Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Cardiac surgery wikipedia , lookup
Saturated fat and cardiovascular disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Cardiovascular disease wikipedia , lookup
Myocardial infarction wikipedia , lookup
Coronary artery disease wikipedia , lookup
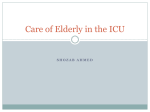
Sleep-Disordered Breathing and Cardiovascular Disorders Rohit Budhiraja MD, Pooja Budhiraja MD, and Stuart F Quan MD Introduction Obstructive Sleep Apnea and Hypertension Obstructive Sleep Apnea and Coronary Artery Disease Sleep-Disordered Breathing and Congestive Heart Failure Sleep-Disordered Breathing and Arrhythmias Sleep-Disordered Breathing and Stroke Potential Pathogenetic Mechanisms of Cardiovascular Disease in Sleep-Disordered Breathing Sleep-Disordered Breathing and Excess Mortality Summary Compelling data demonstrate a strong association between sleep-disordered breathing (SDB) and cardiovascular disorders. The association is most consistent between obstructive sleep apnea (OSA) and hypertension. Epidemiologic and clinic-based studies provide evidence for an etiological role of OSA in hypertension, independent of obesity. Furthermore, several studies suggest amelioration of hypertension with therapy for sleep apnea. Emerging data also suggest a role for OSA in causing coronary artery disease. This association is bolstered by evidence suggesting that continuous positive airway pressure (CPAP) therapy improves early signs of atherosclerosis and may impede progression to clinically important cardiovascular disease. SDB (both OSA and central sleep apnea) is frequently observed in patients with heart failure. OSA may be a risk factor for incident heart failure. The current data do not provide consistent evidence for whether treatment of SDB will improve survival or other end points in patients with heart failure, and larger trials are currently underway to better elucidate that relationship. Substantial evidence also links SDB to an increased risk of various arrhythmias. Treatment of SDB with CPAP appears to significantly attenuate that risk. Finally, several studies suggest SDB as a risk factor for stroke. Whether treatment of SDB reduces stroke risk, however, remains to be determined. In conclusion, persuasive data provide evidence for an association, probably causal, between sleep-disordered breathing and several cardiovascular disorders. Large randomized controlled trials will further help confirm the association and elucidate the cardiovascular benefits of SDB therapy. Key words: sleep-disordered breathing; cardiovascular disease; obstructive sleep apnea; OSA; hypertension; obesity; continuous positive airway pressure; CPAP; atherosclerosis. [Respir Care 2010;55(10):1322–1330. © 2010 Daedalus Enterprises] Rohit Budhiraja MD and Pooja Budhiraja MD are affiliated with the Department of Medicine, Southern Arizona Veterans Affairs Health Care System, and with the Department of Medicine, University of Arizona College of Medicine, Tucson, Arizona. Rohit Budhiraja MD is also affiliated with the Arizona Respiratory Center, University of Arizona College of Medicine, Tucson, Arizona. Stuart F Quan MD is affiliated with the Arizona Respiratory Center, University of Arizona College of Medicine, Tucson, Arizona, and with the Division of Sleep Medicine, Harvard Medical School, and Brigham and Women’s Hospital, Boston Massachusetts. 1322 Dr Quan presented a version of this paper at the 45th RESPIRATORY CARE Journal Conference, “Sleep Disorders: Diagnosis and Treatment,” held December 10-12, 2009, in San Antonio, Texas. This research was partly supported by National Institutes of Health grant HL53938 and Stanford University subcontract HL068060. Correspondence: Stuart F Quan MD, Division of Sleep Medicine, Harvard Medical School and Brigham and Women’s Hospital, 401 Park Drive, 2nd Floor East, Boston MA 02215. E-mail: [email protected]. RESPIRATORY CARE • OCTOBER 2010 VOL 55 NO 10 SLEEP-DISORDERED BREATHING Introduction Sleep-disordered breathing (SDB), expressed most frequently as obstructive sleep apnea (OSA), is a common syndrome, and becomes progressively more prevalent with increasing age.1 For the past several decades, a number of cross-sectional studies, performed primarily in relatively small clinical cohorts or using surrogates such as snoring as markers of SDB, have reported linkages between SDB and cardiovascular disease. For example, a high prevalence of OSA has been observed in patients with hypertension.2 Conversely, hypertension is found in a large percentage of OSA patients. With respect to cardiac disease, early studies linked OSA to ischemic heart disease.3,4 In addition, it has been shown that OSA is associated with deterioration in left-ventricular function5 and that treatment of OSA with continuous positive airway pressure (CPAP) improves cardiac function. If SDB plays a causal role in the pathogenesis of cardiovascular disease, higher mortality would be expected among individuals with OSA. This hypothesis was supported in some6,7 but not all8 retrospective studies. Whether SDB is an independent risk factor for cardiovascular disease is an important public health question. According to the 1999 –2000 National Health and Nutrition Examination Survey, the prevalence of hypertension in the United States in those over age 55 years is 48%.9 According to the year 2000 census, there are approximately 59 million Americans age 55 or older. If 25–50% of these individuals also have OSA, then 14 –29 million of those people are at increased risk for cardiovascular disease or excess mortality related to OSA. In the past several years a persuasive body of data now indicates a causal association, independent of obesity, between SDB and cardiovascular disorders such as hypertension, coronary artery disease, arrhythmias, congestive heart failure, and stroke. The association is strongest and most consistent between OSA and hypertension. This review will summarize the most important studies demonstrating the linkages between SDB and cardiovascular disease, and outline potential responsible mechanisms. Obstructive Sleep Apnea and Hypertension Cogent data confirm the association between OSA and hypertension.10 Several epidemiologic and clinic-based studies conducted in cross-sectional as well as longitudinal designs have demonstrated a strong and consistent relationship between these disorders. Peppard et al found a causal association between SDB at baseline and the presence of hypertension 4 years later in 709 subjects in the Wisconsin Sleep Cohort, and the odds of hypertension increased with increasing baseline AHI.11 The association was independent of age, sex, body mass index, waist and neck circumference, baseline hypertension, smoking, and RESPIRATORY CARE • OCTOBER 2010 VOL 55 NO 10 AND CARDIOVASCULAR DISORDERS alcohol use. The odds ratios for hypertension continued to be significant when those hypertensive at baseline were excluded. Recent analyses of data from this cohort demonstrated dose-response increased odds of incident nocturnal non-dipping of systolic blood pressure, a risk factor for hypertensive complications, in participants with SDB over an average of 7.2 years of follow-up.12 A cross-sectional analysis of the Sleep Heart Health Study arrived at similar conclusions.13 Persons with an AHI ⱖ 30 events/h had a 1.37-fold greater odds of hypertension than those without OSA (AHI ⬍ 1.5 events/h), after adjusting for several confounders. However, recent prospective analyses of data from the Sleep Heart Health Study found that the relationship between the baseline AHI and the risk of developing hypertension approached but did not quite reach statistical significance after adjustment for body mass index.14 However, the odds ratio in the longitudinal analysis was quite similar to that in the crosssectional analysis, suggesting that a causal relationship is most likely present and obscured by residual confounding. The older age of participants in this study, exclusion of those with baseline hypertension, and different methods of diagnostic testing are among the potential reasons the results of these analyses differ from those of the Wisconsin Sleep Cohort.15-17 Other epidemiologic and clinic-based studies provide corroborating evidence for an association between SDB and hypertension. In the Nurses Health Study, snoring, a surrogate symptom of SDB, was associated with an increased risk of incident hypertension over an 8-year follow-up period.18 The Outcomes of Sleep Disorders in Older Men Study (an ancillary study of the Osteoporotic Fractures in Men Study) revealed 1.6-fold higher odds of hypertension in elderly men with SDB.19 Persons with OSA also have a significantly higher prevalence of non-dipping of blood pressure at night.20 Conversely, drug-resistant or poorly controlled hypertension is associated with a high prevalence of concomitant undiagnosed SDB.21,22 Another line of evidence supporting SDB as a causal factor in hypertension is provided by trials demonstrating amelioration, albeit modest, of hypertension with therapy of sleep apnea.23 The changes in mean blood pressure after CPAP have been suggested to be on the order of 2–5 mm Hg.24 Studies cumulatively suggest better antihypertensive response with CPAP in patients with daytime sleepiness than those without excessive sleepiness.25-27 Refractory hypertension may also improve with CPAP therapy in persons with comorbid OSA.21 In addition, mandibular advancement devices and otolaryngological surgery are associated with improvement in blood pressure in patients with OSA.28 However, there has been a lack of consistent demonstration of antihypertensive effects of OSA therapy.29 This discrepancy may emanate from diverse populations and 1323 SLEEP-DISORDERED BREATHING sample sizes, varying diagnostic techniques, and different definitions for apneas and hypopneas, as well as dissimilar follow-up periods in different studies. In conclusion, consistent data suggest a strong causal association between OSA and hypertension. Preliminary trials evaluating therapy of OSA suggest amelioration of hypertension in some subgroups with sleep apnea, but larger prospective trials are clearly needed to unambiguously elucidate the effects of OSA therapy on blood pressure and related outcomes. Obstructive Sleep Apnea and Coronary Artery Disease The evidence suggesting an association between OSA and coronary artery disease continues to accrue. One study showed an increased prevalence and extent of coronary artery calcium, a marker of subclinical coronary artery disease, in patients with OSA.30 Presence of sleep apnea in the Osteoporotic Fractures in Men Study cohort was associated with 1.2-fold increased odds of the presence of cardiovascular disease.19 Cross-sectional analyses of data from the Sleep Heart Health Study revealed higher odds of self-reported coronary artery disease, heart failure, and stroke in persons with high AHI.31 Preliminary longitudinal analyses of the Sleep Heart Health Study data indicate that the risk of incident coronary artery disease is primarily in men less than age 70 years.32 Other prospective observational studies in clinical populations have demonstrated a higher incidence of cardiovascular disorders in persons with OSA33,34 as well. Cardiovascular mortality is also increased in OSA.35 One study with a mean of 10.1 years of follow-up found that participants with untreated severe OSA had a higher incidence of fatal cardiovascular and non-fatal cardiovascular events, compared to healthy participants.36 However, this latter study was recruited from a clinical population and included only men. In persons with coronary artery disease undergoing elective percutaneous intervention, OSA is associated with restenosis and vessel remodeling.37 There is also an increase in the incidence of major adverse cardiac events such as revascularizations and cardiac mortality after percutaneous intervention in patients with OSA.38 Furthermore, OSA patients demonstrate smaller increases in leftventricular ejection fraction and regional wall motion within the infarct area days after percutaneous intervention.39 Finally, treatment of OSA after percutaneous intervention is associated with a reduction in the number of cardiac deaths.40 Treatment of OSA may alleviate cardiovascular risk. One study revealed significantly lower combined end points of cardiovascular death, acute coronary syndrome, hospitalization for heart failure, or need for coronary revascu- 1324 AND CARDIOVASCULAR DISORDERS larization in persons treated for OSA, compared to those with OSA who declined therapy (hazard ratio 0.24).41 In the study by Marin et al,36 cardiovascular disease risk in those with severe OSA treated with CPAP was the same as in non-OSA patients. As outlined in the foregoing discussion, accumulating data in cross-sectional and longitudinal observational studies implicate SDB as an independent risk factor for cardiovascular disease. In addition, evidence suggests that CPAP therapy improves early signs of atherosclerosis and may impede progression to clinically important cardiovascular disease.42 Cardiac biomarkers such as C-reactive protein may decline with CPAP treatment as well.43 Nevertheless, there have been no large-scale randomized studies demonstrating that treatment of SDB reduces cardiovascular disease risk. Recently, however, 2 large randomized clinical trials were started to determine whether OSA treatment impacts cardiovascular disease risk. In Europe, a large prospective randomized CPAP intervention in 400 patients with coronary artery disease and OSA is aimed at assessing the impact of CPAP treatment on a composite end point of new revascularization, myocardial infarction, stroke, and cardiovascular mortality over a 3-year period in persons with coronary artery disease and OSA.44 In the United States, the multicenter HeartBEAT study will randomize 352 subjects with OSA and coronary artery disease or coronary artery disease risk factors to CPAP, lowflow nocturnal oxygen, and health-lifestyle instruction to determine whether CPAP or oxygen affects cardiac biomarkers. Another clinical trial, the Continuous Positive Airway Pressure Treatment of Obstructive Sleep Apnea to Prevent Cardiovascular Disease, is being conducted in several international sites to determine whether CPAP will reduce incident cardiovascular disease. Enrollment of 5,000 subjects is planned, with study sites in Australia, China, India and New Zealand. In conclusion, data suggesting an association between OSA and clinical and subclinical coronary artery disease continue to accrue. Large prospective trials will help better elucidate the impact of OSA therapy on improvement of cardiovascular morbidity. Sleep-Disordered Breathing and Congestive Heart Failure SDB is present in approximately three fourths of patients with symptomatic or decompensated systolic heart failure.45,46 The prevalence is very high, even in those with stable chronic heart failure.47-49 Cross-sectional analyses from the Sleep Heart Health Study data revealed an adjusted odds ratio of 2.2 for self-reported heart failure among subjects with OSA.31 Of all heart-failure patients with sleep apnea in one study, 40% had AHI ⬎ 30 events/h.47 Patients with SDB were older and had higher body mass RESPIRATORY CARE • OCTOBER 2010 VOL 55 NO 10 SLEEP-DISORDERED BREATHING index and brain-natriuretic peptide, despite similar leftventricular ejection fraction and functional class of heart failure. There is little published longitudinal data, but preliminary longitudinal analyses of data from the Sleep Heart Health Study indicate that men, but not women, have an increased risk of incident congestive heart failure as a consequence of SDB, even after exclusion of subjects with central sleep apnea.32 Both OSA and central sleep apnea are encountered in heart-failure patients, and the proportion of these events has differed in different studies. It has been suggested that the reduction in PaCO2 and increase in lung-chemoreceptor circulation time in such patients can result in an overnight shift in the predominant apnea type from obstructive to central. Central sleep apnea is frequently accompanied by Cheyne-Stokes respiration, a breathing pattern characterized by repetitive sinusoidal waxing and waning of tidal volume amplitude. Central sleep apnea is an independent predictor of mortality in patients with heart failure or cardiac transplantation.50,51 The hazard ratio for early mortality in heart-failure patients with central sleep apnea in one study was 2.1 relative to those without central sleep apnea.50 CheyneStokes respiration is also associated with higher mortality.52 Furthermore, central sleep apnea/Cheyne-Stokes respiration may also promote cardiac electrical instability, with impaired heart-rate variability and enhanced occurrence of cardiac arrhythmias.53 Obstructive events are associated with a marked negative swing in intrathoracic pressure, which can lead to increased pre-load and after-load. Furthermore, sympathetic activation resulting from SDB and arousals can deteriorate cardiac function. CPAP therapy improves leftventricular ejection fraction and quality of life in heartfailure patients with OSA.54,55 CPAP use also decreases myocardial irritability and risk of arrhythmias.56 The prevalence of SDB is high not only in systolic heart failure but also in heart failure with normal ejection fraction. One study of 247 patients with heart failure with normal ejection fraction found SDB in 69%, OSA in 40%, and central sleep apnea in 29%.57 Central sleep apnea was associated with higher pulmonary artery wedge pressure and brain-natriuretic peptide, and lower PaCO2. Persons with central sleep apnea had a larger left atrial diameter than those with OSA, who in turn had more pronounced atrial enlargement than those with no SDB. However, whether diastolic dysfunction leads to SDB or vice versa is yet to be clearly elucidated. Presence of left-ventricular hypertrophy in OSA and regression of hypertrophy with CPAP has been documented in smaller studies.58,59 The effect of PAP therapy on central sleep apnea in patients with heart failure is not clearly understood. The Canadian Continuous Positive Airway Pressure Trial for Congestive Heart Failure Patients With Central Sleep Ap- RESPIRATORY CARE • OCTOBER 2010 VOL 55 NO 10 AND CARDIOVASCULAR DISORDERS nea (CanPAP) trial was designed to answer this question.60 CPAP improved nocturnal oxygenation, cardiac ejection fraction, and 6-minute walk distance, and lowered norepinephrine level, but did not improve heart-transplant-free survival or significantly alleviate central sleep apnea in many of the trial participants. Post-hoc analyses revealed significantly better transplant-free survival (hazard ratio 0.371, P ⫽ .043) in subjects whose AHI had been reduced to less than 15 events/h, compared to control subjects. Whether advanced methods of applying PAP in heart-failure patients will be more efficacious is unknown. Small clinical studies suggest that both bi-level PAP and adaptive servo ventilation may benefit some patients with central sleep apnea and heart failure.61 Larger trials are underway. Some studies have evaluated the effect of cardiac pacing on SDB. While one study suggested that atrial overdrive pacing can improve SDB,62 other studies have failed to consistently confirm this effect.63,64 It appears that pacing may have some benefits in alleviating SDB in patients with heart failure with predominantly central sleep apnea.65 However, larger trials are required to clearly understand the magnitude and physiologic basis of this effect. The effect of cardiac resynchronization therapy on central sleep apnea/Cheyne-Stokes respiration in patients with chronic heart failure has been more consistently demonstrated.66,67 An improvement in cardiac output and decreased pulmonary vascular congestion may be responsible for improvement of central events in heart failure. In summary, SDB in the form of both OSA and central sleep apnea is frequently observed in patients with heart failure. Improvement in cardiac function with cardiac resynchronization therapy may improve central sleep apnea. OSA may be a risk factor for incident heart failure, but it is currently unclear whether treatment of either OSA or central sleep apnea, or both forms of SDB will reduce the incidence of heart failure or improve survival in patients with heart failure. Sleep-Disordered Breathing and Arrhythmias Diverse cardiac arrhythmias such as atrial fibrillation, nonsustained ventricular tachycardia, and complex ventricular ectopy have been described in persons with SDB.68 It has been suggested that atrial fibrillation has a strong association with central sleep apnea, whereas complex ventricular ectopy is more closely associated with OSA.69 Conversely, the prevalence of undiagnosed OSA in patients with cardiac pacemaker implantation for diverse reasons is extremely high.70 Several mechanisms such as hypoxia, sympathetic activation and swings in intrathoracic pressure may explain this association. Recent analyses from the Sleep Heart Health Study demonstrated a 17-fold increased odds of an arrhythmia (atrial fibrillation and non- 1325 SLEEP-DISORDERED BREATHING sustained ventricular tachycardia) occurring after a respiratory disturbance than an arrhythmia occurring after normal breathing during sleep,71 providing corroborating evidence for the link between SDB events and arrhythmias. Arrhythmias can be severe and potentially lifethreatening. One study of 112 persons who had undergone polysomnography and had died suddenly from cardiac cause suggested that the peak in sudden cardiac death in those with OSA occurs primarily from midnight to 6 AM (ie, during the sleeping hours) (relative risk 2.6).72 The risk of arrhythmias in OSA significantly decreases with CPAP therapy. In an elegant study, arrhythmias were evaluated in 23 patients with moderate to severe OSA over a 14-month period, using a subcutaneously implanted loop recorder. The follow-up duration included 2 months with no OSA therapy, and 12 months thereafter on CPAP. The occurrence of severe arrhythmias was common prior to CPAP therapy, but decreased rapidly after initiation of CPAP therapy, with no ectopy recorded during the last 6 months of follow-up. Another study demonstrated lower recurrence of atrial fibrillation after elective cardioversion in OSA patients who were treated with CPAP therapy.73 In summary, substantial evidence links SDB as an etiologic factor in the pathogenesis of various arrhythmias, particularly atrial fibrillation. Treatment of SDB with CPAP appears to reduce this risk. Sleep-Disordered Breathing and Stroke Several studies suggest that SDB is a risk factor for stroke.74 However, these studies have been primarily case series, case-control studies, or used snoring as a surrogate for objective documentation of SDB. More recently, an observational cohort study in a clinical population found an increased rate of the composite outcome of stroke or death in patients with OSA over a 4-year interval, in comparison to those without OSA, with an adjusted hazard ratio of 1.97.75 Similar findings have been observed in the Wisconsin Cohort Study over a 4-year interval, although the fully adjusted odds ratio failed to reach statistical significance, in part because of inadequate study power.76 More recently, analysis of prospective data from the Sleep Heart Health Study suggested that severe SDB is an independent risk factor for stroke only in men.77 Whether treatment of SDB reduces stroke risk remains to be determined. Although there are now substantial data indicating that SDB is a risk factor for stroke, the converse also is true in that stroke appears to be a risk factor for the development of SDB.74 Unfortunately, CPAP is not well tolerated in post-stroke patients, and long-term adherence to CPAP therapy is low. Nevertheless, it appears that long-term survival after stroke is better among patients who adhere to CPAP therapy.78 1326 AND CARDIOVASCULAR DISORDERS To summarize, SDB appears to be a risk factor for stroke, and, conversely, stroke is a risk factor for SDB. However, it is unclear whether treatment of SDB reduces long-term stroke risk. SDB also is a risk factor for subsequent cardiovascular disease events after stroke. CPAP treatment of SDB after stroke may reduce that risk, but long-term adherence is difficult to achieve. Potential Pathogenetic Mechanisms of Cardiovascular Disease in Sleep-Disordered Breathing Several SDB-related mechanisms, including endothelial dysfunction, hypoxia, inflammation, obesity, metabolic dysregulation, and sympathetic activation, may influence the pathogenesis of cardiovascular disease in persons with SDB. OSA is associated with intermittent hypoxemia, consequent to intermittent upper-airway occlusion. Hypoxia and attendant hypercapnia augment sympathetic nervous system activity. Recurrent hypoxemia-re-oxygenation produces sustained hypertension in rodents, via sympathetic activation.79 The intrathoracic pressure swings and arousals associated with hypopneic and apneic events also boost sympathetic activity Intermittent hypoxemia may also be pivotal in the genesis of systemic inflammation in OSA. Intermittent hypoxemia increases the expression of transcription factors such as activator protein 1 and nuclear factor kappa 〉, which then up-regulates expression of inflammatory cytokines and adhesion molecules.80 Indeed, the circulating levels of C-reactive protein,81,82 soluble interleukin-6 receptors,83 intracellular adhesion molecule-1, and vascular-cell adhesion molecule-1 are elevated in persons with OSA.84,85 Furthermore, the propensity of monocytes to adhere to vascular endothelium is increased.86 Increased levels and adherence of inflammatory mediators contribute to atherosclerosis.87 Production, migration, and adherence of these mediators is favorably modified by OSA treatment.86,88 Additionally, hypoxia re-oxygenation, sympathetic activation, and increased lipid peroxidation amplify freeradical production.89 There is enhanced free-radical production from neutrophils and monocytes in OSA, and this ameliorates with therapy.86,90,91 Oxidant stress contributes to endothelial injury, increased production of adhesion molecules in the endothelium, diminished vasodilator production, and atherosclerosis.92 The hypoxia-regeneration, inflammation, and oxidative stress contribute to endothelial injury and, thence, vasoconstriction, hypercoagulability, and atherosclerosis.86 These pathways may constitute the mechanistic paradigm whereby OSA mediates the genesis or worsening of hypertension and other cardiovascular disorders (Fig. 1). RESPIRATORY CARE • OCTOBER 2010 VOL 55 NO 10 SLEEP-DISORDERED BREATHING AND CARDIOVASCULAR DISORDERS verse cardiovascular disorders, as well as increased mortality. Large, prospective, long-term studies will help further confirm this relationship. The current data also suggest a beneficial role of CPAP therapy in attenuating the risk of adverse cardiovascular sequelae. However, conclusive evidence of the salutary role of SDB therapy will require large randomized controlled studies designed with careful attention to the potential confounders, as well as aimed at elucidating the mechanistic pathways whereby SDB therapy provides cardiovascular benefits. REFERENCES Fig. 1. Pathogenetic mechanisms whereby sleep-disordered breathing leads to cardiovascular sequelae. (Adapted from Reference 92.) Sleep-Disordered Breathing and Excess Mortality As previously discussed, most retrospective studies indicate that OSA is a risk factor for decreased long-term survival. More recently, 3 observational cohort studies confirmed that SDB appears to increase mortality. In an 18year follow-up of the Wisconsin Sleep Cohort, the adjusted hazard ratio for all-cause mortality with severe SDB versus no SDB was 3.0, and the cardiovascular-diseasespecific hazard ratio was 5.2.93 Similarly, a 14-year follow-up of the Busselton Health Study found the fully adjusted hazard ratio for all-cause mortality associated with moderate to severe OSA was 6.24.94 However, in both studies the confidence intervals were wide and the precision of the estimate is uncertain. More recently, with an average follow-up duration of 8.2 years, the Sleep Heart Health Study found a fully adjusted hazard ratio for allcause mortality of 1.46, with much narrower confidence intervals. In addition, death in men accounted for most of the effect. Coronary-heart-disease-specific mortality showed the same pattern, and it appeared that nocturnal hypoxemia was an important mediating factor.95 Although treatment of OSA with CPAP reduced the risk of fatal and non-fatal cardiovascular events in a clinically derived observational cohort composed of only men,36 a randomized controlled trial has not been performed, so it remains to be definitively determined whether treatment of SDB reduces all-cause mortality. Summary There is compelling evidence suggesting an association, probably causal, between SDB, especially OSA, and di- RESPIRATORY CARE • OCTOBER 2010 VOL 55 NO 10 1. Tishler PV, Larkin EK, Schluchter MD, Redline S. Incidence of sleep-disordered breathing in an urban adult population: the relative importance of risk factors in the development of sleep-disordered breathing. JAMA 2003;289(17):2230-2237. 2. Fletcher EC. The relationship between systemic hypertension and obstructive sleep apnea: facts and theory. Am J Med 1995;98(2): 118-128. 3. Franklin KA, Nilsson JB, Sahlin C, Naslund U. Sleep apnoea and nocturnal angina. Lancet 1995;345(8957):1085-1087. 4. Hung J, Whitford EG, Parsons RW, Hillman DR. Association of sleep apnoea with myocardial infarction in men. Lancet 1990; 336(8710):261-264. 5. Malone S, Liu PP, Holloway R, Rutherford R, Xie A, Bradley TD. Obstructive sleep apnoea in patients with dilated cardiomyopathy: effects of continuous positive airway pressure. Lancet 1991; 338(8781):1480-1484. 6. He J, Kryger MH, Zorick FJ, Conway W, Roth T. Mortality and apnea index in obstructive sleep apnea: experience in 385 male patients. Chest 1988;94(1):9-14. 7. Partinen M, Jamieson A, Guilleminault C. Long-term outcome for obstructive sleep apnea syndrome patients. Mortality. Chest 1988; 94(6):1200-1204. 8. Gonzalez-Rothi RJ, Foresman GE, Block AJ. Do patients with sleep apnea die in their sleep? Chest 1988;94(3):531-538. 9. Fields LE, Burt VL, Cutler JA, Hughes J, Roccella EJ, Sorlie P. The burden of adult hypertension in the United States 1999 to 2000: a rising tide. Hypertension 2004;44(4):398-404. 10. Budhiraja R, Sharief I, Quan SF. Sleep-disordered breathing and hypertension. J Clin Sleep Med 2005;1(4):401-404. 11. Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med 2000;342(19):1378-1384. 12. Hla KM, Young T, Finn L, Peppard PE, Szklo-Coxe M, Stubbs M. Longitudinal association of sleep-disordered breathing and nondipping of nocturnal blood pressure in the Wisconsin Sleep Cohort Study. Sleep 2008;31(6):795-800. 13. Nieto FJ, Young TB, Lind BK, Shahar E, Samet JM, Redline S, et al. Association of sleep-disordered breathing, sleep apnea, and hypertension in a large community-based study. Sleep Heart Health Study. JAMA 2000;283(14):1829-1836. Erratum in: JAMA 2002;288(16): 1985. 14. O’Connor GT, Caffo B, Newman AB, Quan SF, Rapoport DM, Redline S, et al. Prospective study of sleep-disordered breathing and hypertension: the Sleep Heart Health Study. Am J Respir Crit Care Med 2009;179(12):1159-1164. 15. Logan A. Sleep-disordered breathing and hypertension. Am J Respir Crit Care Med 2009;179(12):1082-1083. 16. Peppard PE. Is obstructive sleep apnea a risk factor for hypertension? Differences between the Wisconsin Sleep Cohort and the Sleep Heart Health Study. J Clin Sleep Med 2009;5(5):404-405. 1327 SLEEP-DISORDERED BREATHING 17. Redline S. Does sleep disordered breathing increase hypertension risk? A practical perspective on interpreting the evidence. J Clin Sleep Med 2009;5(5):406-408. 18. Hu FB, Willett WC, Colditz GA, Ascherio A, Speizer FE, Rosner B, et al. Prospective study of snoring and risk of hypertension in women. Am J Epidemiol 1999;150(8):806-816. 19. Mehra R, Stone KL, Blackwell T, Ancoli Israel S, Dam TT, Stefanick ML, Redline S; Osteoporotic Fractures in Men Study. Prevalence and correlates of sleep-disordered breathing in older men: osteoporotic fractures in men sleep study. J Am Geriatr Soc 2007;55(9): 1356-1364. 20. Kario K, Shimada K, Pickering TG. Abnormal nocturnal blood pressure falls in elderly hypertension: clinical significance and determinants. J Cardiovasc Pharmacol 2003;41(Suppl 1):S61-S66. 21. Logan AG, Perlikowski SM, Mente A, Tisler A, Tkacova R, Niroumand M, et al. High prevalence of unrecognized sleep apnoea in drug-resistant hypertension. J Hypertens 2001;19(12):2271-2277. 22. Lavie P, Hoffstein V. Sleep apnea syndrome: a possible contributing factor to resistant. Sleep 2001;24(6):721-725. 23. Durán-Cantolla J, Aizpuru F, Martínez-Null C, Barbé-Illa F. Obstructive sleep apnea/hypopnea and systemic hypertension. Sleep Med Rev 2009;13(5):323-331. 24. Giles TL, Lasserson TJ, Smith BJ, White J, Wright J, Cates CJ. Continuous positive airways pressure for obstructive sleep apnoea in adults. Cochrane Database Syst Rev 2006;(1):CD001106. 25. Robinson GV, Smith DM, Langford BA, Davies RJ, Stradling JR. Continuous positive airway pressure does not reduce blood pressure in nonsleepy hypertensive OSA patients. Eur Respir J 2006;27(6): 1229-1235. 26. Faccenda JF, Mackay TW, Boon NA, Douglas NJ. Randomized placebo-controlled trial of continuous positive airway pressure on blood pressure in the sleep apnea-hypopnea syndrome. Am J Respir Crit Care Med 2001;163(2):344-348. 27. Pepperell JC, Ramdassingh-Dow S, Crosthwaite N, Mullins R, Jenkinson C, Stradling JR, Davies RJ. Ambulatory blood pressure after therapeutic and subtherapeutic nasal continuous positive airway pressure for obstructive sleep apnoea: a randomised parallel trial. Lancet 2002;359(9302):204-210. 28. Shibata N, Nishimura T, Hasegawa K, Hattori C, Suzuki K. Influence of sleep respiratory disturbance on nocturnal blood pressure. Acta Otolaryngol Suppl 2003;(550):32-35. 29. Budhiraja R, Quan SF. When is CPAP an antihypertensive in sleep apnea patients? J Clin Sleep Med 2009;5(2):108-109. 30. Sorajja D, Gami AS, Somers VK, Behrenbeck TR, Garcia-Touchard A, Lopez-Jimenez F. Independent association between obstructive sleep apnea and subclinical coronary artery disease. Chest 2008; 133(4):927-933. 31. Shahar E, Whitney CW, Redline S, Lee ET, Newman AB, Javier Nieto F, et al. Sleep-disordered breathing and cardiovascular disease: cross-sectional results of the Sleep Heart Health Study. Am J Respir Crit Care Med 2001;163(1):19-25. 32. Gottlieb DJ, Yenokyan G, Newman AB, O’Connor GT, Punjabi NM, Quan SF, et al. Prospective study of obstructive sleep apnea and incident coronary heart disease and heart failure: the sleep heart health study. Circulation 2010;122(4):352-360. 33. Peker Y, Hedner J, Norum J, Kraiczi H, Carlson J. Increased incidence of cardiovascular disease in middle-aged men with obstructive sleep apnea: a 7-year follow-up. Am J Respir Crit Care Med 2002; 166(2):159-165. 34. Mooe T, Franklin KA, Holmström K, Rabben T, Wiklund U. Sleepdisordered breathing and coronary artery disease: long-term prognosis. Am J Respir Crit Care Med 2001;164(10 Pt 1):1910-1913. 1328 AND CARDIOVASCULAR DISORDERS 35. Peker Y, Hedner J, Kraiczi H, Loth S. Respiratory disturbance index: an independent predictor of mortality in coronary artery disease. Am J Respir Crit Care Med 2000;162(1):81-86. 36. Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet 2005;365(9464):1046-1053. 37. Steiner S, Schueller PO, Hennersdorf MG, Behrendt D, Strauer BE. Impact of obstructive sleep apnea on the occurrence of restenosis after elective percutaneous coronary intervention in ischemic heart disease. Respir Res 2008;9:50. 38. Yumino D, Tsurumi Y, Takagi A, Suzuki K, Kasanuki H. Impact of obstructive sleep apnea on clinical and angiographic outcomes following percutaneous coronary intervention in patients with acute coronary syndrome. Am J Cardiol 2007;99(1):26-30. 39. Nakashima H, Katayama T, Takagi C, Amenomori K, Ishizaki M, Honda Y, Suzuki S. Obstructive sleep apnoea inhibits the recovery of left ventricular function in patients with acute myocardial infarction. Eur Heart J 2006;27(19):2317-2322. 40. Cassar A, Morgenthaler TI, Lennon RJ, Rihal CS, Lerman A. Treatment of obstructive sleep apnea is associated with decreased cardiac death after percutaneous coronary intervention. J Am Coll Cardiol 2007;50(14):1310-1314. 41. Milleron O, Pillière R, Foucher A, de Roquefeuil F, Aegerter P, Jondeau G, et al. Benefits of obstructive sleep apnoea treatment in coronary artery disease: a long-term follow-up study. Eur Heart J 2004;25(9):728-734. 42. Drager LF, Bortolotto LA, Figueiredo AC, Krieger EM, Lorenzi GF. Effects of continuous positive airway pressure on early signs of atherosclerosis in obstructive sleep apnea. Am J Respir Crit Care Med 2007;176(7):706-712. 43. Steiropoulos P, Tsara V, Nena E, Fitili C, Kataropoulou M, Froudarakis M, et al. Effect of continuous positive airway pressure treatment on serum cardiovascular risk factors in patients with obstructive sleep apnea-hypopnea syndrome. Chest 2007;132(3):843-851. 44. Peker Y, Glantz H, Thunstrom E, Kallryd A, Herlitz J, Ejdeback J. Rationale and design of the Randomized Intervention with CPAP in Coronary Artery Disease and Sleep Apnoea (RICCADSA) trial. Scand Cardiovasc J 2009;43(1):24-31. 45. Khayat RN, Jarjoura D, Patt B, Yamokoski T, Abraham WT. Inhospital testing for sleep-disordered breathing in hospitalized patients with decompensated heart failure: report of prevalence and patient characteristics. J Card Fail 2009;15(9):739-746. 46. Oldenburg O, Lamp B, Faber L, Teschler H, Horstkotte D, Topfer V. Sleep-disordered breathing in patients with symptomatic heart failure: a contemporary study of prevalence in and characteristics of 700 patients. Eur J Heart Fail 2007;9(3):251-257. 47. Paulino A, Damy T, Margarit L, Stoïca M, Deswarte G, Khouri L, et al. Prevalence of sleep-disordered breathing in a 316-patient French cohort of stable congestive heart failure. Arch Cardiovasc Dis 2009; 102(3):169-175. 48. Schulz R, Blau A, Börgel J, Duchna HW, Fietze I, Koper I, et al. Sleep apnoea in heart failure. Eur Respir J 2007;29(6):1201-1205. 49. Javaheri S, Parker TJ, Liming JD, Corbett WS, Nishiyama H, Wexler L, Roselle GA. Sleep apnea in 81 ambulatory male patients with stable heart failure: types and their prevalences, consequences, and presentations. Circulation 1998;97(21):2154-2159. 50. Javaheri S, Shukla R, Zeigler H, Wexler L. Central sleep apnea, right ventricular dysfunction, and low diastolic blood pressure are predictors of mortality in systolic heart failure. J Am Coll Cardiol 2007; 49(20):2028-2034. 51. Sin DD, Fitzgerald F, Parker JD, Newton G, Floras JS, Bradley TD. Risk factors for central and obstructive sleep apnea in 450 men and RESPIRATORY CARE • OCTOBER 2010 VOL 55 NO 10 SLEEP-DISORDERED BREATHING 52. 53. 54. 55. 56. 57. 58. 59. 60. 61. 62. 63. 64. 65. 66. 67. 68. 69. women with congestive heart failure. Am J Respir Crit Care Med 1999;160(4):1101-1106. Hanly PJ, Zuberi-Khokhar NS. Increased mortality associated with Cheyne-Stokes respiration in patients with congestive heart failure. Am J Respir Crit Care Med 1996;153(1):272-276. Lanfranchi PA, Somers VK, Braghiroli A, Corra U, Eleuteri E, Giannuzzi P. Central sleep apnea in left ventricular dysfunction: prevalence and implications for arrhythmic risk. Circulation 2003;107(5): 727-732. Kaneko Y, Floras JS, Usui K, Plante J, Tkacova R, Kubo T, et al. Cardiovascular effects of continuous positive airway pressure in patients with heart failure and obstructive sleep apnea. N Engl J Med 2003;348(13):1233-1241. Mansfield DR, Gollogly NC, Kaye DM, Richardson M, Bergin P, Naughton MT. Controlled trial of continuous positive airway pressure in obstructive sleep apnea and heart failure. Am J Respir Crit Care Med 2004;169(3):361-366. Javaheri S. Effects of continuous positive airway pressure on sleep apnea and ventricular irritability in patients with heart failure. Circulation 2000;101(4):392-397. Bitter T, Faber L, Hering D, Langer C, Horstkotte D, Oldenburg O. Sleep-disordered breathing in heart failure with normal left ventricular ejection fraction. Eur J Heart Fail 2009;11(6):602-608. Cloward TV, Walker JM, Farney RJ, Anderson JL. Left ventricular hypertrophy is a common echocardiographic abnormality in severe obstructive sleep apnea and reverses with nasal continuous positive airway pressure. Chest 2003;124(2):594-601. Laaban JP, Pascal-Sebaoun S, Bloch E, Orvoen-Frija E, Oppert JM, Huchon G. Left ventricular systolic dysfunction in patients with obstructive sleep apnea syndrome. Chest 2002;122(4):1133-1138. Bradley TD, Logan AG, Kimoff RJ, Sériès F, Morrison D, Ferguson K et al; CANPAP Investigators. Continuous positive airway pressure for central sleep apnea and heart failure. N Engl J Med 2005;353(19): 2025-2033. Naughton MT, Lorenzi-Filho G. Sleep in heart failure. Prog Cardiovasc Dis 2009;51(4):339-349. Garrigue S, Bordier P, Jaïs P, Shah DC, Hocini M, Raherison C, et al. Benefit of atrial pacing in sleep apnea syndrome. N Engl J Med 2002;346(6):404-412. Erratum in: N Engl J Med 2002;346(11):872. Simantirakis EN, Schiza SE, Chrysostomakis SI, Chlouverakis GI, Klapsinos NC, Siafakas NM, Vardas PE. Atrial overdrive pacing for the obstructive sleep apnea-hypopnea syndrome. N Engl J Med 2005; 353(24):2568-2577. Krahn AD, Yee R, Erickson MK, Markowitz T, Sula LJ, Klein GJ, et al. Physiologic pacing in patients with obstructive sleep apnea: a prospective, randomized crossover trial. J Am Coll Cardiol 2006; 47(2):379-383. Melzer C, Fietze I, Duru F, Glos M, Lemola K, Bloch K, et al. Nocturnal overdrive pacing for the treatment of sleep apnea syndrome. Sleep 2006;29(9):1197-1202. Gabor JY, Newman DA, Barnard-Roberts V, Korley V, Mangat I, Dorian P, Hanly PJ. Improvement in Cheyne-Stokes respiration following cardiac resynchronisation therapy. Eur Respir J 2005;26(1): 95-100. Lüthje L, Renner B, Kessels R, Vollmann D, Raupach T, Gerritse B, et al. Cardiac resynchronization therapy and atrial overdrive pacing for the treatment of central sleep apnoea. Eur J Heart Fail 2009; 11(3):273-280. Mehra R, Benjamin EJ, Shahar E, Gottlieb DJ, Vawabit R, Kirchner HL, et al. Association of nocturnal arrhythmias with sleep-disordered breathing: the Sleep Heart Health Study. Am J Respir Crit Care Med 2006;173(8):910-916. Mehra R, Stone KL, Varosy PD, Hoffman AR, Marcus GM, Blackwell T, et al. Nocturnal arrhythmias across a spectrum of obstructive RESPIRATORY CARE • OCTOBER 2010 VOL 55 NO 10 AND CARDIOVASCULAR DISORDERS 70. 71. 72. 73. 74. 75. 76. 77. 78. 79. 80. 81. 82. 83. 84. 85. 86. 87. and central sleep-disordered breathing in older men: outcomes of sleep disorders in older men (MrOS sleep) study. Arch Intern Med 2009;169(12):1147-1155. Garrigue S, Pépin JL, Defaye P, Murgatroyd F, Poezevara Y, Clémenty J, Lévy P. High prevalence of sleep apnea syndrome in patients with long-term pacing: the European Multicenter Polysomnographic Study. Circulation 2007;115(13):1703-1709. Monahan K, Storfer-Isser A, Mehra R, Shahar E, Mittleman M, Rottman J, et al. Triggering of nocturnal arrhythmias by sleep-disordered breathing events. J Am Coll Cardiol 2009;54(19):1797-1804. Gami AS, Howard DE, Olson EJ, Somers VK. Day-night pattern of sudden death in obstructive sleep apnea. N Engl J Med 2005;352(12): 1206-1214. Kanagala R, Murali NS, Friedman PA, Ammash NM, Gersh BJ, Ballman KV, et al. Obstructive sleep apnea and the recurrence of atrial fibrillation. Circulation 2003;107(20):2589-2594. Dyken ME, Im KB. Obstructive sleep apnea and stroke. Chest 2009; 136(6):1668-1677. Yaggi HK, Concato J, Kernan WN, Lichtman JH, Brass LM, Mohsenin V. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med 2005;353(19):2034-2041. Arzt M, Young T, Finn L, Skatrud JB, Bradley TD. Association of sleep-disordered breathing and the occurrence of stroke. Am J Respir Crit Care Med 2005;172(11):1447-1451. Redline S, Yenokyan G, Gottlieb DJ, Shahar E, O’Connor GT, Resnick HE, et al. Obstructive sleep apnea hypopnea and incident stroke: the Sleep Heart Health Study. Am J Respir Crit Care Med 2010;182(2): 269-277. Martínez-García MA, Soler-Cataluña JJ, Ejarque-Martinez L, Soriano Y, Román-Sánchez P, Illa FB, et al. Continuous positive airway pressure treatment reduces mortality in patients with ischemic stroke and obstructive sleep apnea: a 5-year follow-up study. Am J Respir Crit Care Med 2009;180(1):36-41. Fletcher EC. Physiological consequences of intermittent hypoxia: systemic blood pressure. J Appl Physiol 2001;90(4):1600-1605. Ryan S, Taylor CT, McNicholas WT. Systemic inflammation: a key factor in the pathogenesis of cardiovascular complications in obstructive sleep apnoea syndrome? Thorax 2009;64(7):631-636. Shamsuzzaman AS, Winnicki M, Lanfranchi P, Wolk R, Kara T, Accurso V, Somers VK. Elevated C-reactive protein in patients with obstructive sleep apnea. Circulation 2002;105(21):2462-2464. Larkin EK, Rosen CL, Kirchner HL, Storfer-Issner A, Emancipator JL, Johnson NL, et al. Variation of C-reactive protein levels in adolescents: association with sleep-disordered breathing and sleep duration. Circulation 2005;111(15):1978-1984. Mehra R, Storfer-Isser A, Kirchner HL, Johnson N, Jenny N, Tracy RP, Redline S. Soluble interleukin 6 receptor: a novel marker of moderate to severe sleep-related breathing disorder. Arch Intern Med 2006;166(16):1725-1731. Ohga E, Nagase T, Tomita T, Teramoto S, Matsuse T, Katayama H, Ouchi Y. Increased levels of circulating ICAM-1, VCAM-1, and L-selectin in obstructive sleep apnea syndrome J Appl Physiol 1999; 87(1):10-14. El-Solh AA, Mador MJ, Sikka P, Dhillon RS, Amsterdam D, Grant BJ. Adhesion molecules in patients with coronary artery disease and moderate-to-severe obstructive sleep apnea. Chest 2002;121(5):15411547. Dyugovskaya L, Lavie P, Lavie L. Increased adhesion molecules expression and production of reactive oxygen species in leukocytes of sleep apnea patients. Am J Respir Crit Care Med 2002;165(7): 934-939. Price DT, Loscalzo J. Cellular adhesion molecules and atherogenesis. Am J Med 1999;107(1):85-97. 1329 SLEEP-DISORDERED BREATHING 88. Yokoe T, Minoguchi K, Matsuo H, Oda N, Minoguchi H, Yoshino G, et al. Elevated levels of C-reactive protein and interleukin-6 in patients with obstructive sleep apnea syndrome are decreased by nasal continuous positive airway pressure. Circulation 2003;107(8):1129-1134. 89. Zhang GX, Kimura S, Nishiyama A, Shokoji T, Rahman M, Yao L, et al. Cardiac oxidative stress in acute and chronic isoproterenolinfused rats. Cardiovasc Res 2005;65(1):230-238. 90. Schulz R, Mahmoudi S, Hattar K, Sibelius U, Olschewshi H, Mayer K, et al. Enhanced release of superoxide from polymorphonuclear neutrophils in obstructive sleep apnea: impact of continuous positive airway pressure therapy. Am J Respir Crit Care Med 2000;162(2 Pt 1):566-570. 91. Deanfield J, Donald A, Ferri C, Giannattasio C, Halcox J, Halligan S, et al. Endothelial function and dysfunction. Part I: Methodological Discussion Kapur: Stuart, a lot of people accept the fact that OSA is a cause of hypertension, but when we’re talking about coronary disease, congestive heart failure, or stroke, where do you think we are on the continuum to proving causation. If we’re not there yet, what needs to be done to able to make that statement about these other relationships? Quan: I think it would be good to have more data on women and various other segments of the population. In hypertension there are a lot of (albeit small) clinical studies where they used CPAP and found a decrease in blood pressure or they used less drug. In coronary heart disease we don’t have good data to show that CPAP does a lot. There is the Marin study1 and the Yaggi study,2 but neither were randomized controlled studies. I don’t like the Yaggi study because they used a combined outcome variable of stroke or death, and I think that’s very messy. So was it stroke or death? Anyway, I think that we need interventional studies to demonstrate that doing something is important. We also need to determine if some segments of the population are more susceptible to the adverse cardiovascular impact of sleep apnea. 1. Marin JM, Carrizo SJ, Vincente E, Agusti AG. Long-term cardiovascular outcomes in 1330 AND CARDIOVASCULAR DISORDERS 92. 93. 94. 95. issues for assessment in the different vascular beds: a statement by the Working Group on Endothelin and Endothelial Factors of the European Society of Hypertension. J Hypertens 2005;23(1):7-17. Budhiraja R, Parthasarathy S, Quan SF. Endothelial dysfunction in obstructive sleep apnea. J Clin Sleep Med 2007;3(4):409-415. Young T, Finn L, Peppard PE, Szklo-Coxe M, Austin D, Nieto FJ, et al. Sleep-disordered breathing and mortality: eighteen-year follow-up of the Wisconsin Sleep Cohort. Sleep 2008;31(8):1071-1078. Marshall NS, Wong KK, Liu PY, Cullen SR, Knuiman MW, Grunstein RR. Sleep apnea as an independent risk factor for all-cause mortality: the Busselton Health Study. Sleep 2008;31(8):1079-1085. Punjabi NM, Caffo BS, Goodwin JL, Gottlieb DJ, Newman AB, O’Connor GT, et al. Sleep-disordered breathing and mortality: a prospective cohort study. PLoS Med 2009;6(8):e1000132. men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet 2005;365(9464): 1046-1053. 2. Yaggi HK, Concato J, Kernan WN, Lichtman JH, Brass LM, Mohsenin V. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med 2005;353(19): 2034-2041. Owens: In the study you showed with the C-reactive protein data,1 it seemed that the patients who were nonadherent had a lower C-reactive protein level at the start of the trial, but at the end of the trial their C-reactive protein was about the same as those who had been adherent to treatment. Is C-reactive protein a marker of symptoms from the disease? And can we use it to predict who might symptomatically benefit from treatment and therefore will probably be adherent to therapy? Or can we use biomarkers to predict who needs to be treated? 1. Steiropoulos P, Tsara V, Nena E, Fitili C, Kataropoulou M, Froudarakis M, et al. Effect of continuous positive airway pressure treatment on serum cardiovascular risk factors in patients with obstructive sleep apnea-hypopnea syndrome. Chest 2007; 132(3):843-851. Quan: That’s why we’re doing the HeartBEAT study.1 About the Chest article,2 as a clinician reading that sort of paper you say, “Oh yeah, they had a large number of people,” but to an epidemiologist that’s puny. Those differences in C-reactive protein between people who refused and people who got treated weren’t significant, but if they studied 1,000 people, they have might been significant. It’s hard to know. 1. Redline S. Phase II trial of sleep apnea treatment to reduce cardiovascular morbidity. http://projectreporter.nih.gov/project_info _description.cfm?aid⫽7853407. Accessed June 24, 2010. 2. Steiropoulos P, Tsara V, Nena E, Fitili C, Kataropoulou M, Froudarakis M, et al. Effect of continuous positive airway pressure treatment on serum cardiovascular risk factors in patients with obstructive sleep apnea-hypopnea syndrome. Chest 2007; 132(3):843-851. Malhotra: It’s easy for those of us who were not on the scene in the mid1990s to criticize. Some say that we should have designed the Sleep Heart Health Study differently so that there wasn’t a survivor cohort; they were older, asymptomatic, and there wasn’t a lot of disease there. Wasn’t the primary outcome all-cause mortality in all comers? Quan: That was one of them. We had a number of what we called primary hypotheses. One was all causes of mortality, and another was cardiovascular disease, among others. Malhotra: My understanding is that the age over 70 or under 70 was not pre-specified and that was sort of just based on results. Is that right? And gen- RESPIRATORY CARE • OCTOBER 2010 VOL 55 NO 10 SLEEP-DISORDERED BREATHING der stratification was a secondary outcome? Quan: That was brought up by one of the reviewers for PLoS [Public Library of Science] Medicine, in looking at whether age of death was a prespecified outcome variable. Malhotra: But the 70 cut-off wasn’t? Quan: No, but we had to put a cutoff somewhere. We had tried a few other cut-off points and it didn’t matter too much. Malhotra: If you had to redesign that study, what would you do differently? Quan: Basically recruit an entire new cohort. Malhotra: Not a survivor cohort? Quan: Not a survivor cohort, but the cohort we used was recruited for financial reasons. The National Institutes of Health wanted to do an observational cohort study. The Sleep Heart Health Study,1 all told, in direct costs was probably $20 million. Observational cohort studies are very expensive, and so they felt that they could reduce the costs by strapping a study onto other studies. They basically came up with the design that’s been used subsequently by several other cohort studies. 1. Quan SF, Howard BV, Iber C, Kiley JP, Nieto FJ, O’Connor GT, et al. The Sleep Heart Health Study: design, rationale, and methods. Sleep 1997;20(12):1077-1085. Malhotra: Would it have been cheaper if you didn’t have to go 8 years? For example, if you had a bigger sample with more events, could you have after 4 years—which was the original design? Quan: It’s possible, but I think that although the Wisconsin cohort was much smaller,1 their mortality data are AND CARDIOVASCULAR DISORDERS out a long time too. Terry Young’s confidence intervals in the mortality study were very wide,2 which means that the precision was very low. 1. Young T, Palta M, Dempsey J, Peppard PE, Nieto FJ, Hla KM. Burden of sleep apnea: rationale, design, and major findings of the Wisconsin Sleep Cohort study. WMJ 2009;108(5):246-249. 2. Young T, Finn L, Peppard PE, Szklo-Coxe M, Austin D, Nieto FJ, et al. Sleep-disordered breathing and mortality: eighteenyear follow-up of the Wisconsin sleep cohort. Sleep 2008;31(8):1071-1078. Malhotra: Terry Young’s study was in a community cohort as well, right? I’m wondering if you wouldn’t have had a more symptomatic, more affected group and a bigger sample and not needed 18 years of follow-up? I don’t know. Quan: That’s possible. If I were to design this again and money was no object, I would recruit a huge cohort, more along the size of the Women’s Health Initiative.1 And it would include people who were nonsymptomatic. Obviously, by having such a huge cohort you would have symptomatic and non-symptomatic individuals. You would answer the question, which symptoms are important? You’d have a wide spectrum. I say we need to do a birth cohort study like the National Children’s Study. 2 That would be ideal. We then could wait for about 40 years for some answers. 1. Women’s Health Initiative Study Group. Design of the women’s health initiative clinical trial and observational study. Control Clin Trials 1998;19:61-109. 2. The National Children’s Study. http://www. nationalchildrensstudy.gov/about/ overview/pages/default.aspx. Accessed June 24, 2010. Malhotra: I talked to the Nurses’ Health Study (http://www.channing. harvard.edu/nhs) people. They prospectively followed 100,000 women. You can’t do it for less than $100 million unless you have some kind of substandard diagnostic technique. RESPIRATORY CARE • OCTOBER 2010 VOL 55 NO 10 Quan: It is very hard to do these studies inexpensively. You could cut down by doing a limited sleep study. However, the spinoff on these cohort studies is that the Sleep Heart Health Study has published more than 50 papers, many of which don’t relate to the primary hypothesis at all, because we accumulated all this information. If we had not done EEG [electroencephalography], we would not have had those data on arousals, for example. Kapur: Stuart, given the data you presented on higher cardiovascular risk and higher potential cardiovascular mortality in an observational cohort, particularly in men and those who have more severe apnea, are there ethical limits on what kind of randomized clinical trials we can do? This is the sort of issue that people who design the studies interact with IRBs [institutional review boards] about. The IRB will ask questions like, “Don’t we know this already?” How can you randomize a patient with severe apnea to CPAP versus placebo? Quan: You have to ask whether there’s equipoise. Certainly, you can do it for 6 months or longer. In the APPLES study1 we had a sham arm of 6 months, and the amount of time from when people were first identified for possible recruitment to when they finished the study was probably in excess of 8 months. Most of those people have had the condition for a long time. You could argue that every second counts and you’ve got to get them treated, but that’s not going to answer your question. 1. Kushida CA, Nichols DA, Quan SF, Goodwin JL, White DP, Gottlieb DJ, et al. The apnea positive pressure long-term efficacy study (APPLES): rationale, design, methods, and procedures. J Clin Sleep Med 2006; 2(3):288-300. Gay: I was thinking about that when I saw you had an oxygen arm in that. Are you worried that you might make them worse with oxygen, by prolong- 1331 SLEEP-DISORDERED BREATHING AND CARDIOVASCULAR DISORDERS ing apneas in someone with severe apneas? Oxygen isn’t the standard of care anywhere for OSA, so I’m curious how you got to that oxygen arm. Quan: The mortality data are in PLoS Medicine.1 The cardiovascular data2 are under revision, hopefully the last revision. Quan: The oxygen was put in there because of our data from the Sleep Heart Health Study1 that hypoxemia appears to be factor responsible for the increase in cardiovascular disease with sleep apnea. Some data indicate that oxygen might prolong the apneas. However, there are some exclusions from HeartBEAT for people with very bad sleep apnea.2 I’ve also given oxygen in the clinic to people who have refused to wear CPAP, and they did not appear to get worse. 1. Punjabi NM, Caffo BS, Goodwin JL, Gottlieb DJ, Newman AB, O’Connor GT, et al. Sleep-disordered breathing and mortality: a prospective cohort study. PLoS Med 2009;6(8):e1000132. 2. Gottlieb DJ, Yenokyan G, Newman AB, O’Connor GT, Punjabi NM, Quan SF, Redline S, et al. Prospective study of obstructive sleep apnea and incident coronary heart disease and heart failure: the sleep heart health study. Circulation 2010;122(4):352360. 1. Punjabi NM, Caffo BS, Goodwin JL, Gottlieb DJ, Newman AB, O’Connor GT, et al. Sleep-disordered breathing and mortality: a prospective cohort study. PLoS Med 2009;6(8):e1000132. 2. Redline S. Phase II trial of sleep apnea treatment to reduce cardiovascular morbidity. http: // projectreporter.nih.gov / project_info_ description.cfm?aid⫽7853407. Accessed June 24, 2010. Gay: We all have. Quan: So I don’t worry too much about that, personally. Mokhlesi: How do you translate this? And I assume that some of the data from the Sleep Heart Health Study has not been published yet. 1332 Mokhlesi: I understand the importance of population-based studies, but what do you do when you have a woman who is 50 years old and has severe OSA with an AHI of 50? At the end of the day, we don’t treat populations, we treat patients. How do we connect these? Do you think there’s a danger of people in the community interpreting these data and saying that a 50-year-old woman with an AHI of 50 shouldn’t even get treated, because there’s no mortality benefit? Quan: Even if sleep apnea wasn’t a risk factor for any subsequent disease, if the person is symptomatic, it’s reasonable to treat them. But what about a person with an AHI of 50 but they’re asymptomatic? I don’t think the data are conclusive enough to say that I wouldn’t treat that individual. I might point out to the person that perhaps it’s a little unclear, but I think that they might want to give this a try. Malhotra: I think that’s the most important point. In the Sleep Heart Health Study there are very few women in their 50s with AHIs in the 50s. I think people are drawing conclusions that aren’t supported by the data. Quan: Absolutely. Parthasarathy: Are there gender differences in biomarkers? Quan: I don’t know. I have no doubt that there probably are differences, but I haven’t completely reviewed that literature yet. Malhotra: Which biomarkers? Parthasarathy: Any. Malhotra: We have done vascular studies in a cohort of obese OSA patients and matched controls, and have seen some gender differences. Parthasarathy: You mean that the augmentation makes a difference? Malhotra: We have some data that are not yet published. RESPIRATORY CARE • OCTOBER 2010 VOL 55 NO 10