Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Epidemiology wikipedia , lookup
Gene therapy of the human retina wikipedia , lookup
Declaration of Helsinki wikipedia , lookup
Public health genomics wikipedia , lookup
Gene therapy wikipedia , lookup
Clinical trial wikipedia , lookup
Theralizumab wikipedia , lookup
Placebo-controlled study wikipedia , lookup
Alzheimer's disease research wikipedia , lookup
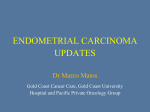
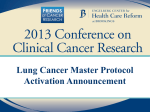
Clinical Trial Endpoint Selection in Oncology: What Can Make a Difference? James CH Yang, MD, PhD Conflicts of Interest • James Chih-Hsin Yang received honoraria for speeches or for participated in compensated advisory boards of Boehringer Ingelheim, Eli Lilly, Bayer, Roche/Genentech/Chugai, Astellas, MSD, Merck Serono, Pfizer, Novartis, Clovis Oncology, Celgene, Merrimack, Yuhan Pharmaceuticals, BMS, and Ono Pharmaceutical, and uncompensated advisory board of AstraZeneca Outline • Brief overview of regulatory authorities and their approval processes • Brief discussion of regulatory perspectives on clinical trial endpoints What Makes a Good Endpoint? CHARACTERISTIC MEANING Relevant Clinically important/useful Quantifiable Measured on an appropiate scale Valid Measures the intended effect Objective Interpreted effect yields consistent measurements Reliable Same effect yields consistent measurements Sensitive Respond to small changes in effect Specific Unaffected by extraneous influences Precise Small variability Other Tradition, cost, time… Surrogate endpoint : firmly established endpoint to predict a clinically meaningful outcome or to predict an established endpoint Clinical Trial Endpoint Selection in Last Two Decades • Strict legal requirements to demonstrate benefit – Randomised controlled trials (how many are necessary?) – Primary endpoint: Valid and reliable measure that provides the most clinically relevant and convincing evidence – Wrong design or lack of efficacy the most important reason for rejection • The commonly used endpoints are based on OS: Historically viewed as the most effective way, as it addresses biology of tumour and the natural history of the disease SURVIVAL TUMOUR RESPONSE SYMPTOM ASSESSMENT OS = overall survival; PFS = progression-free survival. PFS: Progression is associated with tumour growth, assesses tumour shrinkage and stabilisation of disease • Response rate: Objective demonstration of drug effect, durability of response is also taken into consideration • Breakthrough designation and fast tract approval are usually based on tumour response Clinical Trial Endpoint Selection in Phase III Trials • Statistically significant • Clinically meaningful Phase III, confirmatory studies, interim analyses/data maturity • OS as primary endpoint, not response rate • Possible: PFS when clinically relevant, symptom control, or could be viewed as a surrogate of OS benefit when OS difference cannot be achieved due to crossover, or long-term waiting • Reflective of patient benefit – Survival – Progression-free survival (PFS) plus some measure of symptom relief or quality of life (QoL) – Symptom relief For accelerated approval: must predict clinical benefit over available therapy – QoL • Overall response rate and response duration have been the most commonly • Surrogate endpoints • used surrogate endpoint in accelerated approval PFS is also acceptable under some conditions OS: Still the Gold Standard for Demonstrating Clinical Benefit • OS should be the primary endpoint in most phase III trials • If OS is a secondary endpoint, trials should be better powered for assessing survival ACCURATE NOT PRONE TO INVESTIGATOR OR ASSESSMENT BIAS OBJECTIVE “Overall survival is accepted as the gold standard for efficacy evaluation in clinical trials of oncology agents.” Soria JC, Massard C, Le Chevalier T. Ann Oncol. 2010;21:2324. READILY COMPARED ACROSS DISEASES CLINICALLY SIGNIFICANT UNAMBIGUOUS Cheema and Burkes. Curr Oncol. 2013;20:e150-60. EASILY MEASURED Advanced NSCLC: Why Overall Survival? In Advanced NSCLC • Most relevant to patient • Most objective endpoint – Clear and accurate endpoint – Usually easy to get this information • Relevant for other reasons – It is easier to decide upon a treatment when its impact on survival is known – Reimbursement issues – Assessment in earlier disease stages – Impact on drug development in general OS as primary end point (or powered for survival) − − − Adjuvant chemotherapy trials; eg, IALT Chemoradiotherapy in NSCLC stage III Most phase lll trials in advanced NSCLC • Pemetrexed • Bevacizumab (ECOG); Cetuximab (FLEX); Necitumumab (SQUIRE) • Maintenance trials (pemetrexed, erlotinib, gefitinib) • Nintedanib • Ramucirumab • Nivolumab • Pembrolizumab A Trial That Looks for OS… • • • • • Takes too long Requires large sample sizes Is influenced by post-trial therapy if subsequent treatments are effective or detrimental Is complex to analyse if there are too many salvage agents after trials Is more expensive • Reminder: – RCTs only require large sample sizes when one is looking for small treatment effects – Larger trials can stop early with formal interim analysis if the treatment effect is surprisingly large, and can also be stopped early if the success possibility is too low (futility) Korn E. J Clin Oncol. 2012. Overall Survival Challenges • Magnitude of the benefit – Hazard ratio of 0.7-0.8 – Median benefit of 2-3 months – Should be realistic and achievable • Impact of further treatment (post-study therapy) – Cannot be excluded – Treatment lines beyond first line have fewer benefits – No major imbalances in subsequent treatments among the arms in large phase lll trials • Role of crossover – Is it really unethical to avoid crossover ? ASCO Consensus: “OS Endpoint Is Important” • OS is a feasible endpoint, though the OS benefit may be clouded by subsequent therapies • Clinical trials should aim to improve OS by >25% ASCO stresses the use of the OS endpoint. Agents not expected to provide such OS gain would no longer be needed in clinical practice. • Consensus (esp. the degree of benefit or HR) was arbitrarily determined by a sample of clinical investigators, patient advocates, biostatisticians, US FDA oncologists, industry oncologists. However, there is a lack of the sampling process and a demonstration that the expert panel is representative of the general user or beneficiaries of the treatment (excluding the financial beneficiaries). http://www.asco.org/practice-research/clinically-meaningful-outcomes ASCO Consensus: “OS Endpoint Is Important” • OS is a feasible endpoint, though the OS benefit may be clouded by subsequent therapies • Clinical trials should aim to improve OS by >25%: Agents not expected to provide such OS gain would no longer be needed in clinical practice Ellis et al. J Clin Oncol. 2014. ASCO Consensus: “OS Endpoint Is Important”? Exceptions “Although OS was selected as the primary end point by all working groups, this does not diminish the value of progression-free survival (PFS) and other surrogate end points as valid end points in certain clinical situations. “We are now able to identify secondary mutations that drive tumor growth after progression during first-line targeted therapies. Although this information provides an opportunity for success in second-line therapies, it also makes OS a more difficult end point to attain. Thus, the use of PFS as a clinically meaningful end point may be appropriate in particular disease settings and has, in fact, been accepted by regulatory authorities on many occasions already.” http://www.asco.org/practice-research/clinically-meaningful-outcomes How Recent New Agents Granted Approval in NSCLC? US FDA’s Decision OS Docetaxel X Pemetrexed X PFS 2nd L vs placebo, HR:0.484, +2.4M RR, RD +3.9 wks Non-inferiority X Gefitinib Erlotinib X 2nd L vs placebo, HR:0.7, +2M Afatinib Bevacizumab First line, non-inferiority X X (1st L) No OS benefit shown in 1st line EGFR mut X (1st L) OS benefit only in subset (EGFR del19) HR: 0.77, +2.3M Only in one study X Crizotinib No OS benefit shown, orphan drug designation No OS benefit shown Ceritinib X No OS benefit shown Alectinib X No OS benefit shown Osimertinib X Accelerated approval Necitumumab X HR: 0.84, +1.6M +0.2M Ramucirumab X HR: 0.86, +1.4M +1.5M Nintedanib X HR: 0.75, +3 M (subset) +0.7M (ITT) Nivolumab X HR: 0.59, +3.2M (CM017) HR: 0.73, +2.8M (CM057) Pembrolizumab X HR: 0.61, +4.2M (10 mg/kg) HR: 0.71, +1.9M (2 mg/kg) Subset (adeno, progression <9M) Accelerated approval first in PDL1+ OS: overall survival, PFS: progression-free survival, RR: response rate, RD: response duration Nivolumab Second Line OS, Total Population Treatment Arm Median Rate at (95% CI), mo 1y HRa (95% CI) P Pembro 2 mg/kg 10.4 (9.4-11.9) 43.2% 0.71 (0.58-0.88) 0.00076 Pembro 10 mg/kg 12.7 (10.0-17.3) 52.3% 0.61 (0.49-0.75) <0.00001 Docetaxel 8.5 (7.5-9.8) 34.6% — — Analysis cut-off date: September 30, 2015. aComparison of pembrolizumab vs docetaxel. Moving on to Surrogates for OS… A measurement used in trials as an early and adequate substitute for OS, like ORR or PFS Advantages of surrogate markers: – Can be measured earlier – Convenient or less invasive An endpoint that is a surrogate for OS would be helpful in addressing the limitations of OS but must first be validated by satisfying statistical criteria A growing belief in the oncology community that delaying progression in metastatic disease is a worthy goal, even if OS is not improved – Can be measured more frequently – Can accelerate the approval process – May reduce the size of clinical trials – May shorten the duration of clinical trials – May reduce the cost of clinical trials PFS as an Endpoint Has Potential Advantages • Progression events occur early and more frequently than death events • Less influenced by competing causes of death • PFS is not influenced by post-progression therapy • Faster time to drug approval • Faster receipt by patients of novel therapies • Less cost to manufacturer or sponsor In Advanced NSCLC PFS as primary endpoint (prolonged PFS): - Tyrosine kinase inhibitor trials in selected patients Saad, Katz. Ann Oncol. 2009; Burzykowski et al. JCO. 2008; Shi et al. Int J Clin Oncol. 2009. Use of PFS in the Contemporary Era 200 11 150 35 2 100 50 0 47 107 167 137 0 1975-1984 1985-1994 1995-2004 2005-2009 No. PUBLISHED RCT Booth C. J Clin Oncol. 2012. PFS AS PRIMARY ENDPOINT Can PFS be Considered a Strong and Robust Surrogate Endpoint? • Is a treatment that improves PFS really an advance for patients even if OS is not improved? • How does PFS relate to patient benefit? • Or is it only lowering the bar to declare efficacy and accelerate drug approval? Buyse M. Stat Methods Med Res. 2008. Booth C. J Clin Oncol. 2012. Disadvantages of Using PFS ASSESSMENT BIAS The investigator may declare a patient in the control arm a progressor to get a patient on an active experimental therapy ASAP EVOLUTION-TIME BIAS A suspected progression may be formally evaluated at a later time when patients are in one arm rather than the other arm THE EXACT TIME OF PROGRESSION IS UNKNOWN It requires frequent radiologic assessment, which introduces imprecision ATTRITION BIAS More patients may withdraw from one arm than from the other arm Challenges With PFS in Trials for Advanced NSCLC • Placebo-controlled, double-blind studies are required but sometimes impossible (eg, in cases of rash) • Other challenges – Progression without radiologic documentation – Clinical deterioration without radiologic progression – Missing data • Sensitivity analyses are required to assess whether the results are robust (Bhattacharya S et al. J Clin Oncol. 2009;27:5958) • Problems are more pronounced when PFS is short • Relevant for patient ? – Only if associated with improved QoL (symptom relief) and absence of relevant toxicity – Magnitude of improvement in QoL becomes an issue – Overall PFS is a soft endpoint Phase III Trials Comparing TKI vs Conventional CT in EGFR Mutation–positive NSCLC Study Control arm Ethnicity Rx evaluation Independent review PFS LUX-Lung 3 (n=345) Afatinib vs Cis/Pem Asian (71%) Caucasian 6w Yes 13.6 vs 6.9 11.1 vs 6.9 LUX-Lung 6 (n=364) Afatinib vs Cis/Gem Asian 6w Yes 11 vs 5.6 EURTAC (n=174) Erlotinib vs CT Caucasian 6w Yes 10.4 vs 5.4 OPTIMAL (N=165) Erlotinib vs Carb/Gem Asian 6w No 13.1 vs 4.6 WJTOG (n=172) Gefitinib vs Cis/Doc Asian 8w No 9.6 vs 6.3 NEJ002 (n=230) Gefitinib vs Carb/Pacl Asian 8w Yes 10.8 vs 5.4 IPASS (n=261) Gefitinib vs Carb/Pacl Asian 6w No 8.4 vs 6.7 SIGNAL (n=42) Gefitinib vs Cis/Gem Asian 9w Yes 9.5 vs 6.3 Afatinib Erlotinib Gefitinib Lines of Targeted Therapy and Overall Survival Results From the IPASS Trial: Subgroup of EGFR Mutation-positive Pts (n=261) Carboplatin/ paclitaxel (doublet chemo) arm Gefitinib arm 2 PFS: 9.5 months (median, 2010) (median, 2008) Chemotherapy Months EGFR TKI PFS: 6.3 months 1 (median, 2008) Months PFS: HR 0.48, 95% CI 0.36-0.64, p<0.001 OS: HR 1.00, 95% CI 0.76-1.33 1. Mok et al. 2008. 2. Yang et al. 2010. OS: 21.6 months 1 OS: 21.9 months (median, 2010) 2 First Line Use of Afatinib vs Chemotherapy and Survival in EGFR Del19 Subgroup LUX-Lung 3 LUX-Lung 6 Afatinib Pem/Cis n=112 n=57 Median, months HR (95%CI), p-value Estimated OS probability 0.8 33.3 1.0 21.1 0.54 (0.36–0.79), p=0.0015 0.6 0.4 HR (95%CI), p-value 18.4 0.64 (0.44–0.94), p=0.0229 0.4 0.2 0 0 3 6 31.4 0.6 0.2 0 Median, months 0.8 Estimated OS probability 1.0 Afatinib Gem/Cis n=124 n=62 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51 0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 Time (months) Time (months) No of patients No of patients Afatinib 112 108 105 102 96 93 83 80 72 62 58 51 34 30 21 6 1 0 Afatinib 124 122 118 115 106 99 90 80 73 69 59 39 16 8 1 0 Pem/Cis 57 55 50 46 43 37 33 27 25 22 20 16 10 1 0 0 Gem/Cis 62 30 28 26 21 18 11 4 3 0 0 Presented by: James Chih-Hsin Yang 6 1 58 53 49 44 35 Yang JC et al. Lancet Oncology. 2015 What Is the True Definition of Meaningful Clinical Benefit? • 68 year old lady, T3N1M0, diagnosed with T3N1M0IIIA adenocarcinoma of lung in 2004, after surgery, she received 4 cycles of paclitaxel and carboplatin • Recurrence in 2007/Oct with multiple lung mets, EGFR L858R+ • Afatinib started 2007/Oct/15 (Lux-Lung-2), progression 2015/July/10, cycle 101 • Afatinib continued beyond progression until 2015/Dec/14 2007/Oct 2015/July/10 2015/Dec/14 PATIENT-REPORTED OUTCOMES (PRO) Are PRO Measures Underappreciated and Underused in Oncology? • PRO address more than just symptoms • Direct measures of patient benefit, they can be considered independent endpoints • This approach is especially useful in trials of drugs for patients with incurable cancers, in which one of the main goals is to improve palliation of symptoms • Only 1/3 of phase III breast cancer trials registered with US NIH have collected or are presently collecting PRO For more on PROs, stay tuned for Dr. Silvia Novello’s talk Wilson et al. Lancet Oncol. 2015. Some Recent Observations and Future Trends • PFS is proving more challenging to employ as a regulatory endpoint – However, it will continue to have a future potential role in oncology drug registration if rigorous acceptance criteria and standards are met • There will be increasing regulatory pressure to link or associate PFS benefits with other clinical trial outcomes that show direct clinical benefit (e.g. QoL benefits, disease-related symptom benefits, OS positive trends) – PFS may have its best future applications in symptomatic disease settings and/or where delay in disease progression correlates with delay in symptom onset – Benefit of delay of progression may also be measured by assessing QoL benefits pre- vs post-progression, independent of study arm New Challenges in Endpoint Selection for New Therapies • INMUNOTHERAPY – Pseudo-progression effect: go vs no-go decision – Survival benefit in the absence of significant responses, or very significant PFS • PERSONALISED THERAPIES – Intra-patient heterogeneity – How to deal with • Brain mets • Single-site progression • Benefit beyond progression • WILL WE BE ABLE TO DEFINE THE BEST SEQUENCING? Accelerated Approval for Breakthrough Medications • • • • • Orphan drug designation Breakthrough treatment designation (based on scientific and clinical evidence) Expedited review Accelerated approval (based on response and response duration) Full approval (based on phase III studies comparing PFS, OS) Development of Reliable Endpoints to Allow an Early Recognition of Clinical Benefit Wilson et al. Lancet Oncol. 2015. 3rd G Osimertinib: EGFR TKI failure T790M+ NSCLC Patients Specific Inhibitor to T790M and Activating Mutations AURA Ph I 80 40 20 0 –20 –40 –60 –80 –100 100 Best percentage change from baseline in target lesion size (%) Best percentage change from baseline in target lesion size (%) 100 AURA pooled Ph II 80 60 40 20 ********* 0 –20 Complete response Partial response Stable disease Progressive disease Not evaluable –40 –60 –80 –100 Complete response Partial response Stable disease Progressive disease Not evaluable AURA Ph I (80 mg) N=61 Confirmed ORR 71% (95% CI 57, 82) Disease control rate† 93% (95% CI 84, 98) Best objective response Complete response Partial response Stable disease ≥6 weeks Progressive disease 1 42 14 2 • AURA Ph I data cut-off 4 January 2016; population: evaluable for response set; assessment: investigator assessed; • AURA pooled Ph II data cut-off 1 November 2015; population: evaluable for response set; assessment: BICR • *Represents imputed values: if it is known that the patient has died, has AURA pooled Ph II (80 mg) new lesions or progression of nonN=397 target lesions, has withdrawn due to • disease progression, and has no 66% evaluable target lesion (before or at (95% CI 61, 71) progression) assessments, best change will be imputed as 20%. 91% † (95% CI 88, 94) • Complete response, partial response, stable disease ≥6 weeks. • 6 ORR, objective response rate; CI, 256 confidence interval. 99 25 EUROPEAN LUNG CANCER CONFERENCE 2016 Yang JC et al. When to Use 3rd-Generation EGFR TKI? (Targeted Therapy) Gefitinib Erlotinib Afatinib Pemetrexed 2nd-line CT platinum Docetaxel 3rd-generation EGFR TKI AURA-ext; AURA2 AURA-ext; AURA2 AURA3; ELUXA2 Other EGFR TKI+ cMETi or anti-PD1 1st-line 3rd-generation EGFR TKI FLAURA, SOLAR Resistance Mechanism Overall Survival? Phase IIb/III Trial of Afatinib (BIBW 2992) + Best Supportive Care (BSC) vs Placebo + BSC in Patients Failing 1–2 lines of CT and Erlotinib/Gefitinib (LUX-Lung 1) Endpoints Patients • Chemo-naïve • Life expectancy ≥12 weeks • PS BIBW2992 BSC IIIB/IV disease 2:1 randomisation • Failed 1 or 2 lines of chemotherapy • Failed Placebo • Used BSC to gefitinib or erlotinib gefitinib or erlotinib for more than 3 months Miller VA, Yang JC. Lancet Oncol. 2012;13(5):528-38. • Overall Survival Time Secondary 0-2 • Stage Primary Progression-free Survival Time Objective Response Rate (according to RECIST) Duration of Clinical Benefit (CR, PR, SD) Time to Objective Response Duration of Objective Response Safety of BIBW 2992 PK parameters Health-related Quality of Life LUX-Lung 1: Afatinib vs Placebo in 3rd/4th-line Efficacy Shown in PFS, but Salvage Agents Were Equally Effective Overall Survival Miller VA, Yang JC. Lancet Oncol. 2012;13(5):528-38. PFS LUX-Lung 5, 4th/5th-line Study Afatinib + Paclitaxel vs Chemotherapy PFS Schuler M et al. Annals of Oncology, 2016;27:417-423. OS MOLECULAR ONCOLOGY…NEW TRIAL ENDPOINTS Buyse M. et al. Nat Rev Clin Oncol. 2010. TREATMENTS ENDPOINTS Signal transduction inhibitors Effect on molecular target Gene expression modulators Circulating tumour cells Angiogenesis inhibitor Circulating tumour DNA Immunotherapies Functional imaging Key Guidelines for Clinical Trial Endpoint Selection The decision should always be related to: • The patient subpopulation of interest • The stage of disease (depends on the type of cancer) • The characteristics of the treatment (toxicity, efficacy) • The aims of the trial (superiority/noninferiority/safety) • The other treatments already available to that group of patients • Ethics • Practical feasibility (costs, logistics…)