Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
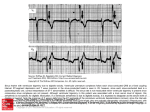
Digitalis and Baroreceptor Reflexes in Man ALBERTO FERRARI, M.D., LUISA GREGORINI, M.D., MARIA CARLA FERRARI, M.D., LAURA PRETI, M.D., AND GIUSEPPE MANCIA, M.D. SUMMARY Data in animals indicate that large amounts of digitalis potentiate arterial baroreflexes and that this factor may be important for the cardiovascular effects of the drug. To determine if arterial baroreflex potentiation also exists after administration of therapeutic doses of digitalis in man, we studied how stimulation and deactivation of arterial baroreceptors by phenylephrine and nitroglycerin injection affect heart rate and how stimulation and deactivation of carotid baroreceptors by neck suction and pressure affects blood pressure and heart rate. The study was performed in 29 normotensive or hypertensive subjects before and after injection of Lanatoside C (0.8 mg i.v.). Baroreceptor stimulation reduced heart rate and blood pressure, while baroreceptor deactivation increased both of these variables. The bradycardic and hypotensive effect of baroreceptor stimulation increased significantly after digitalis both in normotensive and hypertensive subjects. However, the tachycardic and hypertensive responses to baroreceptor deactivation were not affected by digitalis. Thus, therapeutic doses of digitalis in man enhance baroreceptor reflexes, and both the heart rate and the blood pressure reflex effects are involved. However, the enhancement occurs to a marked degree only with baroreceptor stimulation and is not evident with baroreceptor deactivation. Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 EVIDENCE from experimental animals indicates that digitalis increases the effectiveness of the arterial baroreceptor reflexes and suggests that this may be important in the clinical action of the drug. First, administration of ouabain in anesthetized cats and dogs is followed by an increased firing of the aortic and the carotid baroreceptors." 2 Second, injection of acetylstrophantidin in anesthetized dogs increases the depressor response that can be obtained by stimulation of baroreceptors in isolated carotid sinus preparations.3', Third, the bradycardia induced by digitalis in unanesthetized dogs is evident when the baroreceptors are intact, but not after sinoaortic denervation.' However, most of the studies we have mentioned have made use of doses of digitalis compounds that are greater (and often markedly so) than the doses used therapeutically. Most important, the only evidence on the effect of digitalis on baroreflexes in man are reports that digitalis may potentiate the bradycardia induced by baroreceptor stimulation,6 but perhaps only to a minor degree.7 The present study was undertaken to examine the effects of clinical doses of digitalis on human baroreceptor reflexes. We examined the reflex effects induced by baroreceptor stimulation and those resulting from baroreceptor deactivation below the existing stimulus. By using different techniques we studied both the heart rate and the blood pressure influences of the baroreflex. Our results demonstrate that digitalis has a major action on the cardiac and vascular component of the baroreflexes in man. However, this action is more complex than could be anticipated from the animal studies, as it occurs when baroreceptors are stimulated but not when they are deactivated. Methods We studied 29 subjects of both sexes (mean age 41.6 ± 2.5 years, range 21-59 years) who were hospital inpatients with either normal blood pressure or with uncomplicated essential hypertension. None of the subjects had signs of myocardial failure and none had received antihypertensive or other cardiovascular drugs in the preceding 3 weeks. Each gave free consent to the study after its nature and purpose were explained. Measurements Pulsatile arterial blood pressure was measured by a catheter (1.7 mm o.d., 11 cm long) placed percutaneously into a brachial artery and connected to a strain-gauge transducer system with an optimal frequency response curve up to 20 Hz. Mean arterial pressure was obtained by electronic damping of the pulsatile signal and by integration of the pulsatile trace over consecutive periods of 10 seconds. An ECG trace (usually lead 2) was recorded throughout the study for calculation of the RR intervals. Heart rate was also continuously measured by a cardiotachometer, the signal for which was derived either from the R wave or from the pulse-pressure signal. Methods for Studying Arterial Baroreflexes Two methods were used to study arterial baroreceptor reflexes. In the first, which is currently used, i.v. phenylephrine and nitroglycerin are injected to increase and reduce arterial blood pressure, thus stimulating and deactivating all arterial baroreceptors and causing reflex increases and decreases in RR interval.8' 9 In our study we injected intravenously a bolus of 50-100 ,g of phenylephrine, which induced a progressive rise in systolic and diastolic pressures with a maximal increase of 20-30 mm Hg above the pressure values before the injection, and a bolus of 100-150 jig of nitroglycerin, which induced a progressive fall in systolic and diastolic pressures, with From the Istituto di Patologia Medica I dell'Universita di Milano and Centro di Ricerche Cardiovascolari del CNR, Milano, Italy. Address for correspondence: Professor Giuseppe Mancia, Istituto Ricerche Cardiovascolari, Via F. Sforza 35, Policlinico 20122 Milano, Italy. Received November 8, 1979; revision accepted June 11, 1980. Circulation 63, No. 2, 1981. 279 280 CIRCULATION Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 a maximal reduction of 15-20 mm Hg below the pressures before the injection. The other method was the variable-pressure neck chamber, which permits the study of reflex changes in arterial blood pressure as well as in RR interval in response to selective stimulation and deactivation of the carotid sinus baroreceptors. We have given a detailed description of this method elsewhere. 10-12 Briefly, it consists of a collar extending inferiorly to the shoulders and superiorly to a plane intersecting the chin, the ear lobe and the occiput. The pneumatic pressure within the collar can be altered in a positive and a negative direction, the alteration being transmitted to the neck tissues outside the carotid sinuses in the respective amount of 86% and 64%.10 Thus, the positive and negative neck pressure applications cause, respectively, a reduction and an increase in carotid transmural pressure, resulting in deactivation and stimulation of the carotid sinus baroreceptors with respect to the existing stimulus. In the present study the alterations in pneumatic pressure were induced rapidly (90% of the change completed in less than 1 second) and were maintained constant for 2 minutes. The increase and the decrease in neck tissue pressure that were obtained were 30.8 ± 1.1 and 29.8 ± 1.1 mm Hg, respectively, before digitalis and 31.2 ± 1.2 and 29.2 ± 1.0 mm Hg after digitalis. We investigated subjects with normal cardiac function because the injection of phenylephrine caused similar increases in blood pressure before and after administration of digitalis in these patients, achieving comparable baroreceptor stimulation in the two conditions. In preliminary trials, this could not be obtained in patients with heart failure, in whom the phenylephrine injection caused blood pressure to increase less before than after digitalis, probably because in the former condition the heart had less ability to sustain an increased afterload. Protocol The study was made with the subjects in a supine position and began with the insertion of the arterial and the venous catheters, which was made under local anesthesia with 2% lidocaine. A 20-minute rest period was allowed to reduce possible emotional factors involved in the cannulation and to achieve satisfactory basal conditions. In 22 subjects arterial blood pressure was increased by phenylephrine and decreased by nitroglycerin, the two drugs being administered in a random order and with an interval of 10 minutes. Lanatoside C was subsequently injected intravenously at a dose of 0.8 mg, followed by an interval of 40-45 minutes to allow the drug to have its effects,'3 after which phenylephrine and nitroglycerin were administered at the same doses. In a separate group of seven subjects, the 20-minute interval after the insertion of the catheters was followed by application of one positive and one negative neck pressure, performed in a random order and separated by a 10-minute interval. Lanatoside C, 0.8 mg, was then injected intravenously and, after an VOL 63, No 2, FEBRUARY 1981 interval of 40-45 minutes, the positive and negative pressure applications were repeated at the same magnitude and with the same sequence as before. Throughout the study pulsatile arterial pressure, mean arterial pressure, arterial pressure integrated over consecutive periods of 10 seconds, heart rate and ECG were continuously recorded on a Grass polygraph. The recording was made at low speed (50 mm/min), except during the administration of phenylephrine and nitroglycerin, when a high speed (100 mm/sec) of recording was used to allow precise calculation of systolic pressure values and RR intervals during the change in pressure induced by the drugs. Data Analysis The data from the injection of phenylephrine and nitroglycerin were analyzed as described by Smith et al.8 and by Pickering et al.9 Systolic pressure was measured during the increase or the decrease induced by phenylephrine and nitroglycerin, each value being related to the RR interval on the next cardiac cycle. Linear regression lines based on 12-17 values were obtained between these two variables, the regression coefficients (i.e., the slope of the regression lines) indicating sensitivity of the reflex. Only subjects in whom there was a close significant correlation (p < 0.01) between the changes in systolic blood pressure and in RR interval both before and after administration of digitalis were considered. This happened in 18 of the 22 subjects with phenylephrine and in 20 of the 22 subjects with nitroglycerin. This technique has given reproducible results in short- and long-term studies."- ' Within each subject the regression coefficients obtained with either phenylephrine or nitroglycerin before and after administration of digitalis were compared by covariant analysis.?6 For the whole group, regression coefficients were compared by t test for paired observations. The data obtained with the neck chamber were analyzed as previously described."1 12 Mean arterial pressure and RR intervals were calculated as follows. A control period was obtained by averaging the values occurring during the 30 seconds preceding the alterations in neck chamber pressure and an early response was considered which was the average of the values occurring between the fifth and the fifteenth second that followed the alterations in neck chamber pressure. A late or steady-state response was also considered by averaging the values of the last 30 seconds of the neck chamber pressure alterations. These two responses allowed us to take into account both the initial and the late and steady-state effects of the changes in carotid baroreceptor activity.", 12 Data from each individual were pooled to obtain mean and standard error values for the whole group of subjects. The t test for paired observation was used to evaluate effects of digitalis on the responses to stimulation and deactivation of carotid sinus baroreceptors. The early and the steady-state responses were analyzed separately. Values are mean ± SEM. DIGITALIS AND BAROREFLEXES/Ferrari Results Phenylephrine (18 subjects) Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 These data are shown in table 1. In the control period the average value for mean arterial pressure was 112 mm Hg and the RR interval was 823 msec. The rise in pressure induced by phenylephrine caused a progressive lengthening of the RR interval in all subjects. The regression coefficient of RR interval on systolic pressure (expressing the sensitivity of the baroreflex) was on average 8.13 (range 2.67-15.40). Digitalis had no significant effect on basal mean arterial pressure but caused a significant increase in basal RR interval (p < 0.001). There was no significant difference in the rate or magnitude of the rise in blood pressure induced by the same dose of phenylephrine before and after digitalis. After digitalis, however, the sensitivity of the baroreflex was increased. Covariant analysis showed that the magnitude of the regression coefficient was significantly greater in 16 of the 18 subjects (fig. 1) and a significant increase was also found for the whole group by paired t test. The average of the individual regression coefficients after digitalis was 11.83, an increase of 43% over the value before digitalis (fig. 2). et al. 281 Two further points were analyzed. First, a correlation was sought between the increase in RR interval observed after digitalis in the basal period and the increased slope of the baroreflex response induced by the drug. No significant correlation was found (r = 0.285; NS). Thus, the bradycardic action of digitalis was not related to the effect of the drug on the arterial baroreflexes. Second, no significant correlation was found between the increase in the slope of the baroreflex response induced by digitalis and the value of the slope before digitalis (r = 0.322; NS). Thus, the extent of the baroreflex potentiation did not seem to depend on having originally a more or less powerful baroreflex function. Nitroglycerin Data for nitroglycerin are shown in table 2. In the control period the average value for mean arterial pressure was 106 mm Hg and the RR interval was 802 msec. The fall in pressure induced by nitroglycerin caused a progressives shortening of the RR interval in all subjects. The regression coefficient of RR interval on systolic pressure (i.e., the baroreflex sensitivity) was an average 4.93 (range 1.86-18.20). TABLE 1. Reflex Increase in RR Interval Induced by Increasing Arterial Blood Pressure with Phenylephrine in 18 Subjects Studied Before and After Administration of Digitalis After digitalis Before digitalis Control Control Control Control Regr. coeff. RR MAP Regr. coeff. RR MAP p < r (msec/mm Hg) (mm Hg) (msec) r (msec/mm Hg) (mm Hg) (msec) 976 0.67 5.39 0.01 102 2.67 1 0.72 882 109 0.05 10.49 0.92 810 103 6.93 2 839 0.71 117 94 NS 6.23 0.98 833 3 97 789 0.88 7.15 0.01 16.69 0.84 682 109 4 10.96 0.83 594 113 0.05 7.29 0.91 882 123 6.29 0.91 789 123 5 0.01 7.75 0.92 845 89 3.59 6 0.81 828 96 NS 0.89 10.56 952 136 12.57 0.80 143 870 7 0.01 4.80 106 0.97 857 116 2.71 8 0.95 769 0.02 12.14 0.81 967 148 6.81 0.93 857 151 9 0.01 9.37 0.86 94 983 7.23 0.97 882 10 108 0.05 10.76 0.94 869 103 9.90 11 811 0.98 102 0.05 12.25 0.89 857 101 11.49 12 0.99 113 750 0.05 14.45 0.86 723 108 844 10.63 0.88 97 13 0.05 15.60 0.69 958 111 95 14 12.77 0.86 847 0.01 31.50 1000 0.64 13.40 78 15 79 860 0.84 0.01 3.98 0.85 779 122 2.70 0.86 733 138 16 0.01 0.88 19.90 1276 86 10.60 0.82 1190 89 17 0.01 822 13.70 0.92 18 100 114 6.03 0.89 676 11.83 106 893 823 8.13 0.01 -1.54 -4 ±31 0.90 -4 --28 in RR interval inData are expressed in each subject as linear relationships between rise in systolic pressure and lengthening duced by the injection of phenylephrine, each systolic pressure value being related to the next RR interval value. p refers to the difference between the regression coefficients before and after digitalis, estimated by covariant analysis in individuals and by t test in the group as a whole. Abbreviations: MAP = mean arterial pressure; RR = RR interval; regr. coeff. = regression coefficient. Mean SEM 112 282 CIRCULATION VOL 63, No 2, FEBRUARY 1981 msec mm Hg 1400- 0A after A digitalis r - 0.92 b- 13.7 a = -1464 p < 0.001 A 1200- msec <c0.05 10 I W 1. z a-+100- l mmHg 9z digitalis +100- CL z W a - 1: 100- z b: 6.03 a: -350 p< 0.001 800- X I 100 o- C czmse 4 o before r = 0.89 cc 0z (D z 4x IT CU Q 6 Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 -- 160 200 240 mmHg SYSTOLIC PRESSURE FIGURE 1. Effects of increasing systolic blood pressure by phenylephrine on the RR interval before and after administration of digitalis. The increase in systolic pressure caused a linearly related lengthening ofthe RR interval. The slope of the relationship, i.e., the regression coefficient, is significantly greater after than before digitalis administration. As described in the previous section, administration of digitalis was followed by no change in basal arterial pressure and by an increase in basal RR interval (p < 0.005). There was no significant difference in the rate or magnitude of the fall in blood pressure induced by the same dose of nitroglycerin before and after digitalis. In contrast with the results with phenylephrine, however, the sensitivity of the baroreflex as estimated by nitroglycerin was not affected by PHENYLEPHRINE n= 18 + msec/+ mm Hg n= 7 FIGURE 3. Hemodynamic changes induced by stimulating (upper panel) and deactivating (lower panel) carotid sinus baroreceptors by means of negative and positive neckchamber pressures. Data are average (± sEM) changes from control values in seven subjects who were studied before and after administration of digitalis. C = control values; E = early response; and SS = steady-state responses. Basal mean arterial pressure and basal RR interval were, respectively, 117.2 ± 6.1 mm Hg and 772 ± 29 msec before digitalis and 114.3 ± 5 mm Hg and 833 ± 47 msec after digitalis. The p values refer to differences in the responses before and after digitalis. MAP = mean arterial pressure. digitalis. In six subjects, the regression coefficient was significantly increased, in six it was unchanged and in eight it was significantly reduced. The average value for the regression coefficient obtained with nitro- TRINITROGLYCERINE n= 20 14 T 12- FIGURE 2. Effects of baroreceptor stimulation (phenylephrine) and baroreceptor deactivation (nitroglycerin) on RR interval in the control condition and after digitalis administration. The histograms represent the averages (± SEM) of the regression coefficients of each subject. z W 10- <0 d01 IL LL W 0 86- 0 Vl) (n W 4- it WD cc S'S before digitalis after digitalis - msec/- mmHg 14- U -% 010 - 0 . 1 0 LU - _-4 0 ox X C-) -20- W 1 - .1 z _ <0.05 ''\<005 0.05 2 z 20- 0- control digitalis control digitalis DIGITALIS AND BAROREFLEXES/Ferrari et al. 283 Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 TABLEJ 2. Reflex Reduction in RR Interval by Reducing Arterial Blood Pressure with Nitroglycerin in 20 Subjects During Control and After Administration of Digitalis After digitalis Before digitalis RR MAP RR MAP Regr. coeff. Regr. coeff. r (mm Hg) (msec) r p < (msec/mm Hg) (msec/mm Hg) (mm Hg) (msec) 1 109 0.70 882 1.86 102 NS 967 0.65 1.29 810 2 839 2.30 103 0.97 117 0.97 3.21 0.05 94 3 833 97 789 0.97 4.61 0.96 3.22 0.01 682 4 113 594 0.94 3.55 109 0.96 2.98 0.05 5 101 682 6.36 100 952 0.97 0.83 3.79 0.01 123 789 0.88 2.42 123 882 0.85 6 1.98 0.05 96 7 827 845 0.95 3.03 89 0.89 4.19 0.05 143 136 869 8 0.74 3.15 952 0.96 5.59 0.01 106 116 769 2.84 0.97 857 0.97 9 2.37 NS 94 10 882 108 0.98 3.64 983 0.93 3.87 NS 11 102 810 0.92 103 3.28 869 0.89 3.03 NS 12 113 750 3.58 101 0.96 857 0.94 4.20 0.05 722 13 97 843 0.97 3.17 108 0.98 3.00 NS 111 95 958 12.36 0.05 14 847 0.90 10.32 0.92 1001 15 79 869 0.79 3.92 78 0.92 7.44 0.01 16 72 829 0.97 780 9.77 78 0.75 2.55 0.01 122 732 761 17 138 0.92 3.50 0.88 2.81 0.05 18 121 923 114 0.87 903 5.80 0.98 NS 5.09 92 0.92 19 852 18.20 78 1081 0.92 0.01 5.20 114 20 676 100 0.98 3.30 819 0.97 2.21 0.05 106 Mean 802 101 875 4.93 4.02 NS 3 -SE 018 -22 -3 0.86 -0.54 Data are expressed in each subject as linear relationships between fall in systolic pressure and shortening in RR interval induced by the injection of nitroglycerin, each systolic pressure value being related to the next Rlt interval value. Abbreviations: MAP = mean arterial pressure; RR = RR interval; regr. coeff. = regression coefficient. glycerin was 4.02, which did not differ significantly from the average value before digitalis. Neck Chamber The effects of digitalis on basal blood pressure and basal RR interval were similar to those previously described (no significant pressure change and a significant RR interval -lengthening). In the control condition, reducing the tissue pressure outside the carotid sinuses (i.e., increasing carotid transmural pressure and stimulating carotid sinus baroreceptors) caused a clear-cut reduction in arterial blood pressure (fig. 3), whereas increasing the tissue pressure outside the carotid sinuses (i.e., reducing carotid transmural pressure and deactivating the carotid sinus baroreceptors) caused a clear-cut increase in arterial pressure. The early and the steadystate responses to these maneuvers (see Methods) were similar. After digitalis, the hypotensive responses to carotid baroreceptor stimulation were significantly greater, whereas the pressor responses to carotid baroreceptor deactivation were not significantly altered. The effects of carotid baroreceptor stimulation and deactivation on RR interval are shown in figure 3. Confirming previous findings,"' 12 these responses were modest and variable. On average, RR interval was reduced slightly in response to carotid baroreceptor deactivation, while no significant change was observed when the carotid baroreceptors were stimulated. The only effect of digitalis was on the early response to baroreceptor stimulation, which consisted of a significant increase in RR interval. The bradycardic Discussion response to stimulation of arterial baroreceptors by phenylephrine and the hypotensive response to stimulation of carotid sinus baroreceptors by neck suction were greater after than before injection of 0.8 mg of Lanatoside C, which is within the therapeutic range adopted in man. Therefore, administration of clinical doses of digitalis in man augments the reflex effects of arterial baroreceptor stimulation, and the augmentation is evident with regard both to the heart rate and to the blood pressure. This potentiation may have beneficial effects.'7 For example, enhancement of the inhibitory influence of baroreceptors on the sinoatrial and atrioventricular node'8 may reduce the ventricular rate, 284 CIRCULATION Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 thus improving cardiac filling, stroke volume and coronary flow in conditions such as heart failure and atrial fibrillation if baroreflex potentiation occurs in these pathologic conditions as it does in normal subjects. Our results also show that in man, only one side of the baroreflex is enhanced. When the opposite side of the reflex was studied, i.e., when the baroreceptors were deactivated below the existing level of stimulus by nitroglycerin and positive neck pressure, the reflex tachycardic and pressor responses were not significantly different before and after administration of digitalis. Thus, in man, the augmentation of the arterial baroreceptor function by this drug is limited to the effects of the baroreceptor stimulation and cannot be demonstrated for the effects of a baroreceptor deactivation below the level set tonically by the existing arterial pressure. This indicates a difference with animal studies using large doses of digitalis, in which the hemodynamic responses to deactivation of carotid baroreceptors by common carotid occlusion is also enhanced.3 We do not know why digitalis only potentiates the effects of baroreceptor stimulation and not those of baroreceptor deactivation. However, data from experimental animals suggest at least two explanations. The first is that digitalis stimulates vagal efferent fibers by an action at the central level and possibly at the nerve terminals.'7 The second is that besides augmenting baroreceptor responses to increase in blood pressure (a "sensitization," which may account for the potentiation of the reflex that we observed), digitalis causes a direct pharmacologic stimulation of the receptors independent of any pressure stimulus.2' 1' These factors might oppose the tachycardic and pressor responses either by supporting cardiac vagal influence and by limiting the degree of baroreceptor deactivation that can be obtained by a fall in blood pressure or carotid transmural pressure. Whatever the mechanism involved, that digitalis does not potentiate the response to baroreceptor deactivation may be therapeutically beneficial because excessive tachycardia is avoided during reductions in blood pressure. Several other aspects of our study should be discussed. First, our subjects showed widely different degrees of baroreceptor control of heart rate in the basal condition, consistent with their wide range of age and blood pressure.'4' 20, 21 Yet digitalis enhanced the heart rate response to baroreceptor stimulation to the same degree in the subjects with lesser and in those with greater baroreflex sensitivity. One of the conditions in which the baroreflex has a reduced sensitivity is heart failure,15' 21 which is often preceded and caused by hypertension.22 Therefore, the effect of digitalis on the baroreflex may operate in the clinical conditions in which digitalis is used. Second, we found a lack of correlation between the extent of the bradycardia induced by digitalis and the increase in baroreflex sensitivity caused by the drug. This finding suggests that arterial baroreflex potentiation by digitalis is just one of the many factors responsible for the effect of digitalis on heart rate, the others VOL 63, No 2, FEBRUARY 1981 being the well-known influence of digitalis on cardiovagal centers and vagal nerve terminals'7 and possibly also the effect of this drug on reflexes originating in the heart.23 Third, we noted greater blood pressure responses to carotid baroreceptor stimulation after digitalis. Heart rate effects of baroreceptor manipulation are entirely mediated via the vagus,'Il 24 but blood pressure effects depend mainly on the baroreceptor modulation of noradrenergic sympathetic tone.25 26 Thus, our observations indicate that the baroreflex potentiation caused by digitalis in man is not limited to the cardiovagal component of the reflex, but involves its sym- pathetic efferent pathways. Acknowledgment We thank Paola Boccaccini for typing the manuscript, Riccardo Sarri for photography and Carla Zanchetti for preparing illustrations. References 1. McLain PL: Effects of ouabain on spontaneous afferent activity in the aortic and carotid sinus nerves of cats. Neuropharmacol 9: 399, 1970 2. Quest JA, Gillis RA: Effect of digitalis on carotid sinus baroreceptor activity. Circ Res 35: 247, 1974 3. Quest JA, Gillis RA: Carotid sinus reflex changes produced by digitalis. J Pharmacol Exp Ther 177: 650, 1971 4. Reing CM, Thibodeaux H, Gillis RA, Kot PA: Influence of baroreceptor reflexes on cardiovascular responses of the dog to acetylstrophantidin. J Pharmacol Exp Ther 184: 641, 1973 5. McRitchie RJ, Vatner SF: The role of arterial baroreceptors in mediating the cardiovascular response to a cardiac glycoside in conscious dogs. Circ Res 38: 321, 1976 6. Cokkinos DV, Haralambakis G, Thalassinos C, Heimanas ET, Demopoulos J, Voridis N, Gardikas C: Effect of digitalis on diminished baroreceptor sensitivity in diabetics. Angiology 30: 549, 1979 7. Thompson MA, Eckberg DL: Effects of ouabain upon the carotid baroreceptor reflex in normal man. (abstr) Circulation 54 (suppl II): 11-224, 1976 8. Smith HS, Sleight P, Pickering GW: The reflex regulation of arterial pressure during sleep in man: a quantitative method of assessing baroreflex sensitivity. Circ Res 24: 109, 1969 9. Pickering TG, Gribbin B, Sleight P: Comparison of reflex heart rate response to rising and falling arterial pressure in man. Cardiovasc Res 6: 277, 1972 10. Ludbrook J, Mancia G, Ferrari A, Zanchetti A: The variablepressure neck-chamber method for studying the carotid baroreflex in man. Clin Sci Mol Med 53: 165, 1977 11. Mancia G, Ferrari A, Gregorini L, Valentini R, Ludbrook J, Zanchetti A: Circulatory reflexes from carotid and extracarotid baroreceptor areas in man. Circ Res 41: 309, 1977 12. Mancia G, Ludbrook J, Ferrari A, Gregorini L, Zanchetti A: Baroreceptor reflexes in human hypertension. Circ Res 43: 170, 1978 13. Moe GK, Farah AE: Digitalis and allied cardiac glycosides. In The Pharmacological Basis of Therapeutics, edited by Goodman LS, Gilman A. New York, MacMillan, 1974, p 653 14. Gribbin B, Pickering TG, Sleight P, Peto R: Effect of age and high blood pressure on baroreflex sensitivity in man. Circ Res 29: 424, 1971 15. Higgins CB, Vatner JF, Eckberg DL, Braunwald E: Alteration in the baroreceptor reflex in conscious dogs with heart failure. J Clin Invest 51: 715, 1972 16. Snedecor GW, Cochran WG: Statistical Methods. Ames, Iowa, Iowa University Press, 1967 17. Gillis RA, Pearle DL, Levitt 0: Digitalis: a neuroexcitatory drug. Circulation 52: 739, 1975 18. Mancia G, Bonazzi 0, Pozzoni L, Ferrari A, Gregorini L, CORONARY SCORE AND CAD/Leaman et al. 19. 20. 21. 22. Perondi R: Baroreceptor control of atrioventricular conduction in man. Circ Res 44: 752, 1979 Saum WR, Brown AM, Tuley FM: An electrogenic sodium pump and baroreceptor function in normotensive and spontaneously hypertensive rats. Circ Res 39: 497, 1976 Bristow JD, Honour AS, Pickering GW, Sleight P, Smyth HS: Diminished baroreflex sensitivity in high blood pressure. Circulation 39: 48, 1969 Eckberg DL, Drabinsky M, Braunwald E: Defective parasympathetic control in patients with heart disease. N Engl J Med 285: 87, 1971 Kannel WB: Importance of hypertension as a major risk factor in cardiovascular disease. In Hypertension, edited by Genest J, 285 Koiw E, Kuchel 0. New York, McGraw-Hill, 1977, p 888 23. Thames MD: Acetylstrophantidin-induced reflex inhibition of canine renal sympathetic nerve activity mediated by cardiac receptors with vagal afferents. Circ Res 44: 8, 1979 24. Eckberg DL, Abboud FM, Mark AL: Modulation of carotid baroreflex responsiveness in man: effects of posture and propranolol. J Appl Physiol 41: 383, 1976 25. Mancia G, Ferrari A, Gregorini L, Parati G, Ferrari MC, Pomidossi G, Zanchetti A: Control of blood pressure by carotid sinus baroreceptors in human beings. Am J Cardiol 44: 895, 1979 26. Kirchheim H R: Systemic arterial baroreceptor reflexes. Physiol Rev 56: 100, 1976 Coronary Artery Atherosclerosis: Severity of the Disease, Severity of Angina Pectoris and Compromised Left Ventricular Function Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 DAVID M. LEAMAN, M.D., RONALD W. BROWER, PH.D., GEERT T. MEESTER, M.D., PATRICK SERRUYS, M.D., AND MARCEL VAN DEN BRAND, M.D. SUMMARY To determine if the severity of angina pectoris and the degree of altered left ventricular function correlated with the severity and extent of the underlying coronary artery disease, a coronary scoring system was derived. The system was based on the severity of luminal diameter narrowing and weighted according to the usual flow to the left ventricle in each coronary vessel. Thus, the most weight was given to the left main coronary artery, followed by the left anterior descending, circumflex, and right coronary arteries. The resultant number was an indicator of the overall severity of the obstructive coronary artery disease. A coronary arterial system with no obstructive disease was scored as zero and the greater the degree of obstructive disease coronary present, the higher the coronary score. From 202 subjects, four groups were evaluated: group 1 coronary score = 17.5score = 0.5-4.5 (n = 10); group 2- coronary score = 10.5-12.5 (n = 11); group 3 20.5 (n = 11); and group 4 coronary score = 25.0-36.0 (n = 11). All subjects had coronary artery bypass surgery and had preoperative and l-year postoperative cardiac catheterization, including atrial pacing to maximal heart rate. The groups could not be separated on the basis of angina frequency, resting heart rate, cardiac index, left ventricular end-diastolic pressure, peak paced left ventricular end-diastolic pressure, dP/dt, V max, left ventricular end-diastolic volume index, left ventricular end-systolic volume index, stroke volume index, ejection fraction or mean circumferential fiber shortening velocity. Thus, based on this study, the severity of coronary artery disease does not statistically correlate with the frequency of angina pectoris or produce a predictable degree of altered left ventricular function. The frequency of angina pectoris cannot be used to predict prognosis or the adequacy of myocardial revascularization. - IF THE SEVERITY of angina pectoris correlated with the severity of the underlying coronary artery atherosclerosis, one could better judge the appropriate time for invasive diagnostic and therapeutic interventions. One could also ascertain the prognosis of the disease, as it has been adequately shown that prognosis is in part dependent on the severity of coroFrom the Erasmus University, Thoraxcentrum, The Interuniversity Cardiology Institute, Rotterdam, The Netherlands, and the Department of Cardiology, The Milton S. Hershey Medical Center of the Pennsylvania State University, Hershey, Pennsylvania. Address for correspondence: David M. Leaman, M.D., Department of Medicine, Division of Cardiology, The Hershey Medical Center, Hershey, Pennsylvania 17033. Received August 21, 1979; revision accepted June 26, 1980. Circulation 63, No. 2, 1981. nary artery disease (CAD).1-10 It would also be helpful if the severity of the CAD correlated with the degree of abnormal left ventricular function. This would be especially helpful in the postoperative state, when one could very simply ascertain the adequacy of the operation and judge the state of left ventricular function. To evaluate these possibilities, a coronary score was derived to assess the degree of CAD. The coronary score was then related to the frequency of angina pectoris to determine if the extent of CAD could be predicted based on the clinical presentation of angina pectoris. It was also compared with resting and paced left ventricular function measurements to determine if the severity of CAD had a predictably deleterious effect on left ventricular function. The coronary score was also determined at 1 year after coronary bypass surgery and was again compared with the frequency of Digitalis and baroreceptor reflexes in man. A Ferrari, L Gregorini, M C Ferrari, L Preti and G Mancia Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 Circulation. 1981;63:279-285 doi: 10.1161/01.CIR.63.2.279 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1981 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/63/2/279 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/