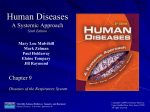
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Human Diseases A Systemic Approach Sixth Edition Mary Lou Mulvihill Mark Zelman Paul Holdaway Elaine Tompary Jill Raymond Chapter 13 Diseases of the Endocrine System Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Chapter 13 Diseases of the Endocrine System Multimedia Asset Directory Slide 5 Slide 89 Slide 90 The Endocrine System Diabetes Diabetes (continued) Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Functions of the Endocrine Glands Secrete hormones Major organs – Hypothalamus – Pituitary gland – Thyroid gland – Parathyroid glands – Pancreatic islets – Adrenal glands – Testes and ovaries Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Anatomy and Physiology of the Endocrine System The endocrine system is a collection of glands that secrete hormones into the bloodstream. Hormones are chemicals that act on target organs to increase or decrease the target’s activity level. The endocrine system is instrumental in maintaining homeostasis. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Click on the screenshot to view an animation showing the endocrine system. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Return to Directory Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Figure 13-1: The endocrine glands. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Types of Glands Two types of glands in Endocrine glands, on the the body: exocrine glands and endocrine glands. Exocrine glands release their secretions into a duct that carries them to the outside of the body. Example: sweat glands other hand, release hormones directly into the bloodstream. Since they have no ducts, they are referred to as ductless glands. Example: thyroid gland Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Glands of the Endocrine System 2 adrenal glands 4 parathyroid glands Pancreas Pineal gland Pituitary gland 2 ovaries in the female 2 testes in the male Thymus gland Thyroid gland Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Figure 13-2: The pituitary gland and its relation to the brain. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Figure 13-3: Anterior pituitary gland and its target organs. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Physiology of the Endocrine Glands Hormones are released from endocrine glands into the bloodstream, where they affect activity in cells at distant sites. – Some hormones affect the whole body whereas others act only on target organs. Most hormones are composed of proteins or chains of amino acids; others are steroids or fatty substances derived from cholesterol. The pituitary gland, which is sometimes called the master gland, is controlled by the hypothalamus. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Physiology of the Endocrine Glands (continued) The body is conservative and secretes hormones only as needed. – Control via negative feedback Overactivity = hyperactive gland – Gland secretes an excessive amount of its hormone – May be caused by a hypertrophied gland or by a glandular tumor. Underactivity = hypoactive – A gland that fails to secrete its hormone or secretes an inadequate amount – May be caused by disease or tumor, or it may be caused by trauma, surgery, or radiation Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. The Pituitary Gland Located on the underneath side of the brain. Small pea-sized gland is divided into an anterior lobe and a posterior lobe. Both lobes are controlled by the hypothalamus in the brain. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. The Anterior Pituitary Secretes seven hormones: Growth hormone (GH), also Follicle-stimulating hormone called somatotropin, promotes growth of the body by stimulating cells to rapidly increase in size and divide. Thyroid-stimulating hormone (TSH) regulates the function of the thyroid gland. Adrenocorticotropin hormone (ACTH) regulates the function of the adrenal cortex. Prolactin (PRL) stimulates milk production in the breast following pregnancy and birth. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e (FSH) responsible for the development of ova in ovaries and sperm in testes; also stimulates the ovary to secrete estrogen. Luteinizing hormone (LH) stimulates secretion of sex hormones in both males and females and plays a role in releasing ova in females. Melanocyte-stimulating hormone (MSH) stimulates melanocytes to produce more melanin, darkening the skin. Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. The Posterior Pituitary Secretes two hormones: Antidiuretic hormone (ADH), also called vasopressin, promotes water reabsorption by the kidney tubules. Oxytocin stimulates uterine contractions during labor and delivery, and after birth the release of milk from the mammary glands. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. The Structure and Function of the Pituitary Gland Hypophysis: has two parts Anterior = adenohypophysis – Activity directed by the hypothalamus – Secretes six tropic hormones – Regulates the adrenal gland Posterior = neurohypophysis – Receives hormones secreted by the hypothalamus and then stores them for subsequent release Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Diseases of the Anterior Pituitary Hyperpituitarism – Giantism – Acromegaly Hypopituitarism – Absence of tropic hormones – Pituitary dwarf Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Hyperpituitarism – Anterior Pituitary Giantism: hypersecretion of growth hormone prior to puberty – Retards normal closure of bone seal – Decreased sexual development – Mental development normal or retarded Etiology: adenoma Treatment: removal of adenoma or radiation to reduce the size of the tumor Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Hyperpituitarism – Anterior Pituitary Acromegaly – Hypersecretion of growth hormone after puberty – Long bones no longer grow – Excessive growth of soft tissue – Enlargement of the face with coarse facial features – Protrusion of the tongue – Curvature of the spine Etiology: adenoma Treatment: surgical removal, radiation, supportive treatments Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Hypopituitarism – Pituitary Etiology – Damage to the anterior lobe of the pituitary gland – Fracture at the base of the skull, tumor, ischemia – Inadequate secretion of hormones Mild or severe Panhypopituitarism: entire anterior lobe is destroyed – No pituitary hormones are secreted Pituitary dwarf Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Figure 13-4: Effects of pituitary failure. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Abnormalities – Absence of Tropic Hormones Lack of thyroid hormone: lethargy Lack of ACTH: salt imbalance, improper metabolism of nutrients – ACTH essential for life Absence of gonadotropic hormones – Depresses sexual function – Before puberty – impaired sexual development – After puberty – Cessation of menstruation – Aspermia in males Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Pituitary Dwarf May occur in children – Inadequate growth hormone – Mentally bright but small and underdeveloped sexually – All growth processes are retarded; teeth are late in erupting. – Replacement therapy with injections of growth hormone is currently used to treat children with pituitary dwarfism. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Hypopituitarism – Treatment Hormonal supplements – Thyroxine, cortisone, growth hormone, and sex hormones can compensate for the dysfunctional glands. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Function of the Posterior Pituitary Gland Posterior pituitary, or neurohypophysis – Secretes oxytocin, and vasopressin (ADH) Oxytocin: causes smooth muscle contraction of the uterine muscles ADH: prevents excessive water loss through the kidneys Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Hyposecretion of the Posterior Pituitary Gland Diabetes insipidus – Deficiency of ADH – In the absence of ADH, water is not reabsorbed by the kidney and is lost in the urine. Extreme thirst or polydipsia and excessive production of diluted urine or polyuria results. A central diabetes insipidus can result from inadequate production of ADH by the hypothalamus or failure of the pituitary gland to release ADH into the bloodstream. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Hyposecretion of the Posterior Pituitary Gland (continued) Nephrogenic diabetes insipidus: ADH levels are normal – Involves a defect in the kidney; the kidney fails to concentrate urine in response to the instructions of ADH. Excessive water loss can quickly lead to dehydration. Treatment: the underlying cause of diabetes insipidus must be corrected. Modified forms of ADH may be taken orally, by injection, or by nasal spray to maintain normal urine output. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Figure 13-6: Normal action of antidiuretic hormone (ADH). Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Figure 13-7: Effect of antidiuretic hormone (ADH) deficiency. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. The Thyroid Gland Resembles a butterfly Produces the in shape; has right and left lobes Located on either side of the trachea and larynx Thyroid cartilage, or Adam’s apple, is located just below the thyroid gland hormones thyroxine, also known as T4, and triiodothyronine, which is called T3 These are produced in the thyroid gland from the mineral iodine. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Structure and Function of the Thyroid Gland Regulates metabolic rate Secretes thyroxine, governs cellular oxygen consumption, and thus, energy and heat production; the more oxygen that is used, the more calories are metabolized (“burned up”). Thyroxine assures that enough body heat is produced to maintain normal temperature even in a cold environment. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Structure and Function of the Thyroid Gland (continued) Structure of the thyroid gland – Located in the neck region, one lobe on either side of the trachea; a connecting strip, or isthmus, anterior to the trachea, connects the two lobes – Just below the Adam’s apple, the protrusion formed by part of the larynx – The thyroid gland consists of follicles, microscopic sacs. Within these protein-containing follicles, the thyroid hormones, thyroxine and triiodothyronine, are made. Thin-walled capillaries run between the follicles in a position ideal to receive the thyroid hormones. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. The Thyroid Gland Also secretes calcitonin in response to hypercalcemia (too high blood calcium level). Its action is the opposite of parathyroid hormone and stimulates the increased deposition of calcium into bone, thereby lowering blood levels of calcium. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Figure 13-8: The thyroid gland. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Function of the Thyroid Gland The thyroid gland synthesizes, stores, and releases thyroid hormones, which contain iodine. – Most of the iodide ions of the body are taken into the thyroid gland by a mechanism called the iodide trap. – Iodine combines with an amino acid; two of these groups join, and the thyroid hormones are formed. The hormones are stored until needed and then released into the blood capillaries. In the blood, the thyroid hormones combine with plasma proteins. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Effects of Thyroid Hormones Thyroxine: secreted in the largest quantity. – Thyroxine stimulates cellular metabolism by increasing the rate of oxygen use with subsequent energy and heat production. – Nutrients are converted to energy in the presence of oxygen and the waste products of metabolism, including carbon dioxide, are formed. – As cellular metabolism increases, respiration and cardiac output increases. – Heat is produced through cellular metabolism – Increases secretion of digestive enzymes and movement through the digestive system. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Figure 13-9: Effects of thyroxine. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Control of Circulating Thyroxine Level Anterior pituitary gland stimulates the thyroid by releasing thyroid-stimulating hormone, TSH. The thyroid, in turn, releases thyroxine, which circulates in the blood to all cells and tissues. When the level of circulating thyroxine is high, the anterior pituitary is inhibited and stops releasing TSH (negative feedback mechanism). – An adequate level of thyroxine prevents further synthesis of the hormone. When the level of thyroxine falls, the anterior pituitary is released from the inhibition, and once again sends out TSH. This feedback mechanism is shown in Figure 13.10. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Figure 13-10: Control of thyroxine secretion through negative feedback. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Histology of normal thyroid gland showing follicles containing thyroglobin. (© M. Peres / Custom Medical Stock Photo.) Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Nodular goiter. Note the distorted follicles. (© O.J. Staats / Custom Medical Stock Photo.) Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Negative Feedback Failure Constitutes one basis for a thyroid disease The thyroid gland may be perfectly healthy, but if the body’s iodine supply is inadequate, the gland cannot produce thyroxine. It is possible for the thyroid gland to be overstimulated or understimulated by the anterior pituitary. The thyroid gland itself may be diseased, with a resultant hyperactivity or hypoactivity. These are some of the conditions that will be discussed. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Goiter An enlargement of the thyroid gland. May be caused by hypoactivity or hyperactivity of the thyroid or a deficiency in iodine needed to synthesize thyroid hormones Types: diffuse colloidal goiter or nontoxic goiter Endemic goiter because it is common in a particular geographic region – The usual cause of an endemic goiter is insufficient iodine in the diet. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Goiter (continued) Etiology of goiter – Continuous secretion of thyroid-stimulating hormone causes the thyroid gland to enlarge as a compensatory mechanism. – An enlargement of the neck is generally the only symptom. Usually enough thyroxine is produced to prevent the symptoms of hypothyroidism. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Goiter (continued) Treatment: iodides: the use of iodized salt prevents endemic goiter formation. If the goiter is very advanced, surgery may be necessary. A very large goiter puts pressure on the esophagus, causing difficulty in swallowing, or presses on the trachea, causing a cough or choking sensation. Other factors can cause a simple diffuse colloidal goiter; for example, a defect in the thyroxine-synthesizing mechanism. A young girl entering adolescence may develop this type of goiter because of an increased need for thyroxine at this time. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Adenomatous or Nodular Goiter Secrete an excessive amount of thyroxine, a condition of hyperthyroidism Symptoms: nervousness and tremors, a shakiness, particularly in the hands: metabolism increases, causing sweating and a rapid pulse; a nodule or adenoma may put pressure on the trachea or esophagus. Treatment: Surgery is sometimes necessary to remove part of the thyroid gland, but medication is often effective in preventing further enlargement. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Graves’ Disease Goiter develops; the entire gland hypertrophies, and there are no nodules Severe hyperthyroidism More common in women than in men and usually affects young women Characteristic facial expression is strained and tense, and there is a stare in the eyes. The eyeballs protrude outward, a condition called exophthalmos. This is caused by edema in the tissue behind the eyes. The bulging of the eyes can be so severe that the eyelids do not close, and the swelling sometimes damages the optic nerve. This symptom generally persists even when the hyperthyroidism is corrected. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Graves’ Disease (continued) The person has a tremendous appetite but loses weight to the point of appearing emaciated, as calories are burned up at a rapid rate. Thyroxine speeds the passage of food through the digestive tract. There is no time for the normal reabsorption of water from the large intestine, so diarrhea frequently accompanies the disease. Tachycardia, rapid pulse rate, and palpitation are also among the symptoms. The person is extremely nervous, excitable, and is always tired but has difficulty sleeping because of the hyperactivity of the body. The high metabolic rate causes excessive heat production, which results in profuse perspiration. The skin is always moist, and an insatiable thirst follows the loss of water. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Signs and Symptoms of Graves’ Disease Exophthalmos Profuse perspiration Hand tremors Goiter Weight loss Nervousness/excitability Rapid pulse Polydipsia Diarrhea Tachypnea Insomnia Graves’ disease is an autoimmune condition in which antibodies to a thyroid antigen stimulate hyperactivity of the thyroid gland. This causes the thyroid to produce too much thyroxine. Graves’ disease can sometimes be treated with medication that inhibits the synthesis of thyroxine, or by administration of radioactive iodine, which destroys the thyroid gland. Removal of the thyroid gland, however, may be necessary. If the gland is removed, hormonal supplements must be given. Partial removal of the thyroid gland allows the remaining portion to secrete hormones. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Hypothyroidism Myxedema severe hypothyroidism, an inadequate level of thyroxine Symptoms: bloated appearance, thick tongue, puffy eyelids, dry scaly skin, little perspiration, muscular weakness and somnolence, excessive sleepiness, sluggish mental and physical processes, slurred speech, slow reflexes, decreased heart rate, slowed circulation, edema to develop. Lack of thyroxine increases the amount of circulating lipids, which leads to the development of atherosclerosis. The digestive system works sluggishly, so the patient suffers from constipation. Weight gain also accompanies the disease. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Myxedema Affects women more than men, and usually affects women of middle age. Etiology: Radiation damage to the thyroid gland or develops after thyroid surgery if thyroxine is not administered Primary disease of the thyroid gland or secondary to pituitary disease. – If the pituitary gland does not secrete thyroid-stimulating hormones, the thyroid gland ceases to function. Myxedema is treated by administering thyroxine. The condition generally responds well to treatment, and the symptoms disappear. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Cretinism Congenital thyroid deficiency in which thyroxine is not synthesized; thyroxine is essential to both physical and mental development. Mental retardation and an abnormal, dwarfed stature Etiology: error in fetal development if the thyroid gland fails to form or is nonfunctional, or may be endemic where the mother suffers from an inadequate iodine supply The cretin is a dwarf with a stocky stature and a characteristically protruding abdomen. The sexual organs do not develop, and the face of the cretin is typically misshapen: a broad, sunken nose, small eyes set far apart, puffy eyelids, and a short forehead. A thick tongue protrudes from a wide-open mouth, and the face is expressionless. The earlier this condition is diagnosed and treated with thyroxine, the more optimistic is the prognosis. Lifelong hormonal therapy will be required. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Diagnostic Test Activity of the Thyroid Gland Tests to determine the activity of the thyroid gland are based on this combination of triiodothyronine (T3) and thyroxine (T4) with plasma proteins. Serum is incubated with radioactive thyroid hormones and resin. – The resin absorbs the hormones that are not bound to the blood proteins. – Radioactivity counts of the serum and resin are made, and the percentage of thyroid hormones absorbed by the resin is calculated. – A low percentage of absorption indicates a poorly functioning thyroid gland. – A high percentage of absorption indicates hyperactivity. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Two Adrenal Glands Located above each of the kidneys Each gland is composed of two sections: – Adrenal cortex – Adrenal medulla Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Figure 13-11: The adrenal glands. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Outer Adrenal Cortex Manufactures Several Different Families of Hormones They are all produced by The adrenal cortex of the cortex; they are collectively referred to as corticosteroids. The mineralocorticoid hormone, aldosterone, regulates sodium (Na+) and potassium (K+) levels in the body. The glucocorticoid hormone, cortisol, regulates carbohydrates in the body. both men and women secretes steroid sex hormones: androgens, estrogen, and progesterone. They regulate secondary sexual characteristics. The inner portion of the adrenal medulla secretes epinephrine and norepinephrine. Epinephrine is also called adrenaline. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Structure and Function of the Adrenal Glands The adrenal glands are located on top of each kidney. Each of the glands consists of two distinct parts: an outer part (the adrenal cortex) and an inner section (the adrenal medulla). The cortex and medulla secrete different hormones. The adrenal cortex is stimulated by ACTH, adrenocorticotropic hormone, from the anterior pituitary gland. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Disease of the Adrenal Cortex Hyperactivity of the adrenal cortex is usually caused by hyperplasia (enlargement of the glands), a tumor. Hyperactivity may also result from over-stimulation by the anterior pituitary gland. Hypoactivity of the adrenal cortex sometimes results from a destructive disease, such as tuberculosis. Some steroid hormones can cause the adrenal glands to atrophy by interfering with the normal control mechanism for corticosteroid release. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Hyperadrenalism Overactivity of the adrenal cortex (hyperadrenalism) can take different forms depending on which group of hormones are secreted in excess. – Cushing’s syndrome – Conn’s syndrome – Adrenogenital syndrome – Pheochromocytoma Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Table 13-1: Signs and symptoms of Graves’ disease. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Cushing’s Syndrome Excess of glucocorticoid hormones Signs and symptoms: result from decreased protein synthesis – Hyperglycemia (adrenal diabetes) – Mobilization of lipids (trunk obesity, buffalo hump, but the arms and legs remain normal, moon shaped face) – Sodium and water, retention resulting in hypertension – Atherosclerosis develops as a result of excess circulating lipid. – Muscular weakness and fatigue accompany the disease, and the person finds it difficult even to climb stairs. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Cushing’s Syndrome (continued) Signs and symptoms: result from decreased protein synthesis (continued) – Easy bruisability, striae (stretch marks) develop on the abdomen, buttocks, and breasts – Poor wound healing – Increased susceptibility to infection – Bones, particularly the vertebrae and ribs, are likely to fracture. Treatment: surgical removal of the enlarged glands or tumor can correct the condition. Hormonal therapy is then required to replace the hormones normally secreted by the adrenal cortex. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Conn’s Syndrome Aldosterone is secreted in excess – Retention of sodium and water, and abnormal loss of potassium in the urine – Hypertension develops as a result of the salt imbalance and water retention. – Muscles become weak to the point of paralysis. – Excessive thirst (polydipsia) caused by the salt retention – Polyuria follows the great intake of water. Conn’s syndrome is usually caused by a tumor that can be removed surgically, and the prognosis is usually good. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Adrenogenital Syndrome Adrenal virilism – Androgens, male hormones, are secreted in excess. If this occurs in children, it stimulates premature sexual development. Sex organs of a male child greatly enlarge. In a girl, the clitoris enlarges, a male distribution of hair develops, and the voice deepens. Etiology: a block in the synthesis of cortisol from cholesterol or from other corticosteroids. – Cortisone is generally inactive until it is converted to cortisol. Cortisone is prepared synthetically from animal and plant tissue. Inasmuch as steroids cannot be converted to cortisol, because of the blockage in the pathway, they are converted to androgens. Cortisol treatment can prevent this overproduction. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Adrenogenital Syndrome (continued) Excessive androgen secretion in a woman causes masculinization (adrenal virilism). Hair develops on the face, a condition called hirsutism, and the hairline recedes. The breasts diminish in size, the clitoris enlarges, and ovulation and menstruation cease. In an adult, the cause is usually an androgen-secreting tumor of the glands. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Pheochromocytoma A rare tumor of the adrenal medulla that causes overproduction of epinephrine and norepinephrine Occurs equally in men and women, most commonly between the ages of 30 and 60 Symptoms of palpitations, increased blood pressure, rapid heart rate, chest pain, and weight loss may appear suddenly and sporadically. Treatment: surgical removal the tumor; medications are also used before surgery to control symptoms caused by excessive epinephrine and norepinephrine Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Hypoadrenalism Addison’s disease—adrenal glands fail to produce corticosteroids, aldosterone, and cortisol Etiology: destruction or damage to the adrenal glands by cancer, infections, or inhibited by chronic use of steroid hormones, such as prednisone; many cases are called idiopathic Aldosterone deficiency renders the patient unable to retain salt and water. Kidneys are unable to concentrate urine and, eventually, dehydration ensues. Severe dehydration can ultimately lead to shock. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Hypoadrenalism (continued) Cortisol deficiency leads to low blood sugar, impaired protein and carbohydrate metabolism, and generalized weakness. Pituitary gland produces more corticotropin in response to a deficiency of corticosteroids. Corticotropin normally stimulates the adrenal gland and production of a skindarkening pigment called melanin. Persons with Addison’s disease develop a peculiar yellow-brown discoloration. Addison’s disease can be life-threatening and must be treated with corticosteroid replacement. Injectable cortisol treatment is used initially to treat severe cases. Oral cortisol treatment is required for life. Medication to restore normal excretion of salt and water is also administered. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Parathyroid Glands Four tiny glands located on the dorsal surface of the thyroid gland The parathyroid hormone (PTH) secreted by these glands regulates the amount of calcium in the blood. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e If calcium levels in the blood fall too low, parathyroid hormone levels in the blood are increased and will stimulate bone breakdown to release more calcium into the blood. Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Figure 13-12: Parathyroid glands. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Function of the Parathyroids Regulate the level of circulating calcium and phosphate, and osteoclastic and osteoblastic activity When the blood calcium level falls, parathormone is secreted. – Parathormone increases the amount of calcium that is absorbed out of the digestive tract by interaction with ingested vitamin D. – It prevents a loss of calcium through the kidneys and releases calcium from bones by stimulating osteoclastic activity. – When the proper level of circulating calcium is restored, parathormone is no longer released. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Hyperparathyroidism Excessive parathormone raises the level of circulating calcium above normal, the condition called hypercalcemia. – Much of the calcium comes from bone resorption mediated by parathormone. As the calcium level rises, the phosphate level falls. With the loss of calcium, the bones tend to weaken, bend, become deformed, and fracture spontaneously. Giant cell tumors and cysts of the bone sometimes develop. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Hyperparathyroidism (continued) Excessive calcium causes formation of kidney stones because calcium forms insoluble compounds. Calcium deposited within the walls of the blood vessels makes them hard. It may also be found in the stomach and lungs. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Figure 13-13: Tetany of the hand in hypoparathyroidism. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Complications of Hyperparathyroidism – Hypercalcemia See Table 13-3 Kidney stone formation Calcification of blood vessel walls Calcification of organ walls Spontaneous fractures Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Hyperparathyroidism With its concurrent excess of calcium, causes generalized symptoms Bone pain, depression of the nervous system and muscle weakness; heart muscle is affected and the pulse slows Gastrointestinal disturbances, abdominal pain, vomiting, and constipation develop. Deposits of calcium sometimes form in the eye, causing irritation and excessive tearing. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Hyperparathyroidism (continued) Hyperparathyroidism usually results from a tumor. If the tumor is removed, parathormone secretion returns to normal, and the level of circulating calcium is again properly controlled. Hyperparathyroidism can develop from other conditions that reduce the level of circulating calcium. Any decrease in calcium stimulates the parathyroid glands to hypertrophy and to increase their rate of secretion. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Table 13-3: Complications of hyperparathyroidism hypercalcemia Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Hypoparathyroidism The principal manifestation of hypoparathyroidism is tetany, a sustained muscular contraction. The muscles of the hands and feet contract in a characteristic fashion. Laryngeal muscles are very susceptible to these spasms, which can obstruct the respiratory tract, and death may follow. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Hypoparathyroidism (continued) The low level of calcium in the blood, hypocalcemia, makes the nervous system hyper-excitable. As the nerves discharge spontaneously, the skeletal muscles are over-stimulated. Administration of calcium and vitamin D, which assists in the absorption of calcium from the gastrointestinal tract, will correct the condition. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Pancreas Located along the lower Insulin, produced by islet cells, curvature of the stomach. The only organ in the body that has both endocrine and exocrine functions. The exocrine portion of the pancreas releases digestive enzymes through a duct into the duodenum of the small intestines. The endocrine sections of the pancreas, islets of Langerhans, produce insulin and glucagon. stimulates the cells of the body to take in glucose from the bloodstream. Loss of insulin results in diabetes mellitus (DM) and hyperglycemia, which is a high blood sugar level. Overproduction of insulin will result in hypoglycemia, or a low blood sugar level. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Figure 13-14: Islet of Langerhans. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Figure 13-15: Control of blood glucose level. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Endocrine Function of the Pancreas Control of glucose level in the blood; accomplished through the secretion of two hormones, insulin and glucagon – Insulin is secreted by certain cells of the pancreas called beta cells, located in patches of tissue named the islets of Langerhans or pancreatic islets. – Lowers serum glucose, insulin facilitates the entry of glucose into the cells where it is primarily stored as glycogen and metabolized for energy. Glucose enters primarily skeletal muscle cells and fat cells. Glucagon is secreted by the alpha cells of the islets. – When the level of blood glucose falls below normal, glucagon is released. Glucagon circulates to the liver and stimulates the release of glucose from its stored form, glycogen Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Diabetes Mellitus Type 1 Type 2 Destruction of the islet The person makes a cells; the person fails to produce an adequate amount of insulin Must take insulin injections to replace the insulin the pancreas is unable to produce Called insulin-dependent diabetes mellitus (IDDM) sufficient amount of insulin, but it has lost its ability to influence the cells of the body. Do not take insulin Called non-insulindependent diabetes mellitus (NIDDM) Treated by diet, exercise, and oral medications Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Table 13-2: Hyperadrenalism Signs and Symptoms. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Symptoms of Diabetes Mellitus Polyuria, caused by excessive filtration of glucose into the kidney tubule and the volume of water required to carry it away, or the diuretic effect of glucose Excess glucose is excreted in the urine, a condition called glycosuria Polydipsia: an unusual excessive thirst Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Symptoms of Diabetes Mellitus (continued) Cells prefer to metabolize glucose, but in its absence, cells metabolize fats first and proteins last. – Because glucose cannot enter the cells without the action of insulin, the diabetic metabolizes a large amount of fat. Fat metabolism produces a large number of fatty acids, ketone bodies, acetone, and related substances. The production of acids lowers the body’s pH, resulting in the condition of acidosis – Normal pH range is 7.35 to 7.45. – Coma and death results with a pH below 6.9 to 7.0. – Weight loss and fatigue due to mobilization of fat and protein for energy Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Click here to view videos on the topic of diabetes. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Return to Directory Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Click on the screenshot to view an animation on the topic of diabetes. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Return to Directory Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Complications of Diabetes Mellitus Atherosclerosis: increased lipid mobilization, serum cholesterol, poor wound healing Blockage of a coronary artery causes myocardial infarction Thromboembolic strokes Occlusion of a leg artery can result in gangrene; atherosclerosis generally causes poor circulation Diabetic retinopathy, a vascular disorder of the retina that can result in blindness; the minute retinal blood vessels become sclerotic and rupture The nervous system is affected by poor circulation, as manifested by pain, tingling sensations, loss of feeling, and paralysis. Kidney failure Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Figure 13-16: Complications of diabetes mellitus. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Treatment of Diabetes Mellitus Regulation of diet, exercise, insulin, and hypoglycemic medications Regulation of the proper insulin dosage may vary – Illness or emotional stress can temporarily alter a patient’s needs. – Monitoring blood sugar levels is an essential part of diabetes care. Self-monitoring of blood glucose enables the diabetic to determine his or her blood glucose and adjust insulin dosage according to a measured reading. Oral medications mostly used for type 2 diabetes – These are oral hypoglycemic agents, which stimulate secretion of insulin from beta cells that still have some capacity or make cells more responsive to insulin. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Diabetic Coma Develops from failure to take enough insulin or deviation from a prescribed diet. Acidosis and dehydration can follow if proper treatment is not given immediately. – Symptoms: deep, labored breathing, acidosis, fruity acetone breath, dry mouth, flushed and dry skin – Treatment of diabetic coma (diabetic ketoacidosis) requires urgent replacement of fluids to correct the dehydration. Insulin, usually given intravenously, is given as well. Because diabetic coma adversely affects sodium and potassium, the serum electrolytes must be checked frequently as therapy proceeds. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Insulin Shock Too much insulin, not enough food, or excessive exercise Symptoms: light-headedness, faintness, trembles, and perspiration Taking sugar in some form, candy or orange juice for example, may be adequate treatment at this stage. If the glucose level is not raised, speech becomes thick and walking becomes unsteady. Double vision may be experienced, a loss of consciousness may follow. Without treatment coma may result. Shallow breathing Intravenous injections of glucose must be given immediately for insulin shock. The administration of epinephrine raises the blood sugar level. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Table 13-3: Complications of Hyperparathyroidism: Hypercalcemia. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Insulin Shock See Figure 13-7 Difference between insulin shock and diabetic coma Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Tests for Diabetes Mellitus Urine test for ketones Fasting blood glucose levels, glucose tolerance testing, and glycosylated hemoglobin testing are used to monitor and diagnose diabetes. – For the fasting blood glucose level test, a sample of blood is taken after the person has fasted for eight hours. – The glucose tolerance test challenges the body’s ability to secrete and use insulin. The test is performed after a 10-hour fast. The patient drinks a standard glucose solution, and blood and urine sample are taken and analyzed for the next three hours. No glucose should appear in the urine, and the blood glucose levels should not exceed 170 mg/dl of blood if insulin is being produced and utilized. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Tests for Diabetes Mellitus (continued) Fasting blood glucose levels, glucose tolerance testing, and glycosylated hemoglobin testing are used to monitor and diagnose diabetes (continued). – Glycosylated hemoglobin determination is a simple blood test that is used to monitor long-term control of diabetes. It generally indicates the average blood glucose levels over the past 90 days. Normal values should be below 6, and levels for diabetics should be less than 7. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Abnormalities in Secretion of Sex Hormones The gonads (ovaries and testes) are endocrine glands as well as the source of the ova and sperm. They secrete the hormones estrogen and testosterone directly into the blood. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Hypergonadism (Hypersecretion) Abnormally increased functional activity of the gonads before puberty produces precocious sexual development in both sexes. In a male child, excessive production of testosterone may be caused by a tumor in the testes. – This causes rapid growth of musculature and bones but premature uniting of the epiphyses and shaft of long bones. – Normal height, therefore, is not attained. Hypersecretion of ovarian hormones in the female is rare because of the negative feedback mechanism with gonadotropic hormones. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Hypogonadism in the Male Several factors can cause hypogonadism – Congenital: born without functional testes – The testes may fail to descend and thus atrophy – Castration: the testes may be lost through castration Testes fail to develop because of lack of gonadotropic hormone. Loss of the male gonads before puberty causes the condition of eunichism, in which sexual characteristics do not develop. Development of male traits depends on testosterone secreted by the testes. Castration after puberty causes some regression of secondary sexual characteristics, but masculinity is retained. Hormonal therapy, the administration of testosterone, can be effective. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Hypogonadism in the Female Hyposecretion of hormones by the ovaries may be caused by poorly formed or missing ovaries. When ovaries are absent or fail to develop, female eunichism results. Secondary sexual characteristics do not develop. A characteristic of this condition is excessive growth of long bones because the epiphyses do not seal with the shaft of the bone as normally occurs at adolescence. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Changes in Endocrine Function with Age Decrease in growth hormone – In men after age 30 a decrease in lean body mass and decreases in thickness and strength of bone matrix. – Increased body fat is correlated with greater risk of diabetes, heart disease, and cancer. Decreased bone density makes bones more susceptible to fracture. A slight decrease in T3/T4 ratio, resulting in decreased metabolic rate. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Changes in Endocrine Function with Age (continued) Aldosterone levels remain relatively steady: age-related decline in the kidney’s sensitivity to aldosterone, diminished capacity of the kidney to secrete renin when needed. The body is less able to deal with the stress of changes in blood pressure, dehydration, and disease in general. There is an increased incidence of abnormalities in blood pressure, sodium and potassium levels, acid/base balances, and osmotic pressure. The pancreas retains the ability to secrete insulin at normal levels with age, but tissue responsiveness to insulin decreases. Insulin resistance leads to a greater incidence of NIDDM. Androgen and estrogen levels drop with age. Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved. Diagnostic Procedures Serum Assay – Growth hormone levels (pituitary disorders) – TSH, T3, T4 (thyroid disorders) – Parathyroid hormone, calcium (parathyroid disorder) – Cortisol (adrenal disorder) – Glucose levels, tolerance test, hemoglobin A1c Urine specimen and vasopressin test CT scan Ultrasound Mulvihill, Zelman, Holdaway, Tompary, and Raymond Human Diseases: A Systemic Approach, 6e Copyright ©2006 by Prentice-Hall, Inc. Upper Saddle River, New Jersey 07458 All rights reserved.