Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
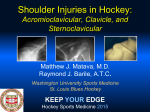
RETROSTERNAL DISLOCATION C. JOHN From Dislocation of the than fracture the literature. completely, symptoms, the Division KENNEDY, TORONTO, of Orthopaedic clavicle, either Surgery, at the ; and retrosternal dislocation Standard text-books on or dismiss it in a few lines. and the grave A youth, seventeen March 18, 1948. Four OF potentialities, THE CLAVICLE CANADA Toronto acromial General or Hospital sternal end, is much less common is so unusual that there is little reference to it in fractures and dislocations ignore the condition The rarity of the injury, the typical signs and have prompted years of age, was days before admission presentation admitted he was to the scuffling of this case. Toronto General Hospital with a group of boys and on fell to the ground. As he lay on his left side, supporting his weight on the left shoulder, another boy fell on his right shoulder. He felt a painful buckling sensation at the inner end of the left clavicle. The limb was immobilised in a figure-of-eight bandage. During the next three days he complained of severe in his throat, life, he snored and difficulty when asleep. clavicle generalised with pain in the region of the in swallowing. His Physical examination swelling. There was sterno-clavicular joint, mother noted that, for showed discolouration the difficulty in palpating the a tight feeling first time in his of skin over the sternal end of the bone which is usually so prominent. Attempted abduction of the limb, whether active passive, gave rise to severe pain in the region of the sterno-clavicular joint. Radiographic examination confirmed the clinical diagnosis of retrosternal dislocation (Fig. 1). The next clavicle, mastoid tissues, of the and tearing joint. Even on the forcibly into day, at operation, crossing the was divided. a transverse sterno-clavicular There was bone at clavicle for two as the junction described months, after Discussion-The sternum relatively invites clavicle made over the medial end of the by which inner end inner of and sterni, by fascial Bankart time therefore grasped its normal position. the wire thirds, middle threaded The was clavicle limb was immobilised and lifted introduced across and left protruding at the lateral sutures passed through drill-holes (1938). the with bone forceps A Compere wire was was the sterno- extremity in the in of sternum a plaster spica removed. is attached firmly by strong ligaments to the and first rib. The capsule, strong in its anterior and posterior distribution, is thin in the superior and inferior areas. The oblique plane of the joint almost dislocation, and it is the strength of the costo-clavicular ligament, anchoring the to the first rib, which protects it. This ligament must necessarily be torn in dislocation of the Retrosternal joint. dislocation may occur from direct or indirect violence. Examples types of injury have been recorded. In one case the patient was kicked by a mule. the injury was a blow on the lateral aspect of the shoulder (Greenlee 1944). now of the Part of the clavicular head of the left sternoof the joint, haemorrhage into surrounding of the capsule. The articular disc was still attached to the sternal part under direct vision it was not possible to reduce the dislocation by pulling clavicular joint into the manubrium the incision. Repair was reinforced and was joint. disruption abducted limb. The clavicle from beneath the sternum into the incision or reported the injury In establishing the was due diagnosis to indirect the of both In another In the case violence. history is often of assistance, particularly when, after direct or indirect injury to the sterno-clavicular limitation of abduction of the limb, dysphagia, joint, there is local pain and tenderness, snoring due to tracheal pressure, and evidence on physical prominence examination of loss The diagnosis is confirmed projections, stereograms, and The fortunate. 74 potentialities Death has of the normal by radiographic laminograms. of this dislocation been recorded from of the examination are so great that tracheal laceration. THE medial which the JOURNAL should rarity There OF end of the include of the injury is also danger BONE AND JOINT clavicle. oblique is indeed of injury SURGERY RETROSTERNAL to the great caused personal case were vessels the death of the of superior Manipulative reduction now it was exposed successful, has dispatch oesophagus by been I admission THE with haemothorax-a at in the few in which The 1944 also degree which (Dewar, F. P., In the be involved. is seldom by cases complication in might limbs dislocation redisplacement. I,) Njimegan duct abducted the CLAVICLE rider thoracic on the to reduce Moreover, usually and traction impossible at operation. there Army The OF mediastinum a Canadian communication). reported DISLOCATION successful. traction even closed when reduction of damage to the parts has joint been capsule FIG. Radiograph appear taken show to scrutiny Ofl no reveals might ahnormalit, that tile at l)Ilt left clavicle higher and more medial position The inset shows diagrammatically operation, and emphasizes the Iirst sight more close 1S ridIng at the right. thall the hudings joint disruption. at and extra-articular ligaments is such that Sometimes the sternal end of the clavicle has to the sternum. In this case, fascial repair Summary-Retrosternal a dislocation of reconstructive been removed. with internal the clavicle complications may arise from damage to the trachea, the oesophagus, and the thoracic duct. Operative ligaments is the most reliable treatment. Acknowledgment and Chief is made of the to Division Dr R. I. Harris, of Orthopaedic Associate Surgery Professor of the Toronto surgery In other fixation is an the great reduction is usually indicated. cases it has been fused was successful. unusual injury. of Surgery General in the Hospital, University for his helpful REFERENCES A. BANKART, R. BROWN, VOL. 31 B, NO. H. M. 1, (1927): D. GREENLEE, LEE, S. BLUNDELL P. (1937): FEBRUARY (1938): Surgical (1944): Journal Minnesota 1949 British Clinics of Journal North of the America, American 1\Iedicine, 20, 480. of Surgery, 26, 320. 7, 1263. Medical Serious vessels of the mediastinum, and reconstruction of Association, 125, 426. of Toronto, criticism. the