Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
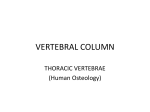
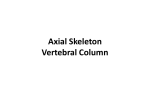
Low Back Pain What’s that? The Problem – 93 million work days lost annually for LBP. – Cost of Tx for LBP is greater than Heart Disease or Traffic Accidents. – 2nd most common reason for seeking medical care. – 91% seeking Chiropractic care…did so for low back pain Facet Syndrome – Who? • Chiropractic use by Seniors: • “Those over 65 constitutes between 12 – 17 % of the average Chiropractic practice.” » Coulter et al. Chiropractic patients in a comprehensive home based geriatric assessment, follow up and health promotion program. Top Clinical Chiropractor 1996; 3(2): 46-55. Facet Syndrome – Who? • Chiropractic Care and management of the Geriatric patient… – U.S. Department of Commerce: • 1994 – 33 million over 65 ( 1 in 8 ) • 2000 – 13 % of the population over 65 • By 2030 – 20% of the population over 65, and care for older patients will represent half of all healthcare dollars • 2050 (This means you!!!) – 80 million over the age of 65 (1 in 5) Facet Syndrome - Process – Degenerative Disc Disease and Disc Herniation…Physiological changes in the intervertebral disc, beginning in the second decade, progress throughout life with degenerative changes resulting. – As the nucleus pulposis and annulus fibrosis degenerate, a bulging, herniation of the nucleus, or even nuclear extrusion may occur…Thus, the beginnings of LBP!!! Facets - Normal – Superimposed loads on the lumbar spine are borne by the body-disc-body anteriorly and by the two articular facets posteriorly…ligaments provide stability for the posterior elements and the intervertebral disc. Facets - Normal • The apophyseal joints are not loaded heavily by compression (borne by the disc) or flexion-extension…but can be heavily loaded by A to P / P to A shear loads. • The lumbar apophyseal joints function to allow limited movement between vertebrae and to protect the discs from shear forces, excessive flexion, and axial rotation. Not designed to resist compression…that’s the job of the disc. Facets - Normal – Morris states that 70 % of the superimposed body weight is carried on the vertebral bodies and 30 % on the articular facets. Morris JM, Lucas DB, Bresler B: Role of trunk in stability of the spine. J Bone Joint Surgery 43A: 327, 1961 Facet Loading • Panjabi presents the following algorithm of the stages of injury to the F.S.U.: • 1. Asymmetric disc injury at one F.S.U. level • 2. Disturbed kinematics of F.S.U.’s above and below • 3. Asymmetric movements at facet joints • 4. Unequal sharing of facet loads • 5. High load on one facet joint resulting in intraarticular cartilage degeneration, joint space narrowing, and facet atrophy. Facet Syndrome – It is obvious that weight distribution on the facets change with degenerative disc disease, in which narrowing of the disc places disproportionately more weight on the articular facets…as high as 47% to 70% Facets – With Disc thinning…an individual has an increased articular weight bearing. This contact between the facet tip and lamina is labeled in Chiropractic as a Facet - lamina syndrome. Facet Lamina Syndrome – Thus causing an abnormally high impingement of the facet tips on the adjacent lamina or pedicle, and the apophyseal joints show gross osteoarthritic changes. • It is possible that the joint capsule is nipped by such high stress placed on the tips of the articular facets…meniscoids!!! Facets - Normal – The mean articular facet area increases suddenly at L4 & L5 as compared to the upper lumbar levels, indicating that there is more compressive force at the articular facets in the lower than in the upper lumbar spine. – T5 – L4…increase vertebral body size Normal - R.O.M. – 75% to 80% of all flexion / extension occur at L5 / S1 region. – 20% occurs at L4 / L5 – 5% occurs at the remaining upper levels…L3 and above. L5 / S1 • Remember, the joint between L5 & S1 is the single most common site for problems in the vertebral column…Because of the following: • The joint bears more weight than any other vertebral joint. • Center of gravity passes directly through these two segments. • Transition site between mobile segment and relatively stable pelvic girdle. • Increased angle between L5 & Sacrum. Facets – The increased transfer of weight through the pedicles at L5, which is an area of forward and downward inclination of forces as L5 sits on the sacrum at an inclined plane, has been offered as an explanation for the stress leading to fracture of the Pars interarticularis and resultant spondylolisthesis. • Normal sacral angle & inclination…41° & 46 ° respectively. Analysis…Facet Syndrome? • Check facet imbrication & Stenosis…X-ray assessment. • Check Disc angle…15° or More? • Check X, Y & Z; Psoas; piriformis; Q.L.; anterior-ilio femoral ligament; etc. • Check A.P.I. • Female 5 to 10 degrees…normal • Male 0 to 5 degrees…normal Radiographic assessment Facet imbircation (Radiographic Assessment) • Check for unequal weight distribution via X-rays: • • • • Hadley’s “S” curve Macnab lines Lumbsacral angle Van Akkerveeken lines Facet imbircation (Radiographic Assessment) • Hadley’s “S” curve : – Views: Oblique & A - P Lumbar spine – A curvilinear line is constructed along the inferior margin of the TVP and down along the inferior articular process to the apophyseal joint space. The line is then continued across the articulation to connect with the outer edge of the opposing superior articular process. – The resultant configuration of this line will be that simulating the letter “S”. The key region of the “S” to observe is normally a smooth transition across the joint space. – Significance: An abrupt interruption in the smooth contour of this line signifies facet imbrication. – Yochum and Rowe…pg. 192 Facet imbircation (Radiographic Assessment) • Macnab’s line: – View: Lateral lumbar – A line is drawn through and parallel to the inferior end plate at the level to be evaluated. The relationship of the adjacent tip of the superior articular process of the vertebra below is then assessed. » Significance: If the line intersects the superior articulating process, facet imbrication may be present…thus effecting the size of the IVF…Stenosis!!! » Combine Lumbosacral Disc Angle. Facet imbircation (Radiographic Assessment) • Lumbosacral Disc Angle: (Combined with Macnab’s line for possible vertical stenosis of L5/S1 IVF) • View: Lateral lumbar – A line is drawn parallel and through the inferior end plate of the 5th lumbar (Macnab’s line) and superior endplate of the 1st sacral segment. The angle formed by these lines is then measured. » An increase in the lumbosacral disc angle more than 15° has been linked with the presence of low back pain due to facet imbrication. » The greater the disc angle…the more severe the facet syndrome…Cox pg. 447 » Y & R…pg. 189 Facet imbircation (Radiographic Assessment) • Van Akkerveeken’s measurement: – View: Lateral lumbar spine – Two lines are drawn through and parallel to opposing segmental endplates until they intersect posteriorly. The distance from the posterior body margins to the point of intersection in then measured. Alternatively the displacement can be assessed by measuring the offset in the opposing body corners. – Significance: A difference of 1.5 mm to 3.0 mm in measurement shows a greater chance of nuclear, annular, and posterior ligament damage at the displaced segment….Instability. – Measure the disc angle. – Yochum & Rowe…pg. 192 Overview - Review – 70% / 30%...normal weight bearing. Disc degeneration…Increase facet weight bearing to 47% to 70% – Facet – lamina syndrome…with disc thinning – Normal facets…increase in size @ L4 / L5 region – Normal Vertebral bodies increase in size from T5 to L4…L5 V.B. decreases. L5 increased angle…Normal sacral angle & inclination…41° & 46 ° respectively. – Check X,Y, & Z; A.P.I.; Facet imbrication; stenosis; etc… – Radiographic Assessments…Hadley’s “S” curve; Mcnab’s line; Lumbosacral angle; Van akkerveeken’s line. Normal Anatomy – Canal at L5 – S1 is the smallest, yet the DRG there is the largest in the lumbar spine. – R.O.M. – 75% of Flexion / Extension…occurs at L5 – S1 – Center of gravity passes through L5 – S1. – Transition point between the stable pelvic girdle and the mobile lumbar vertebrae. – Facets at L5 – S1 are usually at a 45 degree angle. Diff / DX – Sclerotome…one of the paired masses of mesenchymal tissue, separated from the ventromedial part of a somite, which develop into vertebrae and ribs. – Radiculopathy…disease of the nerve roots. Diff / DX • Sclerotogenous pain • • • • Pain above the knee. Diffuse LBP No motor, No reflex, No dermatomal involement Multiple causes Facet Pain / Patterns – T12 – L3: Facet Pain distribution – No leg or coccygeal pain. Radiating pain to thoracic and cervical spines – L3 – L4: F.P.D. – Upward to thoracic spine, diffuse flank and groin pain & Coccyx – L4 – L5: F.P.D. – Posterior hip and thigh & Coccyx. – L5 – S1: F. P. D. – Coccyx; Hip; Posterior thigh; Groin; Flank. – Lora J, Long D: So – called facet denervation in the management of intractable back pain. Spine 1 (2): 121 – 126, 1976 Diff / DX • Radiculopathy • Contained • Non – Contained • Motor, Reflex, and Dermatomal involvement. Sciatica • 5 common causes: 1. 2. 3. 4. 5. Herniated disc Annular tears…chemical leakage Myogenic Spinal stenosis Facet joint arthropathy Herniated Disc • Herniated nucleus pulposus: • • • • History of specific trauma Leg pain greater than back pain Neurologic deficit present Pain increases with sitting and leaning forward, coughing, sneezing, and straining • Radiologic evidence of nerve root compression Facet Syndrome • Panjabi presents the following algorithm of the stages of injury to the F.S.U. • • • • • 1. Asymmetric disc injury at one F.S.U. level 2. Disturbed kinematics of F.S.U.’s above and below 3. Asymmetric movements at facet joints 4. Unequal sharing of facet loads 5. High load on one facet joint resulting in intraarticular cartilage degeneration, joint space narrowing, and facet atrophy. Facet Syndrome • “Facet fixations may set off a chain of events leading to asymmetrical loading on the epiphyseal plates and to muscle and ligamentous imbalance, ultimately resulting in curve progression”. • – Panjabi & White: Clinical Biomechanics of the spine. Facet Pain • Stretching of the joint capsule may be a source of pain due to the presence of a nociceptive type IV receptor system. • Joint receptors (Type I, II, & III mechanoreceptors) provide information regarding such activities as the direction, velocity, and initiation of joint movements— achieved by responding to tension applied to the connective tissue surrounding them. • Type IV joint mechanoreceptor is unmyelinated, free nerve endings and responds to potentially injurious mechanical or inflammatory processes. Facet Pain – Wyke points out that the apophyseal capsule contains unmyelinated nerve fibers. They are sensitive to both chemical and mechanical irritation, and high tensions develop in the facets following disc degeneration and the carrying of more weight. Facet Pain – – – – Wyke states that the cause of low back pain is irritation of nociceptors. The term Nociceptive means “sensitive to tissue abnormality.” Two abnormalities causing pain are mechanical and chemical. There are three morphological types of nociceptors 1. Unmyelinated fibers in interstitial tissues 2. Free naked nerve endings 3. Unmyelinated paravascular nociceptive system in the adventitial layers of blood vessels. Facet Pain – Histological studies of sectioned “Z” joints indicates the presence of an extensive vascular supply. Since Vascular structures may be related to pain, this may help explain spinal pain of “Z” origin. Facet Pain – This sensory nerve supply is sufficiently developed to support the hypothesis that irritation of the capsule of the lumbar articular facets could well produce pain stimuli. – Which could return to the CNS through the posterior primary division and produce referred pain through the dermatomes of the involved nerves. Facet Pain • The capsule of the articular facets are richly innervated with sensory fibers, according to Von Luschka. The posterior primary division of the spinal nerve (dorsal ramus) and the recurrent nerve of the anterior primary division innervate the capsule. Which correspond exactly with the pathways of Sciatic radiation…namely the 4th and 5th nerves. Facet Pain / Patterns • Lora and Long stimulated the facets…in and around the facets. – Typical radicular radiation is not generated by stimulation of the nerves in and around the facet, but widespread referral of sensation even into the leg is possible: – This referral of sensation is difficult for the patient to localize, and has not gone below the knee in any patient. Facet Pain / Patterns • Referred pain shares the same distribution as the innervation of the affected Zygapophyseal articulations. • Pain arising from the L4 – L5 and L5 – S1 articulations will be felt in the posterior thigh, and occasionally in the medial and lateral calf, and back pain is usually greater than leg pain. – The pain, occasionally, but rarely, extends beyond the calf and into the foot. Facet Pain / Patterns • Schofferman and Zucherman feel that leg pain may prove more useful diagnostically. – The distribution and quality of the pain are used to separate referred pain from radicular pain. Pain in the absence of neurological deficit is referred pain, while pain in the presence of neurological change is radicular. – Schofferman J, Zucherman J: History and physical examination. Spine: State of the Art reviews 1 (1): 14, 1986. Facet Treatment • The major benefits of flexion manipulation: • Improvement of transport of metabolites into the intervertebral discs, reduction of stress on the apophyseal joints and on the posterior half of the annulus fibrosus, and giving the spine a high compressive strength. Manipulation • Benefits of Manipulation • Increase Spinal range of motion • Relieve nociceptor irritation • Equalize the weight distribution…Thus, relieving the compressive forces against the nerve root in the vertebral canal & the I.V.F. Facet Treatment • Test the pt.’s tolerance prior to any manipulative maneuver. A side lying maneuver to treat facet subluxation syndrome when the patient is in too much pain to lie prone. • Place the Iliac crest in the middle of the abdominal piece. • Start the table at ½ speed to check pt.’s tolerance…do not continue if pt. experiences an increase in pain. • Treat pt. in side lying position…Lateral flex the table (knees bent), and pump the vertebra above the lesion. Facet Syndrome • Ghormley stated: “There is ample evidence to regard facets as a cause of sciatic pain. He used the term facet syndrome to describe the sudden onset of low back pain brought on by some activity usually involving a twisting or rotatory strain of the lumbosacral region” • Ghormley RK: JAMA 101: 1773-1777, 1933.