Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
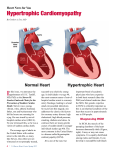
HYPERTROPHIC CARDIOMYOPATHY: Cellular changes of myocytes. Cell disarrangement ise seen on microscope. Left: Organized and parallel cell arrangement in normal myocardium. Right: Disarrangement affects impuls conduction and promotes ventricular arrythmias. HCM: Symtomps: Angina, Dyspne, Presyncope, Syncope. Physical Findings: 1- Before LV beat, LA beat is palpated (S4): Is present even in the absence of any gradient or murmur. Impaired LV relaxation. 2- LVOT Sistolik ejectıon Murmur: Crescendo-Decrescendo, starts with S1 and ends with S2. Best heard between apex and left sternal border. Cervical radiation is weak. Augmented by manouvers and drugs which decrease preload. (Valsalva, standing, amyl nitrite). Attenuates with increasing afterload (squating, handgrip fenilefrin). 3- MR murmur: Heard at late systole, radiates to axilla, and related with LV outflow obstruction. Mitral diastolic rumble and Paradoxic splitting of S2 may be heard. 4- Hyperdynamic carotis pulse. HCM: Clinical Presentation and Mechanisms Chest pain: Ischemia, LVOT ob. Reduced coronary perfusion pressure. Exertional dyspnea: Diastolic dysfunction. Reduced functional capacity: LVOTob, systolic dysfunction, AFwith uncontrolled rapid ventricular rate. Palpitation: SVT, AF, frequent VPB, non-sustained VT. Syncope/Presyncope: Supraventricular arrythmia, LVOTob, vasovagal, high VT rate . İnadequate increase cardiac output during the effort. Cardiac arrest: VT, SVT, AF, VF, bradyarrythmia. HCM: Other manifestations. Atrial Fibrillation Seen in %15 of patients with HCM. Absence of atrial systole. Rapid ventricular rate causes pulmonary edema or hypotension. Rapid ventricular rate causes detoriation of functional capacity. By conversion to sinus rythm or decreasing heart rate functional capacity improves. Endocarditis: May occur on aortic or mitral valves. Unexpected heart failure and IE symptoms or signs should be suggest İE in HCM patiernts. HCM: ECG and CHEST FİLM Chest film: May be normal-large left heart chambers. . No aortic calcification. ECG: Is anormal in %97 of symptomatic HCMP, and in %90 of asymptomatic HCMP patients. AF is detected in %15. Non-sustained VT is frequent. . Q waves in DII, DIII, aVF and D1, aVL, V5, V6 (and less frequently in V1-3). This sign shows hypertrophy, and causes pseudoinfarct patern. Intraventricular conduction delay. High voltage findings of LVH. T waves of LVH. Huge negative T waves are frequently seen in apical HCMP high precordial QRS voltage. Short PR and pre-exitation may be seen, but is infrequent. HCM: Characteristic ECG paterns. Left axis deviation LBBB Pathologic Q wave on anterolateral leads. T wave inversion (commonly in İnferolateral leads) ST segment changes. Criteria for left atrial enlargement. V3-5 or V4-6 huge T wave inversion (“Distal- apikal HCM” HCM: Pseudoinfarction patern, Q wave. HCMP: Echocardiographic Hallmarks Asymetric (dispropotionate) septal thickening: Septum to posterior wall ratio > 1.5 LV myocardial segment >1.5 cm in thicknesss. Poor Septal contractıon. Hypercontractile free posterior wall. Systolic anterior motıon of the mitral valve (SAM) when outflow tract gradient >30 mmHg . Mid-systolic closure of aortic valve. Small LV cavity. Mitral regurgitation is frequent. LVOT gradient at rest present in about %35 of patients Hypertrophic obstructive cardiomyopathy (HOCM): As Mitral valve changes:When the LVOTis narrowed, blood rushes through the passageway toward the aortic valve dragging the leaflets of the mitral valve with it. Mitral valve normally functıons keep blood floıwing in direction from the left atrium (upper heart chamber) to the LV. However increased force of blood caused by HCM pulls the valve open and may cause blood leak backward (called regurgitatıon )into the LA. NORMAL LVOTobs. Anterıor replacement of the papillary muscle in HOCM : MR, Systolic anterior motion (SAM) HCM vs Athlete’s Heart HCM + + + + + + + Unusual pattern of LVH LV cavity <45 mm LV cavity >55 mm LA enlargement Bizarre ECG paterns Abnormal LV filling Female gender thickness with deconditioning Family history of HCM Circulation 1995; 91:1596 Athlete + + - HOCM: Septal myectomy: Before the operatıon There is severe hypertrophy of the basal septum, whith systolic anterior motıon of the mitral valve (-A-). This results in severe LVOT obs. as well as MR. During the surgery (-B ), yhe portıon of the basal septum that project into the outflow tract is removed by scalpel, resulting in abolitıon of the LVOTobs. (-C-). There is no longer SAM, and theMR abolished. HOCM: Septal ablation (with absolute ethanol). İndication: LVOT gradient at rest > 30-50 mmHg. With provocation 75-100 mmHg. HOCM: Decreased LVOT gradient after septal ablation. Restictive Cardiomyopathy Tanım: Ventriküler sertliğin daha farklı mekanizma/patolojilerle artış gösterdiği bir grup bozukluğu temsil etmektedir. İnfiltrtif , inflamatuar veya metabolik hastalıkların sonucunda restriktif kardiyomyopati gelişebilir. Idiopathic Dilated Cardiomyopathy IDC - Definition a disease of unknown etiology that principally affects the myocardium LV dilatation and systolic dysfunction pathology increased heart size and weight ventricular dilatation, normal wall thickness heart dysfunction out of portion to fibrosis Incidence and Prognosis 3-10 cases per 100,000 20,000 new cases per year in the U.S.A. death from progressive pump failure 1-year 2-year 5-year 25% 35-40% 40-80% stabilization observed in 20-50% of patient complete recovery is rare Observed Survival of 104 Patients 120 104 100 80 72 60 56 51 45 40 37 35 31 24 20 19 16 0 0 1 2 3 4 5 6 7 Years Am J Cardiol 1981; 47:525 8 9 10 Predicting Prognosis in IDC Predictive Possible Not Predictive Clinical factors symptoms age duration viral illness Hemodynamics LVEF Cardiac index LV cond delay complex VPC alcoholism peripartum family history LV size atrial pressure AV block atrial fibrillation myofibril volume Dysarrhythmia Histology Neuroendocrine hyponatremia plasma norepinephrine atrial natriuretic factor simple VPC other findings Clinical Manifestations Highest incidence in middle age blacks 2x more frequent than whites men 3x more frequent than women symptoms may be gradual in onset acute presentation misdiagnosed as viral URI in young adults uncommon to find specific myocardial disease on endomyocardial biopsy History and Physical Examination Symptoms of heart failure pulmonary congestion (left HF) dyspnea (rest, exertional, nocturnal), orthpnea systemic congestion (right HF) edema, nausea, abdominal pain, nocturia low cardiac output fatigue and weakness hypotension, tachycardia, tachypnea, JVD Cardiac Imaging Chest radiogram Electrocardiogram 24-hour ambulatory ECG (Holter) lightheadedness, palpitation, syncope Two-dimensional echocardiogram Radionuclide ventriculography Cardiac catheterization age >40, ischemic history, high risk profile, abnormal ECG Clinical Indications for Endomyocardial Biopsy Definite monitoring of cardiac allograft rejection monitoring of anthracycline cardiotoxicity Possible detection and monitoring of myocarditis diagnosis of secondary cardiomyopathies differentiation between restrictive and constrictive heart disease Management Limit activity based on functional status salt restriction of a 2-g Na+ (5g NaCl) diet fluid restriction for significant low Na+ initiate medical therapy ACE inhibitors, diuretics digoxin, carvedilol hydralazine / nitrate combination Management consider adding ß-blocking agents if symptoms persists anticoagulation for EF <30%, history of thromboemoli, presence of mural thrombi intravenous dopamine, dobutamine and/or phosphodiesterase inhibitors cardiac transplantation myocardial noncompaction