Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
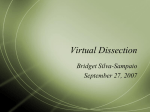
Central neck lymph node dissection is an important component in the treatment of papillary thyroid cancer. Rebecca Kinkead. Nadav and Sara (detail), 2009. Oil and alkyd on canvas, 45⬙ × 37⬙. Central Neck Dissection for Papillary Thyroid Cancer David T. Hughes, MD, and Gerard M. Doherty, MD Background: Central compartment lymph node dissection is a common adjunct to thyroidectomy in the treatment of papillary thyroid cancer. The indications, surgical technique, potential benefits, and operative risks of this procedure should be clearly defined in order to provide optimal care to these patients. Methods: A systematic review of the literature and an analysis of evidence-based recommendations were performed regarding central neck node dissection for patients with papillary thyroid carcinoma. Results: Cervical nodal metastasis in papillary thyroid cancer is a common occurrence. The presence of metastasis is associated with increased recurrence rates and may decrease survival. Detection of central and lateral neck nodal metastasis preoperatively with clinical examination and cervical ultrasound is important in determining the appropriate initial surgical management. Level VI neck dissection and central neck dissection are terms often used interchangeably to describe surgical excision of all lymph nodes from the hyoid bone to the sternal notch between the carotid arteries, but the addition of the superior mediastinal lymph nodes in compartment VII should be included in the central neck dissection. Due to improved recurrence rates and survival, therapeutic central neck dissection is recommended for all patients with nodal involvement detected pre- or intraoperatively. Prophylactic central neck dissection in patients without detectable nodal disease remains a controversial topic due to a lack of definitive evidence of improved recurrence rates or survival and the possibility of higher complication rates compared to total thyroidectomy alone. Reoperative central nodal dissection can be a challenging procedure with increased complication rates but with good outcomes in experienced centers. Conclusions: Central neck lymph node dissection plays an important role in the appropriate treatment of papillary thyroid cancer at initial presentation and in cases of recurrent disease. Surgeons caring for this group of patients should have familiarity and skill with this procedure. Introduction From the Department of Surgery at the University of Michigan, Ann Arbor, Michigan. Dr Hughes is now with Montefiore Medical Center/Albert Einstein College of Medicine, Bronx, NY. Submitted February 24, 2010; accepted April 16, 2010. Address correspondence to David T. Hughes, MD, Montefiore Medical Center/Albert Einstein College of Medicine, 1400 Bainbridge Avenue, Bronx, NY 10467. E-mail: [email protected] No significant relationship exists between the authors and the companies/organizations whose products or services may be referenced in this article. April 2011, Vol 18, No. 2 Papillary thyroid cancer is the most common form of differentiated thyroid cancer, comprising approximately 90% of the 44,670 estimated new cases of thyroid cancer in the United States in 2010.1 The established primary treatment of papillary thyroid cancer per American Thyroid Association (ATA) guidelines is total thyroidectomy for all tumors larger than 1 cm, while thyroid lobectomy is sufficient for tumors smaller than 1 cm.2 The ATA consensus statement also recommends therapeutic central neck dissection in patients with clinically involved nodes and prophylactic central neck dissection in advanced primary tumors (T3 or T4) without evidence of Cancer Control 83 nodal involvement.2 Radioactive iodine ablation plays an important role in adjuvant treatment following thyroidectomy for some subgroups of patients based on risk of recurrence.2 This treatment algorithm achieves extremely low death rates; however, the rates for cervical lymph node metastasis and recurrence remain significant. Despite the ATA recommendations, there is controversy regarding the ideal surgical management of the central neck lymph nodes in patients with papillary thyroid cancer. Nodal Metastasis in Papillary Thyroid Cancer Incidence and Relevance Papillary thyroid cancer and the follicular variant of papillary thyroid cancer have a propensity for cervical lymphatic spread that occurs in 20% to 50% of patients on standard review of surgical pathologic specimens and in 90% of those examined for micrometastases.3,4 The spread of tumors cells occurs in a predictable pattern that initiates in the perithyroidal lymph nodes of the central neck and progresses to the lymph nodes of the lateral cervical compartments and the superior mediastinum.5,6 “Skip” metastases to the lateral compartment Fig 1. — Lymph node compartments of the neck. Level VI and VII are included in central neck dissection, while lateral neck dissection typically includes levels II–V for treatment of papillary thyroid cancer. From American Thyroid Association Surgery Working Group, American Association of Endocrine Surgeons, American Academy of Otolaryngology-Head and Neck Surgery, et al. Consensus statement on the terminology and classification of central neck dissection for thyroid cancer. Thyroid. 2009;19(11):11531158. Courtesy of Mary Ann Liebert, Inc. 84 Cancer Control without central neck nodal involvement are rare but do occur.5,6 Patients with nodal metastasis have higher rates of persistent and recurrent disease during postoperative surveillance.6 The impact of nodal metastasis on overall survival remains debatable; several studies have demonstrated no difference in mortality, while two large population-based studies have shown increased mortality in patients with regional lymph node metastasis.7-11 Detection of Nodal Metastasis The initial approach to a patient with a thyroid nodule should include a detailed examination of the thyroid and the cervical lymph node compartments. The classification system of cervical lymph node compartments is well defined and is important not only in identifying the location of pathologic lymph nodes, but also in planning surgical treatment as outlined and illustrated in the recent ATA guidelines for management of thyroid cancer (Fig 1).2,12,13 Patients with papillary thyroid cancer occasionally present on initial assessment with palpable cervical lymphadenopathy, which is most often located in the central neck or levels III and IV of the lateral neck, usually in conjunction with an ipsilateral thyroid nodule. Cervical ultrasound, often performed as an officebased examination, is the primary imaging modality for the initial assessment as well as the postoperative surveillance of patients with papillary thyroid cancer. Highresolution ultrasonography can detect cervical nodal metastasis in 14% to 20% of papillary thyroid cancer patients and can detect pathologic nodes as small as 2 to 3 mm without the risks associated with radiation exposure.14,15 Ultrasound is also easily repeatable and has been shown to change the surgical procedure performed in 39% of thyroid cancer patients.14,15 A dedicated cervical ultrasound to include nodal levels II–VI should be performed, ideally by a dedicated clinician such as the thyroid endocrinologist, the operating surgeon, or a radiologist with particular interest, to detect nonpalpable lymph node metastases in patients undergoing surgical evaluation for any thyroid nodule (Fig 2). The sensitivity Fig 2. — Ultrasonic appearance of level III lymph node with papillary thyroid cancer metastasis using 12.5 MHz linear transducer. Note the irregular border of the lymph node and the lack of the normal hyperechoic hilar line. April 2011, Vol 18, No. 2 of cervical ultrasound to detect pathologic lymph nodes in papillary thyroid cancer patients is higher in the lateral neck (94%) than in the central neck (53% to 55%), and this disparity may be considered as additional support for prophylactic central neck dissection.16 Pathologic lymph node metastasis detected on ultrasound can be confirmed with ultrasound-guided fine needle aspiration. In patients with suspected mediastinal disease or with bulky cervical lymphadenopathy, cross-sectional imaging with CT should be considered as it can aid in the planning of nodal dissection and often identifies pathologic level VI and VII lymph nodes within the superior mediastinum that are not detected on cervical ultrasound or physical examination. Operative Considerations for Central Neck Lymph Node Dissection Technique Cervical nodal dissection for papillary thyroid cancer should include a systematic or en bloc nodal basin dissection rather than a selective or “berry picking” dissection due to higher rates of persistent and recurrent disease with the later approach.17 The ATA consensus statement12 regarding the terminology and classification of the central neck defines the central compartment nodal dissection as all perithyroidal and paratracheal soft tissue and lymph nodes with borders extending superiorly to the hyoid bone, inferiorly to the innominate artery, and laterally to the common carotid arteries and is well described and illustrated by Grodski et al18 (Fig 3). The inclusion of the level VII nodes in the superior mediastinum with the central neck dissection should be noted as this is often a site of persistent disease following central neck dissection. Moo et al19 compared ipsilateral vs bilateral central neck dissection for papillary thyroid cancer and concluded that an ipsilateral dissection was sufficient in tumors less than 1 cm, while tumors larger than 1 cm required bilateral central neck dissection based on the high incidence of contralateral central neck disease in a retrospective analysis of the pattern of nodal metastases in surgical specimens. Some additional studies demonstrated that ipsilateral central neck dissection was adequate for tumors larger than 1 cm.20 If lateral cervical metastases are present in levels II–V, a bilateral central nodal dissection should be included with the modified radical neck dissection to remove the presumed central neck nodal disease based on described patterns of nodal spread.21 Complications Complications of central neck dissection include injury to the recurrent laryngeal nerve or the external branch of the superior laryngeal nerve, which occurs in 1% to 2% of patients based on several studies.20,22-25 Small retrospective studies have shown that the addition of central compartment lymphadenectomy to total thyroidectomy for thyroid cancer has not increased nerve injury rates in experienced hands.20,22,23,26 In cases of reoperative central lymph node dissection after either previous thyroidectomy or central node dissection, reports have noted increased nerve injury rates ranging from 1% to 12%.24,25,27-29 Temporary hypoparathyroidism following central neck dissection occurs in 14% to 40% of cases depending on the definition of hypoparathyroidism used in the study.20,22,23,30-33 The higher incidence of temporary hypoparathyroidism is likely due to the increased incidence of parathyroid reimplantation and inadvertent inclusion of parathyroid glands in the nodal dissection. Reports are mixed regarding the risk of permanent hypoparathyroidism. A meta-analysis of retrospective studies reported a 1.2% incidence as defined by the requirement for calcium supplements greater than 6 to 12 months postoperatively; however, none showed a statistically significant difference in total thyroidectomy with or without central neck dissection.34 Situational Considerations Fig 3. — Right-level VI lymph node dissection including all perithyroidal and paratracheal soft tissue and lymph nodes. Judicious use of parathyroid reimplantation should be utilized with regard to the lower parathyroid glands. From Grodski S, Cornford L, Sywak M, et al. Routine level VI lymph node dissection for papillary thyroid cancer: surgical technique. ANZ J Surg. 2007;77(4):203-208. Reprinted with permission of John Wiley and Sons, Inc. April 2011, Vol 18, No. 2 Therapeutic Central Neck Dissection Pathologic lymph node involvement noted on preoperative clinical or imaging assessment is a well-established indication for therapeutic lymph node dissection.2 A careful search for the presence of pathologic central compartment lymph nodes with both physical examination and cervical ultrasound is critical during preoperative assessment. The presence of pathologic level VI lymph nodes should prompt detailed physical and ultrasonic examination of the lateral cervical nodal chains for additional evidence of metastasis. Suspicion of lymph node Cancer Control 85 involvement can be confirmed with fine needle aspiration biopsy. The surgical technique for therapeutic nodal dissection should include both the ipsilateral and the contralateral central compartments. The lymph node dissection specimen should be excised en bloc during thyroidectomy. Any incidental note of suspicious nodes in the lateral neck should prompt biopsy and frozen section analysis for confirmation of cancer involvement. If cancer is present in any lateral neck nodes, the dissection should be extended to an ipsilateral modified radical neck dissection to include levels II–V.35-37 Liberal application of parathyroid reimplantation during central neck dissection should be employed to prevent postoperative hypoparathyroidism.20 There are several goals in the use of nodal dissection for clinically evident locoregional lymph node metastasis in papillary thyroid cancer. The primary intent is locoregional control of disease, given the correlation of nodal metastasis with significant increases in persistent and recurrent disease.6,8,38,39 Several studies have demonstrated decreased recurrence rates and improved survival when the burden of cervical disease is removed via therapeutic neck dissection.15,33,40 In patients with known distant metastatic disease, the debulking of cervical disease for palliative purposes is beneficial in preventing local complications. Prophylactic Central Neck Dissection Prophylactic or routine central neck dissection for patients with papillary thyroid carcinoma is defined as complete excision of the level VI and VII lymph nodes in patients with no evidence of nodal involvement after preoperative clinical and imaging evaluation. The role of prophylactic central neck dissection remains a contentious issue regarding its benefits and risks, and several reports have reviewed this subject.41-43 Several singleinstitution retrospective cohort studies on total thyroidectomy alone vs with prophylactic neck dissection, as well as a meta-analysis of these studies, have reported mixed results.20,22,23,30,31,34 Proponents of prophylactic central neck dissection at the time of initial thyroidectomy cite the high incidence of cervical lymph node metastasis and the associated increase in recurrence rates with the possibility of decreased survival. The low sensitivity of preoperative ultrasound evaluation and intraoperative assessment to accurately detect lymph node involvement is also used as rationale for routine central neck dissection.15,38,44 The addition of central neck dissection to initial total thyroidectomy can provide valuable staging information and has been shown to upstage approximately a third of patients older than 45 years of age to stage III disease in two retrospective reviews.45,46 This upstaging has important implications for further treatment as those with nodal metastasis are likely to receive higher doses of I131 ablation treatment, while those with small, 86 Cancer Control noninvasive tumors without nodal disease can forgo I131 ablation. The evidence to support prophylactic dissection due to decreased recurrence rates and improved survival is sparse and is primarily composed of a prospective population-based study from Sweden.47 This study demonstrated that the rate of death due to thyroid cancer, which ranged from 8.4% to 11.1%, was reduced to 1.6% in patients who underwent central neck dissection compared to contemporary controls. However, several retrospective cohort studies have shown no difference or only a slight improvement in recurrence or survival rates.36,48-50 While an additional benefit of reduced postoperative thyroglobulin levels after central neck dissection was demonstrated by Sywak et al,20 a recent study at our institution showed no difference in thyroglobulin levels between total thyroidectomy or total thyroidectomy with central neck dissection.46 In patients with known distant metastasis without evidence of cervical nodal involvement, a prophylactic neck dissection to include both the central neck and the ipsilateral lateral neck has been recommended by some due to the high rates of nodal involvement in this group of patients on histological analysis.51 Overall, the addition of prophylactic central neck dissection appears to provide important staging information that can affect radioactive iodine ablative treatment, but the evidence regarding recurrence and survival benefits remains limited and conflicted. The arguments against prophylactic central lymph node dissection at the time of initial thyroidectomy for papillary cancer focus on the unproven benefit and the possibility of increased complications. The relevance of subclinical cervical lymph node metastasis on rates of recurrence and survival has been questioned by some retrospective studies.50 Additionally, there is a lack of proven benefit in outcomes after prophylactic central node dissection. The possibility of increased complication rates with central neck dissection has been addressed, although again by only small retrospective cohort studies.20-23,26,31,52 Higher rates of temporary hypoparathyroidism with central neck dissection seem consistent between these studies, while the rates of permanent hypoparathyroidism and nerve injury rates are statistically similar compared with total thyroidectomy alone.34,42 The debate on the role of routine central neck dissection in the treatment of papillary thyroid carcinoma is likely to continue until a large randomized trial with long-term follow-up can be completed. Reoperative Central Neck Dissection Reoperative central neck dissection is defined as removal of all remaining soft tissue in the level VI and VII compartments in a patient who has undergone previous thyroidectomy or central lymph node dissection. This is often indicated for patients with papillary thyroid cancer who are noted to have central neck lymph node involvement on surveillance examination or imaging studies after comApril 2011, Vol 18, No. 2 References Fig 4. — CT imaging demonstrating a superior mediastinal lymph node involved with recurrent papillary thyroid carcinoma (arrow). This was removed via a cervical incision during reoperative central neck dissection and was positive for metastatic papillary thyroid cancer. pletion of radioactive iodine ablation therapy. The goal of reoperative neck dissection is the removal of all persistent or recurrent cervical disease. It is important to closely evaluate patients for the presence of additional pathologic lymphadenopathy in the lateral neck and superior mediastinum. Combining imaging modalities with cervical ultrasound and cross-sectional imaging with CT or PET/ CT can help to guide operative planning and to determine the necessary extent of nodal dissection. Ultrasound and physical examination will often miss pathologic lymphadenopathy in the superior mediastinum, which can be detected with cross-sectional imaging and can usually be removed via a cervical incision with caudal extension of the central compartment lymphadenectomy (Fig 4). Preoperative laryngoscopy should be performed before all reoperative procedures to determine the presence of recurrent laryngeal nerve injury, which can affect the approach to reoperative nodal dissection. Several studies have demonstrated increased risk of complications with reoperative central neck dissection, with nerve injury rates of 1% to 12% and permanent hypoparathyroidism rates of 0 to 3.5%.24,25,27-29 Given the challenging nature of reoperative neck dissection, consideration of recurrent laryngeal nerve monitoring and special care to preserve the parathyroid vascular pedicles originating from the inferior thyroidal arteries are important. Conclusions Central neck dissection is the most common neck dissection completed for patients with papillary thyroid cancer and can be performed safely and effectively with low complication rates by experienced surgeons. Therapeutic central neck dissection is recommended for all patients with clinically evident disease. Prophylactic central neck dissection should be considered in order to provide more accurate staging in high-risk patients. However, conclusive data are lacking regarding its influence on recurrence, survival, and complication rates. April 2011, Vol 18, No. 2 1. Jemal A, Siegel R, Xu J, et al. Cancer statistics, 2010. CA Cancer J Clin. 2010;60(5):277-300. 2. American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer, Cooper DS, Doherty GM, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19(11):1167-1214. 3. Cooper DS, Doherty GM, Haugen BR, et al. Management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2006;16(2):109-142. 4. Arturi F, Russo D, Giuffrida D, et al. Early diagnosis by genetic analysis of differentiated thyroid cancer metastases in small lymph nodes. J Clin Endocrinol Metab. 1997;82(5):1638-1641. 5. Gimm O, Rath FW, Dralle H. Pattern of lymph node metastases in papillary thyroid carcinoma. Br J Surg. 1998;85(2):252-254. 6. Machens A, Hinze R, Thomusch O, et al. Pattern of nodal metastasis for primary and reoperative thyroid cancer. World J Surg. 2002;26(1):22-28. 7. Rossi RL, Cady B, Silverman ML, et al. Current results of conservative surgery for differentiated thyroid carcinoma. World J Surg. 1986;10(4):612-622. 8. Mazzaferri EL, Jhiang SM. Long-term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer. Am J Med. 1994;97(5):418-428. 9. Hughes CJ, Shaha AR, Shah JP, et al. Impact of lymph node metastasis in differentiated carcinoma of the thyroid: a matched-pair analysis. Head Neck. 1996;18(2):127-132. 10. Lundgren CI, Hall P, Dickman PW, et al. Clinically significant prognostic factors for differentiated thyroid carcinoma: a population-based, nested case-control study. Cancer. 2006;106(3):524-531. 11. Podnos YD, Smith D, Wagman LD, et al. The implication of lymph node metastasis on survival in patients with well-differentiated thyroid cancer. Am Surg. 2005;71(9):731-734. 12. American Thyroid Association Surgery Working Group, American Association of Endocrine Surgeons, American Academy of OtolaryngologyHead and Neck Surgery, et al. Consensus statement on the terminology and classification of central neck dissection for thyroid cancer. Thyroid. 2009;19(11):1153-1158. 13. Robbins KT, Clayman G, Levine PA, et al. Neck dissection classification update: revisions proposed by the American Head and Neck Society and the American Academy of Otolaryngology-Head and Neck Surgery. Arch Otolaryngol Head Neck Surg. 2002;128(7):751-758. 14. Stulak JM, Grant CS, Farley DR, et al. Value of preoperative ultrasonography in the surgical management of initial and reoperative papillary thyroid cancer. Arch Surg. 2006;141(5):489-494; discussion 494-496. 15. Kouvaraki MA, Shapiro SE, Fornage BD, et al. Role of preoperative ultrasonography in the surgical management of patients with thyroid cancer. Surgery. 2003;134(6):946-954; discussion 954-955. 16. Ahn JE, Lee JH, Yi JS, et al. Diagnostic accuracy of CT and ultrasonography for evaluating metastatic cervical lymph nodes in patients with thyroid cancer. World J Surg. 2008;32(7):1552-1558. 17. Hay ID, Bergstralh EJ, Grant CS, et al. Impact of primary surgery on outcome in 300 patients with pathologic tumor-node-metastasis stage III papillary thyroid carcinoma treated at one institution from 1940 through 1989. Surgery. 1999;126(6):1173-1181; discussion 1181-1182. 18. Grodski S, Cornford L, Sywak M, et al. Routine level VI lymph node dissection for papillary thyroid cancer: surgical technique. ANZ J Surg. 2007;77(4):203-208. 19. Moo TA, Umunna B, Kato M, et al. Ipsilateral versus bilateral central neck lymph node dissection in papillary thyroid carcinoma. Ann Surg. 2009; 250(3):403-408. 20. Sywak M, Cornford L, Roach P, et al. Routine ipsilateral level VI lymphadenectomy reduces postoperative thyroglobulin levels in papillary thyroid cancer. Surgery. 2006;140(6):1000-1005; discussion 1005-1007. 21. Roh JL, Park JY, Rha KS, et al. Is central neck dissection necessary for the treatment of lateral cervical nodal recurrence of papillary thyroid carcinoma? Head Neck. 2007;29(10):901-906. 22. Henry JF, Gramatica L, Denizot A, et al. Morbidity of prophylactic lymph node dissection in the central neck area in patients with papillary thyroid carcinoma. Langenbecks Arch Surg. 1998;383(2):167-169. 23. Palestini N, Borasi A, Cestino L, et al. Is central neck dissection a safe procedure in the treatment of papillary thyroid cancer? Our experience. Langenbecks Arch Surg. 2008;393(5):693-698. 24. Kim MK, Mandel SH, Baloch Z, et al. Morbidity following central compartment reoperation for recurrent or persistent thyroid cancer. Arch Otolaryngol Head Neck Surg. 2004;130(10):1214-1216. 25. Moley JF, Lairmore TC, Doherty GM, et al. Preservation of the recurrent laryngeal nerves in thyroid and parathyroid reoperations. Surgery. 1999;126(4):673-677; discussion 677-679. 26. Roh JL, Park JY, Park CI. Prevention of postoperative hypocalcemia with routine oral calcium and vitamin D supplements in patients with differentiated papillary thyroid carcinoma undergoing total thyroidectomy plus central neck dissection. Cancer. 200;115(2):251-258. Cancer Control 87 27. Segal K, Friedental R, Lubin E, et al. Papillary carcinoma of the thyroid. Otolaryngol Head Neck Surg. 1995;113(4):356-363. 28. Simon D, Goretzki PE, Witte J, et al. Incidence of regional recurrence guiding radicality in differentiated thyroid carcinoma. World J Surg. 1996; 20(7): 860-866; discussion 866. 29. Uruno T, Miyauchi A, Shimizu K, et al. Prognosis after reoperation for local recurrence of papillary thyroid carcinoma. Surg Today. 2004;34(11): 891-895. 30. Roh JL, Park JY, Park CI. Total thyroidectomy plus neck dissection in differentiated papillary thyroid carcinoma patients: pattern of nodal metastasis, morbidity, recurrence, and postoperative levels of serum parathyroid hormone. Ann Surg. 2007;245(4):604-610. 31. Steinmüller T, Klupp J, Wenking S, et al. Complications associated with different surgical approaches to differentiated thyroid carcinoma. Langenbecks Arch Surg. 1999;384(1):50-53. 32. Pereira JA, Jimeno J, Miquel J, et al. Nodal yield, morbidity, and recurrence after central neck dissection for papillary thyroid carcinoma. Surgery. 2005;138(6):1095-1100; discussion 1100-1101. 33. Gemsenjäger E, Perren A, Seifert B, et al Lymph node surgery in papillary thyroid carcinoma. J Am Coll Surg. 2003;197(2):182-190. 34. Chisholm EJ, Kulinskaya E, Tolley NS. Systematic review and metaanalysis of the adverse effects of thyroidectomy combined with central neck dissection as compared with thyroidectomy alone. Laryngoscope. 2009;119(6):1135-1139. 35. Wada N, Duh QY, Sugino K, et al. Lymph node metastasis from 259 papillary thyroid microcarcinomas: frequency, pattern of occurrence and recurrence, and optimal strategy for neck dissection. Ann Surg. 2003; 237(3):399-407. 36. Scheumann GF, Gimm O, Wegener G, et al. Prognostic significance and surgical management of locoregional lymph node metastases in papillary thyroid cancer. World J Surg. 1994;18(4):559-567; discussion 567-568. 37. Farrag TY, Agrawal N, Sheth S, et al. Algorithm for safe and effective reoperative thyroid bed surgery for recurrent/persistent papillary thyroid carcinoma. Head Neck. 2007;29(12):1069-1074. 38. Ito Y, Tomoda C, Uruno T, et al. Clinical significance of metastasis to the central compartment from papillary microcarcinoma of the thyroid. World J Surg. 2006;30(1):91-99. 39. Low TH, Delbridge L, Sidhu S, et al. Lymph node status influences follow-up thyroglobulin levels in papillary thyroid cancer. Ann Surg Oncol. 2008;15(10):2827-2832. 40. Ito Y, Tomoda C, Uruno T, et al. Preoperative ultrasonographic examination for lymph node metastasis: usefulness when designing lymph node dissection for papillary microcarcinoma of the thyroid. World J Surg. 2004; 28(5):498-501. 41. White ML, Gauger PG, Doherty GM. Central lymph node dissection in differentiated thyroid cancer. World J Surg. 2007;31(5):895-904. 42. Mazzaferri EL, Doherty GM, Steward DL. The pros and cons of prophylactic central compartment lymph node dissection for papillary thyroid carcinoma. Thyroid. 2009;19(7):683-689. 43. Mazzaferri EL. What is the optimal initial treatment of low-risk papillary thyroid cancer (and why is it controversial)? Oncology (Williston Park). 2009;23(7):579-588. 44. Moley JF, DeBenedetti MK. Patterns of nodal metastases in palpable medullary thyroid carcinoma: recommendations for extent of node dissection. Ann Surg. 1999;229(6):880-887; discussion 887-888. 45. Bonnet S, Hartl D, Leboulleux S, et al. Prophylactic lymph node dissection for papillary thyroid cancer less than 2 cm: implications for radioiodine treatment. J Clin Endocrinol Metab. 2009;94(4):1162-1167. 46. Hughes DT, White ML, Miller BB, et al. Influence of prophylactic central lymph node dissection on postoperative thyroglobulin levels and radioiodine treatment in papillary thyroid cancer. Surgery. 2010;148(6):1100-1106; discussion 1006-1007. 47. Tisell LE, Nilsson B, Mölne J, et al. Improved survival of patients with papillary thyroid cancer after surgical microdissection. World J Surg. 1996;20(7):854-859. 48. Noguchi S, Murakami N, Yamashita H, et al. Papillary thyroid carcinoma: modified radical neck dissection improves prognosis. Arch Surg. 1998;133(3):276-280. 49. Shah MD, Hall FT, Eski SJ, et al. Clinical course of thyroid carcinoma after neck dissection. Laryngoscope. 2003;113(12):2102-2107. 50. Steinmüller T, Klupp J, Rayes N, et al. Prognostic factors in patients with differentiated thyroid carcinoma. Eur J Surg. 2000;166(1):29-33. 51. Sugitani I, Fujimoto Y, Yamada K, et al. Prospective outcomes of selective lymph node dissection for papillary thyroid carcinoma based on preoperative ultrasonography. World J Surg. 2008;32(11):2494-2502. 52. Bardet S, Malville E, Rame JP, et al. Macroscopic lymph-node involvement and neck dissection predict lymph-node recurrence in papillary thyroid carcinoma. Eur J Endocrinol. 2008;158(4):551-560. 88 Cancer Control April 2011, Vol 18, No. 2