Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
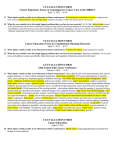
VARIAN MEDICAL SYSTEMS | CLINICAL PERSPECTIVES | BR EAST Prone breast radiotherapy to optimally spare heart and lung Significant strides continue to be made in the diagnosis and treatment of breast cancer. Although access to mammography has broadened, and the incidence of estrogen-sensitive tumors has declined, breast cancer remains the most commonly diagnosed cancer and the second leading cause of cancer death among women in the United States. Each year, approximately 200,000 A new cases of breast cancer are diagnosed and 40,000 women die from it.1 This paper underscores the importance of radiation therapy in breast cancer survival and supports the increasing evidence that the prone setup position is advantageous in minimizing unwanted dose to critical organs. The issues outlined here present an exciting opportunity for additional study to optimize tissue sparing techniques for breast cancer treatment. FIGURE 1. SUPINE (A) AND PRONE (B) SCANS AT THE LEVEL OF LATERAL MARKERS SHOW HOW THE SHAPE AND SITE OF THE POSTSEGMENTAL EXCISION SEROMA VARIES BASED ON PATIENT’S POSITION. WHEN PRONE, THE CAVITY ELONGATES AND IS MORE DISTANT FROM THE CHEST WALL. SAME PATIENT AS IN FIGURE 2, ONE MONTH FOLLOWING BREAST SURGERY. FORMENTI, SILVIA. SEMINARS IN RADIATION ONCOLOGY, VOLUME 15, ISSUE 2, APRIL 2005, PAGES 92-99. the trials were conducted, the study underscored the importance of excluding the lungs and especially the heart from the treatment fields when irradiating the breast. All of these women were treated in the supine position. Radiation saves lives Improvement with prone setup In improving breast cancer survival, radiation has an important role to play. Breast-conserving lumpectomy followed by radiation to the whole breast has replaced mastectomy as the standard of care for patients with small tumors.2 Post-operative radiation therapy—after lumpectomy or mastectomy—significantly reduces local recurrence of the cancer and improves survival rates. A large meta-analysis published in the Lancet in 2005 analyzed 42,000 patients from 72 randomized trials conducted between 1958-1991, demonstrating a 5 percent improved 15-year survival rate among women who had received radiation treatment.3 Radiation treatment for breast cancer has traditionally been planned and delivered with patients in the supine position. However, there is increasing evidence that the prone treatment position affords several potential advantages over supine treatment. These include Preventing heart and lung toxicity Several trials investigated treating patients in the prone position to provide better heart and lung sparing.5, 6, 7, 8 A 2007 trial of 91 patients, conducted at the New York University (NYU) Cancer Institute, concluded that accelerated whole breast intensity modulated radiotherapy in the prone position is feasible and can drastically reduce the volume of lung and heart tissue exposed to radiation.9 To determine when prone setup is optimal, a Another study, however, also revealed a significantly higher 15-year mortality rate from heart disease and secondary lung cancers among breast-cancer patients treated with radiation. Furthermore, more patients treated for left breast cancer died from heart disease than those treated for right breast cancer.4 While the precision of radiation techniques has improved since • B etter normal tissue sparing with less delivered dose to critical organs • Improved dose homogeneity • Less motion due to respiration • Reduction in skin toxicity and fewer skin related effects B subsequent NYU prospective trial involved 200 left-breast and 200 right-breast cancer patients.10 All patients received 48 Gy in 15 fractions of IMRT. Each patient underwent two CT simulations and planning in the supine and prone position. For patients with left-breast cancer, the plan that minimized the volume of heart in the field was chosen for treatment. For patients with right-breast cancer, the plan with the least volume of lung in the field was chosen. The prone position proved optimal for the majority of both right and left breast patients, regardless of breast size. The prone position spared lung volume in 98 percent of the right breast patients, reducing the volume of lung in the treatment field by a mean 107 cubic centimeters. The prone position was optimal for 85 percent of the left breast patients, reducing exposed lung volume by a mean of 93 cubic centimeters (cc) and heart volume by a mean of 11 cc. Figure 2, which was printed in the New York Times11, shows a patient example of the better sparing of normal tissue that can be achieved in the prone position. Areas to explore In the NYU study, breast size did not predict the optimum setup position, since both large and small-breasted women benefited from prone positioning. Selection parameters for prone versus supine setup is an area that needs further investigation. While prone set-up provided better heart sparing for the vast majority (85 percent) of left-breast patients, the supine position was the best in 15 percent of cases. Techniques for prone setup need to be standardized. For example, the NYU study10 found that turning a patient’s head to the left could reduce heart volume in the treatment field when treating the left breast. Differences in the results from trials of prone positioning may be attributed to different positioning techniques and accessories. Summary Radiation after surgery improves survival from breast cancer, but it can increase the risk of mortality from heart disease and secondary lung cancer. There is growing evidence that special care must be taken to spare lung and especially heart tissue. Prone setup can drastically reduce the heart and lung volume in the treatment field, compared to supine setup. Further study of selection parameters for prone versus supine setup is needed. Prone setup techniques to better spare normal tissue, and ultimately, improve long term outcomes, are still in need of standardization. References A B FIGURE 2. (A,B) IMPROVED HEART AND LUNG SPARING IN THE PRONE POSITION (A) SUPINE, HEAD FIRST (B) PRONE, HEAD FIRST IMAGES COURTESY OF NYU These reconstructed digital radiographs compare supine (A) and prone (B) set up, showing the position of the lung (brown), heart (blue), and tumor bed (red). The yellow frame represents the beam’s eye view of the field. The insets above are the corresponding supine and prone computed tomography cut, at the level of the plane identified by radio-opaque markers. The prone set-up (B) characteristically enables better sparing of normal tissue than the supine set-up (A).12 A partner for life 1. Jemal A, et al. Cancer Statistics 2010, CA Cancer J Clin; 60(5): 277–300 2. NIH Consensus Development Conference statement: Adjuvant therapy for breast cancer, November 1-3, 2000; J Natl Cancer Inst Monogr 30:5-15, 2001 3. Clarke M, et al. Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: an overview of the randomized trials, Lancet 2005 Dec 17;366(9503):2087-106. 4. Darby S et al, Lancet oncology 2005:6;(8)557-565 5. Formenti et al. IJROBP. 60(2):493-504.2004 6. Buijsen et al. IJRO. 82(1):337-340. 2007 7. Morrow et al. IJROBP. 69(3):910-917. 2007 8. Varga et al. IJROBP. 1-7. 2009 9. Formenti, S, et al. Phase I-II Trial of Prone Accelerated Intensity Modulated Radiation Therapy to the Breast to Optimally Spare Normal Tissue, JCO 2007; 25(16): 2236-2242 10. Formenti S, et al. Results of NYU 05-181: A Prospective Trial to Determine Optimal Position (Prone versus Supine) for Breast Radiotherapy, IJROBP 2009; 75(3): S203-S204 11. Grady. Shorter Radiation for Cancer of the Breast. New York Times 2008 Sep 22. http://www.nytimes.com/2008/09/23/health/research/23canc.html?pagewanted=all 12. DeWyngaert et al. Accelerated Intensity-Modulated Radiotherapy to Breast in Prone Position: Dosimetric Results, IJROBP 2007; 68(4):1251-1259. 2007 USA Headquarters, California Varian Medical Systems Palo Alto, CA Tel: 650.424.5700 800.544.4635 Fax:650.493.5637 www.varian.com RAD 10164 © 2010 Varian Medical Systems, Inc. 10/10 (500)