke
mi
a
TPH:
pi
r
a
r
ubi
c
i
n,
MI
T:
mi
t
o
xa
nt
r
o
ne
,
ACR:
a
c
l
a
r
ubi
c
i
n
da
uno
r
ubi
c
i
n,
I
DAR:
i
da
r
ubi
c
i
n,
stopped under the following conditions: if the subject
Dobutamine Stress Protocol
experienced intolerable
chest
pain,
palpitations,
Dobutamine was infused at an initial rate of 5 μg!
headache, nausea, or other symptoms; if the systolic
kg!
min for 3 minutes, and the infusion rate was
blood pressure rose to >200 mmHg; if frequent
increased by 5 μg!
kg!
min every 3 minutes to a
episodes of ventricular arrhythmia were observed;
maximum
of
30 μg!
kg!
min.
Infants
and
small
or if sustained ventricular tachycardia was observed.
children were sedated during the dobutamine stress
Throughout
test. Administration of dobutamine was prematurely
monitoring was performed. Heart rate and blood
236
this
protocol,
continuous
ECG
J Nippon Med Sch 2010; 77 (5)
Anthracycline Cardiotoxicity
pressure were recorded at baseline and after each
echocardiogram was recorded in the standard left
stage of dobutamine infusion, and the double
ventricular (LV) short axis view at the level of the
product (DP: defined as heart rate multiplied by
chordae tendineae, with the M-mode cursor angled
systolic pressure) was calculated as an index of
through the center of the LV cavity. We measured
stress volume.
the LV end-systolic and end-diastolic dimensions
(LVDs and LVDd), and the end-systolic and end-
ECG and QT Analysis
diastolic posterior wall thickness (PWTs, PWTd). We
Standard 12-lead ECGs were recorded at a paper
calculated the following indices: 1) LV ejection
speed of 25 mm!
s for each study subject in the
fraction (EF)=(LVDd3 LVDs3)!
LVDd3, as an index
supine position with Cardio Multi FDX-4520 (Fukuda
of cardiac performance; 2) end-systolic wall stress
Denshi, Tokyo, Japan). Subjects were required to lie
(ESS)=P
LVDs
1.35!
4
PWTs
(1 + PWTs!
15
supine for 5 minutes for stabilization before ECGs
LVDs) , where P is the LV end-systolic pressure
were recorded. All ECGs were sampled at 250 Hz
calculated from the measured upper limb systolic
with simultaneous 12-lead recordings, and digitized
blood pressure (P=0.66
systolic blood pressure +
16
data were saved to a floppy disk for automated
13.5 ), as an index of LV after-load; 3) percentage LV
analysis. For each ECG, QT intervals in each lead
posterior wall thickening (%PWT)=100
were
manual
PWTd)!
PWTd, as an index of the rate of change of
modification of the computerized recognition of the
LV wall thickness. Pulsed Doppler echocardiograms
T-wave offset. The T-wave offset was detected as
were obtained in the left parasternal 4-chamber
the intersect of the T-P isoelectric baseline with the
view. The sample volumes were placed on the mitral
least-squares-fit line around the target to the T-wave
valve annulus, and the angle between the Doppler
downslope. The heart-rate corrected QT (QTc) was
beam and the presumed mitral flow vectors was
calculated using the Bazett formula: QTc=QT!
"RR
kept as small as possible. We measured the
interval. The QT intervals were measured from the
maximum early filling peak velocity (E) and the
QRS complex to the end of the T wave. If a U wave
atrial contraction peak velocity (A) from the LV
was present, the T wave offset was defined as the
transmitral flow wave recordings, and calculated E!
nadir between the T and U waves. If the T wave
A as an index of diastolic function.
automatically
calculated
without
offset could not be identified, the lead was excluded
The
investigators
who
interpreted
(PWTs
the
QT
from analysis. The QTd, which is defined as the
dispersion, M-mode echocardiograms, and pulse
difference between the maximum and minimum QT
Doppler echocardiograms were blinded to
intervals, was derived for each recording. The heart-
clinical data.
the
rate corrected QTd (QTcd) was calculated with the
Bazett formula.
Statistical Analysis
Differences among the groups were analyzed at
Echocardiography
and
Pulsed
Doppler
Echocardiography
each stage with one-way analysis of variance
(Scheffe s method). Differences with a probability
After 5 minutes of rest, systolic and diastolic blood
pressures were measured in the upper limb by
value
of
p<0.05
were
considered
statistically
significant.
means of a manual sphygmomanometer with a 5-, 9-,
or 14-cm cuff. Echocardiography and pulsed Doppler
Results
echocardiography were performed with a HewlettPackard SONOS-2500 (Hewlett-Packard, Palo Alto,
CA, USA) with a
5- or
3.5-MHz
transducer.
Clinical Data of the Patients and Control
Subjects
Phonocardiograms, indirect carotid pulse tracing,
There were no significant differences in the levels
and ECGs were simultaneously recorded at a paper
of hemoglobin or electrolytes between any of the
speed
groups (Table 2).
of
50 mm!
s.
J Nippon Med Sch 2010; 77 (5)
The
2-dimensional
237
Y. Uchikoba, et al
"200 mg!
m2. When the cut-off value for normal
Ta
bl
e2 He
mbl
o
bi
na
nde
l
e
c
t
r
o
l
yt
e
s
+
2
+
Na
K+
Ca
(
mEq/
L) (
mEq/
L) (
mg/
dL)
Hb
(
g/
dL)
c
o
nt
r
o
l
N
L
M
H
1
3
.
5
±0
.
8
1
2
.
6
±0
.
6
1
1
.
9
±0
.
9
1
2
.
6
±0
.
8
1
2
.
1
±0
.
7
1
4
1
.
4
±4
.
3
1
3
9
.
8
±3
.
6
1
4
0
.
2
±2
.
9
1
4
2
.
3
±4
.
9
1
4
0
.
6
±5
.
2
4
.
3
±0
.
3
4
.
2
±0
.
2
4
.
5
±0
.
3
4
.
2
±0
.
2
4
.
1
±0
.
2
9
.
4
±0
.
2
9
.
6
±0
.
3
9
.
4
±0
.
2
9
.
7
±0
.
4
9
.
5
±0
.
2
QTd was set at <50 milliseconds17,18, 68.8% (11 of 16)
of the patients in group M and 83.3% (5 of 6) of
patients in group H had an abnormal QTd. After
administration of dobutamine at 5 μg!
kg!
min, the
results were the same as those at rest. After
administration of dobutamine at 30 μg!
kg!
min, QTd
and QTcd were significantly greater in patients
Hb:
he
mo
gl
o
bi
n
from group L (56.5
6.4, 81.3
4.8, 79.6
8.4), group M (61.2
8.5), or group H (64.3
7.7, 83.0
10.5)
than in the other 2 groups or in healthy control
Hemodynamic
Changes
before
and
after
subjects (p<0.05) (Table 4). With a QTd cut-off value
of <50 milliseconds, 5 of the 8 patients (62.5%) in
Dobutamine Stress
or
group L, 15 of the 16 patients (93.8%) in group M,
dobutamine
and all 6 patients in group H had an abnormal QTd.
administration, and all subjects were a given the full
On the other hand, there were no significant
dobutamine dose of 30 μg!
kg!
min. In each group,
differences in QTd or QTcd between group N and
the heart rate and systolic blood pressure increased
the control subjects at rest or after administration of
significantly from those at rest to those after
dobutamine at 5 or 30 μg!
kg!
min.
No
subjects
arrhythmias
administration
showed
in
of
any
response
dobutamine
symptoms
to
at
30 μg!kg!min.
There were no significant differences between any
Correlation between Cumulative Anthracycline
of the groups at rest or after administration of
Dose and QTd at Rest and after Dobutamine
dobutamine at 30 μg!
kg!
min. In all groups, DP was
Stress at 30 μg!
kg!
min.
greater after administration of dobutamine at 30 μg!
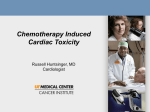
We tested the correlation between cumulative
kg!
min than at rest or after low-dose dobutamine
anthracycline dose and QTd after dobutamine stress
administration. In all groups, the mean DP increased
at 30 μg!
kg!
min, and found a good correlation using
significantly up to 20,000, which is thought to be a
the following correlation formula: y=0.051x + 42.2
practical exercise volume after administration of
(r=0.81, p<0.001) (Fig. 1). This correlation suggests
dobutamine at 30 μg!
kg!
min (Table 3).
that QTd was worse at the highest cumulative
anthracycline dose. The cut-off value for detection of
QTd, QTcd Values at Rest, and after Low- and
abnormal
cardiac
reserve
function
was
at
a
2
cumulative anthracycline dose of 152.9 mg!
m , which
High-dose Dobutamine Stress
We could not identify the T wave offset in 4
was
calculated
using
the
correlation
formula
patients at high-dose dobutamine stress, which
between QTd and cumulative anthracycline dose.
included leads I and aVL in 2 patients from groups M
The sensitivity and specificity for detection of
and H, lead aVL in 1 patient from group M, and lead
anthracycline cardiotoxicity based on our findings of
V1 in 1 patient from group L. We examined whether
abnormal QTd ("50 milliseconds) after high-dose
sex affected QTd and found that QTd is not sex-
dobutamine stress in patients with a cumulative
dependent (male QTd: 44.5
anthracycline dose of >150 mg!
m2 were 96.0% and
3.9, female QTd: 46.3
4.1). At rest, QTd and QTcd were significantly
83.3%, respectively. This finding shows that patients
greater in groups M and H (group M: 51.3
receiving a cumulative dose of anthracycline of
3.6, group H: 52.1
4.1, 54.0
4.5, 52.8
3.4) than in the
150 mg!
m2
or
more
display
subclinical
other 3 groups or in healthy control subjects (p<
electrophysiological
0.05). This finding indicates that inhomogeneity of
Thus, QTd is a reliable predictor of anthracycline
ventricular repolarization occurred even at rest in
cardiotoxicity
patients who received an anthracycline dose of
anthracyclines,
238
anthracycline
in
and
patients
cardiotoxicity.
treated
subclinical
with
myocardial
J Nippon Med Sch 2010; 77 (5)
Anthracycline Cardiotoxicity
Ta
bl
e3 Ca
r
di
o
va
s
c
ul
a
rhe
mo
dyna
mi
cc
ha
nge
sbe
f
o
r
ea
nda
f
t
e
rdo
but
a
mi
nes
t
r
e
s
s
gr
o
up HRr
e
s
t
HR
DOB5
HR
DOB3
0
s
ysBP
r
e
s
t
s
ysBP
DOB5
s
ysBP
DOB3
0
DPr
e
s
t
DPDOB5
DPDOB3
0
c
o
nt
r
o
l7
1
.
6
±1
2
.
27
5
.
3
±1
6
.
31
2
1
.
7
±2
0
.
81
0
9
.
1
±1
2
.
31
2
3
.
8
±1
1
.
21
6
6
.
3
±1
9
.
47
,
7
8
4
±6
8
49
,
4
3
6
±1
,
6
7
92
0
,
8
9
2
±1
,
1
2
6
N
6
5
.
0
±1
1
.
26
7
.
1
±1
0
.
21
2
1
.
3
±9
.
1 1
0
7
.
1
±6
.
7 1
2
4
.
3
±1
0
.
41
6
6
.
2
±1
4
.
07
,
6
0
8
±8
3
2 9
,
5
6
3
±9
5
6 2
1
,
4
5
4
±9
6
9
L
7
3
.
1
±1
6
.
67
2
.
0
±1
2
.
31
2
0
.
4
±2
8
.
91
0
7
.
2
±1
2
.
01
2
2
.
5
±1
2
.
31
6
3
.
2
±1
7
.
17
,
8
0
3
±7
6
6 9
,
4
5
7
±8
8
7 2
1
,
7
9
8
±9
4
5
M
7
3
.
4
±1
1
.
17
2
.
6
±1
2
.
61
2
5
.
2
±1
9
.
81
0
0
.
9
±1
2
.
61
2
5
.
4
±1
4
.
71
5
0
.
5
±1
8
.
88
,
0
2
1
±8
9
69
,
1
3
8
±1
,
2
3
62
2
,
1
0
5
±1
,
2
0
3
H
6
8
.
8
±9
.
9 8
3
.
5
±3
6
.
41
3
7
.
0
±1
5
.
41
0
0
.
5
±1
0
.
51
2
3
.
0
±5
.
3 1
5
4
.
0
±1
8
.
67
,
9
9
6
±9
1
31
0
,
1
6
6
±2
,
0
7
62
1
,
3
2
6
±1
,
0
2
6
HR:
he
a
r
tr
a
t
e
,
DOB:
do
but
a
mi
ne
,
s
ysBP:
s
ys
t
o
l
i
cbl
o
o
dpr
e
s
s
ur
e
,
DP:
do
ubl
epr
o
duc
t
Ta
bl
e4 QTda
ndQTc
dva
l
ue
sa
tr
e
s
t
,
a
f
t
e
rDOB5μg/
kg/
mi
nut
ea
nd3
0μg/
kg/
mi
nut
es
t
r
e
s
s
c
o
nt
r
o
l
N
L
M
H
QTdr
e
s
t
(
ms
e
c
)
QTdDOB5
(
ms
e
c
)
QTdDOB3
0
(
ms
e
c
)
QTc
dr
e
s
t
(
ms
e
c
)
QTc
dDOB5
(
ms
e
c
)
QTc
dDOB3
0
(
ms
e
e
c
)
3
7
.
1
±9
.
0
3
8
.
7
±3
.
6
3
9
.
1
±4
.
6
*
5
1
.
3
±4
.
5
*
5
2
.
1
±4
.
1
4
1
.
1
±7
.
8
3
9
.
2
±4
.
6
4
1
.
1
±4
.
2
*
5
1
.
7
±5
.
3
*
5
2
.
2
±6
.
8
4
2
.
6
±7
.
9
4
1
.
2
±4
.
6
*
5
6
.
5
±4
.
8
*
6
1
.
2
±6
.
4
*
6
4
.
3
±7
.
7
4
4
.
1
±1
0
.
9
4
4
.
7
±7
.
8
4
3
.
1
±6
.
0
*
5
2
.
8
±3
.
6
*
5
4
.
0
±3
.
4
4
6
.
8
±1
3
.
1
4
7
.
2
±5
.
6
4
8
.
3
±7
.
1
*
5
6
.
6
±6
.
5
*
5
7
.
3
±8
.
4
5
7
.
8
±9
.
8
5
8
.
3
±7
.
9
*
7
9
.
6
±8
.
4
*
8
1
.
3
±8
.
5
*
8
3
.
0
±1
0
.
5
QTd:
QT di
s
pe
r
s
i
o
n,
QTc
d:
c
o
r
r
e
c
t
e
dQT di
s
pe
r
s
i
o
n
*p
<0
.
0
5vs
.
o
t
he
rgr
o
ups
cardiotoxicity was a cumulative anthracycline dose
of 526.3 mg!
m2, which seems far less sensitive for
detecting anthracycline cardiotoxicity.
EF, ESS, E!
A, and %PWT at Rest and after
Low- and High-dose Dobutamine Stress
We could perform cardiac performance tests for 7
of 10 control subjects, all patients of group N, 7 of 8
patients of group L, 14 of 16 patients of group M,
and all patients of group H. At rest and after
Fi
g.1 Co
r
r
e
l
a
t
i
o
n
be
t
we
e
n
c
umul
a
t
i
ve
a
nt
hr
a
c
yc
l
i
nedo
s
ea
ndQT di
s
pe
r
s
i
o
na
f
t
e
r
kg/
mi
n.
do
but
a
mi
nes
t
r
e
s
sa
t3
0μg/
The Y a
xi
ss
ho
ws QT di
s
pe
r
s
i
o
na
f
t
e
r
do
but
a
mi
nes
t
r
e
s
sa
t3
0μg/
kg/
mi
n,
a
ndt
he
hr
a
c
yc
l
i
ne
Xa
xi
ss
ho
wst
hec
umul
a
t
i
vea
nt
do
s
e
.The
r
ewa
sago
o
dc
o
r
r
e
l
a
t
i
o
nbe
t
we
e
n
t
he
s
ei
ndi
c
e
s
,wi
t
hac
o
r
r
e
l
a
t
i
o
nf
o
r
mul
ao
f
1
x+ 4
2
.
2(
r
=0
.
8
1
,
p<0
.
0
0
1
)
.
y=0
.
0
5
dobutamine stress at 5 μg!
kg!
min, E!
A and %PWT
were significantly lower in group H than in the
other 4 groups. After dobutamine stress at 30 μg!
kg!
min, groups M and H showed ESS, E!
A, and
%PWT values that were significantly different from
those of the other 3 groups. Increases in ESS and
decreases in %PWT were due to reduced endsystolic LV wall thickness (data not shown), and
decreases
in
E!A
indicated
reduced
diastolic
abnormalities can develop in patients receiving a
function. These results suggest that patients with a
cumulative anthracycline dose of "150 mg!
m2. On
cumulative m2dose of "400 mg!
m2 had subclinical
the other hand, we found a good correlation
decreases in LV muscle volume and subclinical
between anthracycline dose and QTd at rest using
increases in LV wall stiffness. On the other hand,
the following correlation formula: y=0.04x + 28.9 (r=
there were no significant differences in EF among
0.78, p<0.001). When the abnormal value was 50
the 5 groups at rest, after dobutamine stress at 5
milliseconds, the cut-off value for detection of
μg!
kg!
min, or after dobutamine stress at 30 μg!
kg!
J Nippon Med Sch 2010; 77 (5)
239
Y. Uchikoba, et al
Ta
bl
e5
1 EFa
ndESSva
l
ue
sa
tr
e
s
t
,
a
f
t
e
rDOB5μg/
kg/
mi
nut
ea
nd3
0μg/
kg/
mi
nut
es
t
r
e
s
s
c
o
nt
r
o
l
N
L
M
H
EFr
e
s
t
EFDOB5
EFDOB3
0
ESSr
e
s
t
ESSDOB5
ESSDOB3
0
6
4
.
1
±6
.
0
6
8
.
3
±3
.
6
6
2
.
5
±9
.
1
6
1
.
6
±8
.
3
5
8
.
7
±9
.
5
6
9
.
7
±9
.
6
7
4
.
9
±3
.
6
7
0
.
4
±8
.
7
6
7
.
0
±8
.
4
6
8
.
7
±4
.
9
7
9
.
0
±4
.
7
8
0
.
9
±4
.
8
7
8
.
0
±7
.
7
7
5
.
8
±1
0
.
8
8
1
.
0
±1
.
0
5
5
.
1
±7
.
0
5
5
.
8
±6
.
3
5
6
.
6
±2
.
1
5
4
.
7
±8
.
7
5
8
.
8
±1
4
.
8
5
4
.
2
±3
.
2
5
5
.
3
±2
.
9
5
6
.
4
±9
.
1
5
6
.
2
±8
.
6
6
1
.
6
±1
7
.
5
5
1
.
1
±2
.
5
5
2
.
3
±3
.
1
5
1
.
5
±2
.
1
*
6
3
.
9
±7
.
1
*
6
2
.
2
±1
3
.
1
*p
EF:
e
j
e
c
t
i
o
nf
r
a
c
t
i
o
n,
ESS:
e
nds
ys
t
o
l
i
cl
e
f
tve
nt
r
i
c
ul
a
rwa
l
ls
t
r
e
s
s
,
<0
.
0
5vs
.
o
t
he
rgr
o
ups
Ta
bl
e5
2 E/
Aa
nd%PWT va
l
ue
sa
tr
e
s
t
,
a
f
t
e
rDOB5μg/
kg/
mi
nut
ea
nd3
0μg/
kg/
mi
nut
es
t
r
e
s
s
c
o
nt
r
o
l
N
L
M
H
E/
Ar
e
s
t
E/
A DOB5
E/
A DOB3
0
%PWT r
e
s
t
%PWT DOB5
%PWT DOB3
0
2
.
0
±0
.
1
2
.
1
±0
.
2
2
.
1
±0
.
1
2
.
0
±0
.
2
*
1
.
7
±0
.
2
2
.
2
±0
.
1
2
.
3
±0
.
1
2
.
3
±0
.
2
2
.
1
±0
.
3
*
1
.
8
±0
.
2
1
.
5
±0
.
1
1
.
4
±0
.
1
1
.
6
±0
.
2
*
1
.
2
±0
.
1
*
1
.
0
±0
.
1
9
6
.
2
±1
.
6
9
4
.
8
±4
.
3
9
1
.
2
±4
.
6
9
1
.
7
±3
.
2
*
6
8
.
9
±6
.
1
1
1
5
.
3
±5
.
6
1
1
8
.
6
±7
.
6
1
0
9
.
1
±9
.
5
1
1
2
.
4
±6
.
1
*
9
2
.
4
±1
1
.
2
1
3
2
.
7
±5
.
7
1
3
4
.
8
±4
.
9
1
3
5
.
8
±2
6
.
3
*
9
6
.
2
±3
.
8
*
9
2
.
2
±5
.
5
E/
A:r
a
t
i
oo
ft
hema
xi
mum e
a
r
l
yf
i
l
l
i
ngpe
a
kve
l
o
c
i
t
y(
E)a
ndt
hea
t
r
i
a
lc
o
nt
r
a
c
t
i
o
npe
a
kve
l
o
c
i
t
y(
A)
,%PWT:
pe
r
c
e
nt
a
gel
e
f
tve
nt
r
i
c
ul
a
rpo
s
t
e
r
i
o
rwa
l
lt
hi
c
kne
s
s
*p
<0
.
0
5vs
.
o
t
he
rgr
o
ups
min. These findings suggest that even the highest
2
cardiomyopathy have been described. Most studies
cumulative m doses in the patients did not reduce
support the view that an increase in oxidative stress
LV systolic function (Table 5-1, 5-2). These findings
(evidenced by increases in free radicals and lipid
using 2-dimensional echocardiography and pulse
peroxidation and decreases in antioxidants and
Doppler echocardiography are similar to the findings
sulfhydryl groups) plays an important role in the
we obtained in our previous study14.
pathogenesis of anthracycline cardiomyopathy21,22.
The unique sensitivity of the myocardium to
Discussion
anthracyclines may be due to the low levels of
catalase
Late cardiotoxic effects of anthracycline are an
increasing problem for survivors of childhood cancer.
and
superoxide
dismutase
in
cardiac
23
myocytes .
The main features of cardiac biopsies from
Anthracycline-induced congestive heart failure is a
anthracycline-treated
dose-dependent phenomenon. Reported incidences of
vacuolization due to dilation of the sarcotubules and
anthracycline-induced congestive heart failure range
loss of myofibrils19,24. In patients who received a high
from >5% (cumulative adriamycin dose, 501 to 550
dose
2
patients
(455―500 mg!m 2 )
of
are
cytoplasmic
daunomycin,
cardiac
mg!
m ) to >30% (cumulative adriamycin dose, >601
biopsies exhibited degenerative, atrophic, and lytic
mg!
m2)19. In a long-term follow-up study, patients
lesions in cardiac muscle cells, and interstitial edema
who had no symptoms of cardiotoxicity at the time
and fibrosis23. These histological abnormalities could
of complete remission of cancer after adriamycin
strongly affect myocardial action potentials and cell-
therapy
to-cell conduction, and lead to inhomogeneity of
had
an
unusually
high
incidence
of
cardiovascular complications typical of adriamycin
20
ventricular
depolarization
and
repolarization.
cardiomyopathy over the subsequent 4 to 20 years .
Previously, we reported that anthracycline-treated
Thus, it is important to find ways to avoid or
patients
minimize the cardiotoxic side effects of anthracycline
depolarization,
in the treatment of cancer.
Several effects of anthracycline which may play
critical roles in the pathogenesis of anthracycline
240
exhibited
as
abnormal
revealed
by
ventricular
signal-averaged
25
electrocardiography . However, there have been no
other
reports
of
abnormalities
of
ventricular
repolarization in anthracycline-treated patients. QT
J Nippon Med Sch 2010; 77 (5)
Anthracycline Cardiotoxicity
dispersion is defined as the difference between the
kg!
min, patients with a very low cumulative
maximum and minimum QT interval durations on a
anthracycline dose (anthracycline dose "80 mg!
m2 )
12-lead standard ECG and is considered to reflect
had significantly greater QTd and QTcd than did
local differences in repolarization of the myocardium.
control subjects or patients who had not received an
In the present study, at rest, when the cut-off value
anthracycline.
17,18
for normal QTd was set at <50 milliseconds
With
the
cut-off
value
of
>50
, the
milliseconds, an abnormal QTd was found in 62.5%
QTd was abnormal in 68.8% of the patients with a
of patients with a cumulative anthracycline dose of
cumulative anthracycline dose of "200 mg!
m and
80 to <200 mg!
m2, 93.8% of
in
cumulative anthracycline dose of 200 to <400 mg!
m2 ,
2
83.3%
of
the
patients
with
a
cumulative
anthracycline dose of "400 mg!
m2. An abnormal
and
100%
of
patients
with
a
a
cumulative
"400 mg!m .
2
of
with
increase in QT dispersion could be caused by
anthracycline
inhomogeneity of ventricular repolarization. The
evaluated
QTc was prolonged at rest by more than 450
muscle performance under dobutamine stress using
milliseconds in only 5 of the present cases. The QTc
2-dimensional echocardiography and pulsed Doppler
may be less sensitive as an index of anthracycline
echocardiography. The values for ESS, E!
A, and
cardiotoxicity at rest than are the QTd data. On the
%PWT that we obtained were consistent with our
other hand, in the present study, 2-dimensional
previous findings25, yet were much less sensitive
echocardiography showed that only patients with a
than were the QTd and QTcd data that we obtained
cumulative anthracycline dose of "400 mg!
m2 had a
in the present study. Because these indices are
significantly reduced LV cardiac muscle volume at
calculated from changes in LV wall motion on
25
dose
patients
cardiotoxicity
by
examining
We
also
cardiac
rest, which is consistent with our previous findings .
echocardiograms, detectable changes in wall motion
It appears likely that decreased numbers of cardiac
must require much higher cumulative doses than
myocytes and increased interstitial edema and
the electrophysiological changes detected on the
fibrosis leads not only to reduced ventricular cardiac
basis of QT dispersion. Data from 2-dimensional
volume but also to abnormal microelectrical findings.
echocardiography
Our
a
echocardiography is more difficult to evaluate than
"200 mg!m ,
are data from 12-lead ECG. Moreover, whereas
electrical findings at rest indicates cardiotoxic effects
sedation may be needed for infants and small
(morphological changes in ventricular myocardium)
children when they undergo echocardiography,
that require intervention.
there is no need for sedation to perform 12-lead
findings
cumulative
show
that
anthracycline
for
patients
dose
of
with
2
and
pulsed
Doppler
Dobutamine is a synthetic catecholamine α1, β1
ECG. Thus, in terms of ease of use, QTd and QTcd
and β2 with mimetic activity. Dobutamine has
have clear advantages over ESS, E!
A, and %PWT
inotropic effects at low doses (5―10 μg!
kg!
min) and
as indices for detecting anthracycline cardiotoxicity
causes increased heart rate, blood pressure, and
that manifests as abnormal cardiac reserve function.
coronary vasodilation at high doses (>20 μg!
kg!
min).
In the present study, there was little difference
oxygen
between QTd and QTcd. Some earlier studies have
consumption in the myocardium and increase the
found no evidence that QT dispersion requires the
inhomogeneity of ventricular myocytes at moderate
same type of heart rate correction as the duration of
doses (>10 μg!
kg!
min) . These findings suggest that
the QT interval27,28. Also, clear criteria have recently
the inhomogeneity of ventricular repolarization can
been established for detecting abnormal QTd based
be increased in cardiac myocytes exposed to
on
anthracyclines.
evaluated
precise value for detecting abnormal QTcd has been
myocardial reserve function as an indicator of
established. Moreover, assessing QTd is much easier
cardiotoxicity, by performing electrophysiological
than assessing QTcd. Thus, QTd has an advantage
and morphological evaluations under dobutamine-
over QTcd as an index for detecting abnormal
induced stress. After dobutamine stress at 30 μg!
ventricular inhomogeneity.
Thease
changes
lead
to
increased
26
In
this
study,
J Nippon Med Sch 2010; 77 (5)
we
electrophysiological
findings 17,18,
whereas
no
241
Y. Uchikoba, et al
In the present study, we also assessed the
analysis.
correlation between cumulative anthracycline dose
The Bazett formula is commnly used to correct
and QTd after dobutamine stress at 30 μg!
kg!
min.
the QT interval for heart rate. Recently, the
We found a good correlation between those 2
Fridericia formula has been considered better for
variables when using the correlation formula: y=
correcting the QT interval when the heart rate is
0.051x + 42.2 (r=0.81, p<0.001) (Fig. 1). With this
high. We would have liked to use the Fridericia
formula,
cumulative
formula in the present study, especially for high
we
determined
that
a
2
anthracycline dose of 152.9 mg!
m was the cut-off for
heart rates during dobutamine stress, however, the
detecting abnormal cardiac reserve function. Based
Cardio Mulyi FDX-4520 is not formatted for the
on these results, the sensitivity and specificity for
Friderica formula. Hence, in this study the QT
detecting anthracycline cardiotoxicity as indicated
interval was corrected with the Bazett formula.
by abnormal QTd after high-dose dobutamine stress
In the present study, we did not obtain control
("50 milliseconds) in patients with a cumulative
data from children because we decided that the
anthracycline dose of >150 mg!
m2 were 96.0% and
dobutamine stress test was too invasive and that
83.3%, respectively. This finding suggests that the
healthy children should not be subjected to such a
physicians
cumulative
stress test. Also, we could not obtain age-matched
anthracycline dose of >150 mg!
m should consider
data. However, there were no significant differences
the possibility of decreased cardiac reserve function.
between the control group and any of the 3 patient
QTd appears to be a useful index for detecting
groups in the basic findings of heart rate and blood
cumulative anthracycline cardiotoxicity.
pressure, which strongly affect electrophysiological
of
patients
with
a
2
Previously, we reported that anthracycline-treated
patients exhibit abnormal ventricular depolarization,
data. Therefore, we felt that the index of age could
be ignored in this study.
as revealed by signal-averaged ECG (SAE). However,
Conclusions
the microvolt electrophysiological changes detected
with
SAE
dependent
require
on
measurement
of
several
method
QTd
criteria
and
is
a
age.
that
are
Because
convenient
and
29
Dobutamine-stress QT dispersion is a useful
method
for
detectinglate
anthracycline
independent of age and sex , it is, therefore, a much
cardiotoxicity, especially for patients who cannot
better method than SAE for detecting anthracycline
tolerate physical exercise. On the basis of these
cardiotoxicity.
findings we believe that the physicians of patients
Finally, we did not evaluate the reproducibility of
with a cumulative anthracycline dose of >150 mg!
m2
QTd in this study. Many papers have reported that
should be aware of the possibility of subclinical
the reproducibility of QT dispersion is significantly
anthracycline cardiotoxicity.
poorer than the reproducibility of the QT interval
itself. Nevertheless, despite this poor reproducibility,
References
our physicians were able to distinguish between
healthy subjects and patients with heart disease on
the basis of QT dispersion17,30,31.
Study Limitations
The most important limitation of this study was
the measurement of QT dispersion. The end of
repolarization can be difficult to define because of
flattening of the T wave or the presence of a U
wave. In the present study, when the T wave offset
could not be identified, the lead was excluded from
242
1.Bonadonna G, Monfardini S, De Lena M, FossatiBellani F, Beretta G: Phase I and II evaluation of
Adriamycine (NSC 123127). Cancer Res 1970; 30:
2572―2582.
2.Blum RH, Carter SK: Adriamycin, a new drug with
significant clinical activity. Ann Intern Med 1974; 80:
249―259.
3.Von Hoff DD, Rozencweing M, Piccart M: The
cardiotoxicity of anticancer agents. Semin Oncol
1982; 9: 23―33.
4.Legha SS, Benjamin RS, Mackay B, et al.: Reduction
of
doxorubicin
cardiotoxicity
by
prolonged
continuous intravenous infusion. Ann Intern Med
1982; 96: 133―139.
J Nippon Med Sch 2010; 77 (5)
Anthracycline Cardiotoxicity
5.Fukazawa R, Ogawa S, Hirayama T: Early detection
of anthracycline cardiotoxicity in children with acute
leukemia using exercise-based echocardiography and
Doppler echocardiography. Jpn Circ J 1994; 58: 625―
634.
6.Davy PP, Bateman J, Mulligan IP, et al.: QT interval
dispersion in chronic heart failure and left
ventricular hypertrophy: relation to autonomic
nervous system and Holter tape abnormalities. Br
Heart J 1994; 71: 268―273.
7.Poloniecki GY, Dickie S, Elliott PM, et al.: Is QT
dispersion associated with sudden cardiac death in
patients with hypertrophic cardiomyopathy? Ann
Noninvasive Electrocardiol 2001; 6: 209―215.
8.Sporton SC, Taggart P, Sutton PM, et al.: Acute
ischaemia: a dynamic influence on QT dispersion.
Lancet 1997; 349: 306―309.
9.Paventi S, Bevilacqua U, Parafati MA, et al.: QT
dispersion and early arrhythmic risk during
myocardial infarction. Angiology 1999; 50: 209―215.
10.Ichkan K, Molnar J, Somberg J: Relation of left
ventricular mass and QT dispersion in patients with
systemic hypertension. Am J Cardiol 1997; 79: 508―
511.
11. Linker NJ, Colonna P, Kekwick CA, et al.:
Assessment of QT dispersion in symptomatic
patients with congenital long QT syndromes. Am J
Cardiol 1992; 69: 634―638.
12.Zareba W, Moss AJ, Le Cessie S: Dispersion of
ventricular repolarization and arrhythmic cardiac
death in coronary artery disease. Am J Cardiol 1994;
74: 550―553.
13.Nahshoni E, Gur S, Marom S, et al.: QT dispersion in
patients with social phobia. J Affective Disorders
2004; 78: 21―26.
14.Hamada H, Ohkubo T, Maeda M, Ogawa S:
Evaluation of cardiac reserved function by high-dose
dobutamine-stress
echocardiography
in
asymptomatic anthracycline-treated survivors of
childhood cancer. Pediatrics International 2006; 48:
313―320.
15.Grossman W, Jones D, McLaurin LP: Wall stress and
patterns hypertrophy in the human left ventricle. J
Clin Invest 1979; 56: 56―64.
16.Marsh DJ, Green LK, Wynne J, Cohn PF, Grossman
W: Left ventricular end-systolic pressure-dimensio
and stress-length relations in normal human
subjects. Am J Cardiol 1988; 12: 426―440.
17.Kautzner J, Yi G, Camm AJ, Malik M: Short- and
long-term reproducibility of QT, QTc, and QT
dispersion measurement in healthy subjects. PACE
1994; 17: 928―937.
18.Linker NJ, Colonna P, Kekwick CA, Till J, Camm J,
Ward DF: Assessment of QT dispersion in
symptomatic patients with congenital long QT
J Nippon Med Sch 2010; 77 (5)
syndromes. Am J Cardiol 1992; 69: 634―638.
19.Lefrak EA, Pitha J, Rosenheim S, Gottleib JA: A
clinicopathologic
analysis
of
adriamycin
cardiotoxicity. Cancer 1973; 32: 302―304.
20.Steinhertz LJ, Steinhertz PG, Tan CTC, Heller G,
Murphy L: Cardiac toxicity 4 to 20 years after
completing anthracycline therapy. J Am Med Assoc
1991; 266: 1672―1677.
21.Singal PK, Siveski-Iliskovic N, Hill M, Thomas TP, Li
T: Combination therapy with probucol prevents
adriamycin-induced cardiomyopathy. J Mol Cell
Cardiol 1995; 27: 1055―1063.
22.Sigal PK, Iliskovic N, Li T, Kumar D: Adriamycin
cardiomyopathy: pathophysiology and prevention.
FASEB J 1997; 11: 931―936.
23.Doroshow JH, Locker GY, Myers CE: Enzymatic
defences of the mouse heart against reactive oxygen
metabolites: alterations produced by doxorubicin. J
Clin Invest 1980; 65: 128―135.
24.Buja LM, Ferrans VJ, Mayer RJ, Roberts WC,
Henderson ES: Cardiac ultrastructual changes
induced by daunorubicin therapy. Cancer 1973; 32:
771―778.
25.Fukumi D, Uchikoba Y, Maeda M, Ogawa S:
Longitudinal
evaluation
of
anthracycline
cardiotoxicity
by
signal-averaged
electrocardiography in children with cancer.
Pediatrics International 2002; 44: 134―140.
26.Horner SM, Murphy CF, Coen B, Dick DJ, Lab MJ:
Sympathomimetic modulation of load-dependent
changes in the action potential duration in the in situ
porcine heart. Cardiovasc Res 1996; 32: 148―157.
27.Malik M, Camm AJ: Mystery of QTc interval
dispersion. Am J Cardiol 1997; 79: 785―787.
28.Zabel M, Wolfgang J: Rate dependence of the QT
interval and QT dispersion: comparison of atrial
pacing and exercise testing. Circulation 1997; 96
(suppl I): I-325.
29.Macfarlane PW, McLaughlin SC, Rodger CR:
Influence of lead selection and population on
automated
measurement
of
QT
dispersion.
Circulation 1998; 98: 2160―2167.
30.Nowinski K, Bergfeldt L: Normal response of the
QT interval and QT dispersion following intravenous
injection
of
the
sodium
channel
blocker
disopyramide: methodological aspects. Cardiovasc
Drugs Ther 1995; 9: 573―580.
31.Savelieva I, Gang Y, Guo W, Hnatkova K, Malik M:
Agreement and reproducibility of automatic versus
manual measurement of QT interval and QT
dispersion. Am J Cardiol 1998; 81: 471―477.
(Received, January 8, 2010)
(Accepted,
May 29, 2010)
243