Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Transtheoretical model wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Public health genomics wikipedia , lookup
Epidemiology of metabolic syndrome wikipedia , lookup
Epidemiology wikipedia , lookup
Seven Countries Study wikipedia , lookup
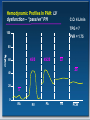
A Practical Approach to Pulmonary Hypertension Brittany Palmer, M.D. Outline • • • • • • PH definition and classification Pathogenesis Patient assessment Making the diagnosis Therapeutic options and efficacy Summary Pulmonary Arterial Hypertension: Definition • Mean PA pressure > 25 mmHg with PCW <15 mmHg – (NIH Registry on PPH, 1987) • PVR ≥ 3 Units PVR = TPG/CO TPG = PAM-PCW • Exercise mean PA pressure > 30-35 mmHg Clinical classification of pulmonary hypertension (Nice 2013) 1. Pulmonary arterial hypertension – Idiopathic PAH – Heritable PAH (BMPR2, ALK1) – Drug and Toxin induced – Associated with: • • • • • Connective tissue disease Congenital heart disease Portal hypertension HIV infection Schistosomiasis 2. PH with left heart disease Systolic or diastolic dysfunction Valvular Congenital/acquired left heart inflow/outflow tract obstruction and congenital cardiomyopathies 1’. PVOD/PCH Simonneau G, et al. J Am Coll Cardiol. 20013;62(25_S) Clinical classification of pulmonary hypertension (Nice 2013) 3. PH with lung diseases/hypoxemia • • • • • • COPD Interstitial lung disease Sleep-disordered breathing Developmental abnormalities Mixed restrictive/obstructive Alveolar hypoventilation 5. Miscellaneous Pulmonary hypertension with unclear multifactorial mechanisms Hematologic disorders: myeloproliferative disorders, splenectomy, chronic hemolytic anemia Systemic disorders: sarcoidosis, pulmonary histiocytosis, lymphangioleiomyomatosis Metabolic disorders: glycogen storage disease, Gaucher disease, thyroid disorders Others: tumoral obstruction, fibrosing mediastinitis, chronic renal failure, segmental PH 4. PH due to chronic thrombotic and/or embolic disease • CTEPH Simonneau G, et al. J Am Coll Cardiol. 2013;62(25_S) Pathogenesis of Pulmonary Arterial Hypertension NORMAL Gaine, JAMA 2000;284:3164 REVERSIBLE DISEASE IRREVERSIBLE DISEASE Percentage Surviving A Disease of Decline & Deterioration IPAH Survival 100 NIH Registry Sitbon Historical Control ACCP Estimate 80 60 40 20 0 0 0.5 1 1.5 2 2.5 3 3.5 Years of Follow-up Adapted from: Sitbon O et al. J Am Coll Cardiol. 2002;40:780-788. Adapted from: D’Alonzo GE,. Ann Int Med 1991;115:343-349 Adapted from: McLaughlin et al. CHEST; 126: 78S-91S 4 4.5 5 Assessment of PAH: Signs and Symptoms • Initial signs and symptoms - Dyspnea - Fatigue - Syncope - Edema - Dizziness - Angina • Non-specific nature of complaint can lead to: - Confusion with other conditions - Delayed diagnosis Assessment of PAH: Physical Exam Presence of PH Presence of RV Failure • Loud P2 • JVD with V wave • RV lift • RV S3 • Systolic murmur (TR) • Hepatomegaly • Diastolic murmur (PR) • Edema • RV S4 • Ascites Assessment of PAH: CXR Peripheral Hypovascularity (Pruning) RV Enlargement into Retrosternal Clear Space Prominent Hilar Pulmonary Arteries Assessment of PAH: EKG RAD RVH RAE RV Strain McGoon M et al for the American College of Chest Physicians. Chest. 2004;126:14S-34S. PAH: Making the Diagnosis Is There A Reason to Suspect PAH? Clinical History (Symptoms, Risk Factors), Exam, CXR, ECG No No Further Evaluation Yes Is PH Likely? ECHO Rationale TR Velocity to Measure RVSP,RVE, RAE, RV Dysfunction Yes Is PH Due to LH Disease? ECHO McGoon M et al for the American College of Chest Physicians. Chest. 2004;126:14S-34S. Echocardiogram: Parasternal Long Axis Image courtesy of Vallerie McLaughlin, MD Echocardiogram: Parasternal Short Axis Image courtesy of Vallerie McLaughlin, MD Echocardiogram: Apical Four Chamber Image courtesy of Vallerie McLaughlin, MD Echocardiogram: Tricuspid Regurgitation Modified Bernoulli’s Equation: 4 x (V)² + RAP = RVSP (PASP) V=tricuspid jet velocity (m/s); RAP= right atrial pressure; RVSP=right ventricular systolic pressure; PASP=pulmonary artery systolic pressure. Image courtesy of Vallerie McLaughlin, MD PAH: Making the Diagnosis Is There A Reason to Suspect PAH? Clinical History (Symptoms, Risk Factors), Exam, CXR, ECG No No Further Evaluation Yes Is PH Likely? ECHO Rationale TR Velocity to Measure RVSP,RVE, RAE, RV Dysfunction Yes Is PH Due to LH Disease? ECHO Yes Dx LV Systolic, Diastolic Dysfunction; Valvular Disease: Appropriate Treatment Yes Dx Abnormal Morphology; Shunt: Surgery, Medical Treatment of PAH or Further Evaluation for Other Contributing Causes Yes Dx Scleroderma, SLE, HIV Infection: Medical Treatment of PAH and Further Evaluation for Other Contributing Causes No Is PH Due to CHD? ECHO With Bubble Study No Is PH Due to CTD, HIV? Serologies No Is Chronic PH Suspected? VQ Scan McGoon M et al for the American College of Chest Physicians. Chest. 2004;126:14S-34S. Ventilation Perfusion Lung Scan Idiopathic Pulmonary Arterial Hypertension Perfusion Ventilation Chronic Pulmonary Embolism Perfusion Ventilation Contrast-Enhanced CT Is Chronic PE Confirmed and Operable? Bands Pouch Absent branches PAH: Making the Diagnosis Is PH Due to Lung Disease? PFTs, Arterial Saturation Yes Dx Parenchymal Lung Disease, Hypoxemia, or Sleep Disorder: Medical Treatment, Oxygen, Positive Pressure Breathing As Appropriate, and Further Evaluation for Other Contributing Causes No What Limitations Are Caused by the PH? Functional Class; 6-minute Walk Distance Test (6MWD) What are precise pulmonary hemodynamics? RHC Document Exercise Capacity Regardless of Cause of PH: Establish Baseline, Prognosis and Document Progression/response to Treatment With Serial Reassessments Document PA pressure, PCWP (LV or LA pressure if PCWP unobtainable or uncertain), transpulmonary gradient, CO, PVR, MVO2, response to vasodilators: Confirm PAH, or IPAH if no other cause identified McGoon M et al for the American College of Chest Physicians. Chest. 2004;126:14S-34S. PAH Definition on RHC • Increased mean pulmonary arterial pressure (mPAP) – >25 mm Hg at rest or >30 mm Hg during exercise • Pulmonary vascular resistance (PVR): >3 WU • Normal PCWP (<15 mm Hg) Definition Characteristics Clinical group Pre-capillary PH Mean PAP ≥25 mm Hg PWP ≤15 mm Hg CO normal or reduced Post-capillary PH Mean PAP ≥25 mm Hg PWP >15 mm Hg CO normal or reduced Passive = TPG ≤12 mm Hg Reactive = TPG >12 mm Hg Adapted from: Galie N, et al. Eur Heart J. 2009;30(20):2493-2537. Pulmonary arterial hypertension PH due to lung disease CTEPH PH with unclear or multifactorial mechanisms PH due to left heart disease Progression of PAH Pre-symptomatic/ Compensated CO Symptomatic/ Decompensating Declining/ Decompensated Symptom Threshold PAP PVR Right Heart Dysfunction Time Therapeutic Options for PAH Traditional Rxs • • • • • Supplemental O2 Diuretics Oral vasodilators – (CCB) Anticoagulants – warfarin Inotropic agents – Digitalis • • • FDA Approved for PAH Investigational Rxs Prostanoids – Epoprostenol (iv) – Treprostinil (iv, sq, inh) – Iloprost (inhaled) ERAs – Bosentan – Ambrisentan – Macitentan PDE-5 Inhibitors – Sildenafil – Tadalafil • • • Prostanoids – Oral Treprostinil ERAs – Sitaxsentan Other - TKIs - sGC stimulator - Prostacyclin receptor agonist PAH Determinants of Risk Lower Risk Determinants of Risk Higher Risk No Clinical evidence of RV failure Yes Gradual Progression Rapid II, III WHO class IV Longer (>400 m) 6MW distance Shorter (<300 m) Minimally elevated BNP Very elevated Minimal RV dysfunction Echocardiographic findings Pericardial effusion, significant RV dysfunction Normal/near normal RAP and CI Hemodynamics High RAP, low CI McLaughlin and McGoon. Circulation 2006;114:1417-31 ADULT LUNG TRANSPLANTATION Kaplan-Meier Survival By Diagnosis (Transplants: January 1994 – June 2003) 100 )N=1,127(ALPHA-1 )N= 4,888(COPD )N= 533(PPH )N= 1,934(CF )N= 2,058(IPF )N = 314(SARCOIDOSIS Survival (%) 75 50 Survival comparisons COPD vs. IPF: p < 0.0001 Alpha-1 vs. CF: p = 0.0248 Alpha-1 vs. IPF: p < 0.0001 Alpha-1 vs. PPH: p = 0.0021 CF vs. COPD: p = 0.0006 CF vs. IPF: p < 0.0001 HALF-LIFE Alpha-1: 5.1 Years; CF: 5.8 Years; COPD: 4.8 CF vs. PPH: p < 0.0001 CF vs. Sarcoidosis: p = 0.0007 Years; IPF: 3.7 Years; PPH: 4.3 Years; Sarcoidosis: 4.0 Years 25 0 0 1 2 3 4 5 6 7 8 9 Years J Heart Lung Transplant 2005;24: 945-982 10 Key Concept Summary • Differential Diagnosis – – – – Beware of the atypical patient Process of Diagnosis of Exclusion CTEPH - “curable” Associated “risk factors” • Treatment – – – – – – – Prostanoids Endothelin Receptor Antagonism Phosphodiesterase Inhibitors Riociguat Anticoagulation RV Failure Transplant Thank you Hemodynamic Profiles In PAH: LV dysfunction – “passive” PH C.O. 4 L/min TPG = 7 100 PVR = 1.75 80 45/5 60 45/25 32 25 40 20 5 0 RA RV PA PA PCW Hemodynamic Profiles In PAH: LV dysfunction – after Rx C.O. 5 L/min TPG = 6 100 PVR = 1.2 mmHg 80 60 20/2 20/8 12 6 40 20 2 0 RA RV PA PA PCW Hemodynamic Profiles In PAH: IPAH - compensated C.O. 5 L/min TPG = 40 100 80/15 80/40 52 PVR = 8 80 60 40 20 10 12 0 RA RV PA PA PCW What is the Optimal Treatment Strategy? Anticoagulate ± Diuretics ± Oxygen ± Digoxin Acute Vasoreactivity Testing Negative Positive Lower Class Risk II-III Oral CCB No Sustained Response ERAs or PDE-5 Is (oral) Epoprostenol or Treprostinil (IV) Iloprost (inhaled) Treprostinil (SC) Higher Class III-IV Risk Epoprostenol or Treprostinil (IV) Iloprost (inhaled) ERAs or PDE-5 Is (oral) Treprostinil (SC) Yes Continue CCB Reassess – consider combo-therapy Investigational Protocols Modified from Badesch DB et al. Chest. 2004;126:35S-62S. Atrial septostomy Lung Transplant PAH Basic therapy Oral anticoagulants, Diuretics, O2, Digoxin ... Acute vasoreactivity test Positive Oral CCB Sustained Response Yes Negative No CCB +++ Fall in mPAP > 10 mmHg + mPAP < 40 mmHg + Normal CO Close monitoring of long-term clinical and hemodynamic effects Continue CCB Sitbon O, et al. Circulation. 2005;111:3105-3111. 3rd World PAH Symposium. J Am Coll Cardiol 2004;43:1S-90S. ACCP Guidelines. Chest 2004;126:1S-92S. Galiè N, et al. ESC Guidelines. Eur Heart J 2004;25:2243-78. Survival in IPAH Long-term CCB Responders 1.0 Long-term CCB responders (~50% of acute responders or ≤6% of iPAH patients) P=0.0007 0.8 Cumulative survival 0.6 Long-term CCB failure 0.4 0.2 0.0 0 Subjects at risk, n 2 4 6 8 10 12 14 (Years) 38 33 30 22 13 19 12 7 4 0 Sitbon O et al. Circulation. 2005;111:3105-3111. 8 3 3 16 18 2 1 Long-term CCB responders Long-term CCB failure Prostacyclins • Epoprostenol • Treprostinil • Iloprost Epoprostenol (Flolan®) • FDA-approved for Class III-IV PAH • Chemically unstable, short half life • Continuous IV Rx • Significant SE’s • Line complications Treprostinil (Remodulin®) • FDA-approved for Class II-IV PAH • Chemically stable; longer half-life • Continuous SQ or IV; inhaled (Tyvaso) • oral under investigation • Smaller pump • Typical prostanoid SE’s • SQ limited by site pain Iloprost (Ventavis®) • • • • • • FDA-approved for Class II-IV PAH Chemically stable; longer half-life Inhaled (6-9 times daily) • IV in Europe Typical )? milder( prostanoid SE’s ? Favored for patients with parenchymal lung disease: • Provides prostacyclin activity directly to lung • Vasodilates (only?) ventilated pulmonary regions Avoids catheter complications IV Epoprostenol in IPAH: Change From Baseline in 6MW Test 40 30 31 20 Median change 10 from baseline 0 (m) P<0.002 -10 -20 -30 Epoprostenol (n=41; baseline=315 m) Barst RJ et al for the PPH Study Group. N Engl J Med. 1996;334:296-301. -29 Conventional (n=40; baseline=270 m) Long-term Outcome in IPAH With Epoprostenol Cumulative Survival % Survival 1 100 Observed (n=162) 0.8 80 * 0.6 IV Epoprostenol (n=178) * 60 0.4 * P<0.0001 0.2 Historical Control (n=135) 0 Expected 40 *P<0.001 20 0 12 24 36 48 60 72 84 Months 96 108 120 No. at risk: 178 129 85 57 36 21 7 3 1 IV Epoprostenol 135 59 34 20 11 2 2 1 Historical Control 4 McLaughlin VV et al. Circulation. 2002;106:1477-1482. Sitbon O et al. J Am Coll Cardiol. 2002;40:780-788. 0 6 12 18 24 Months 30 36 Subcutaneous Treprostinil: Change From Baseline in 6MW Test by Dose Quartile 50 36.1±10 40 Mean change from baseline (m) 20±8 30 20 3.3±10 10 0 1st Quartile <5 (n=45) 1.4±9 2nd Quartile 3rd Quartile 5 to <8.2 8.2 to <13.8 (n=55) (n=49) ng/kg/min Simonneau G et al. Am J Respir Crit Care Med. 2002;165:800-804. 4th Quartile >13.8 (n=53) Inhaled Iloprost: Change from Baseline in 6MW Test (AIR Trial) 40 30 Placebo (n=102) Iloprost (n=101) P=0.004 20 Mean change from baseline (m) 10 0 -10 -20 -30 -40 Week 4 Week 8 AIR=Aerosolized Iloprost Randomized. 6MW test was not the primary endpoint in the AIR trial. Olschewski H et al for the Aerosolized Iloprost Randomized Study Group. N Engl J Med. 2002;347:322-329. Week 12 Endothelin Receptor Antagonists - FDA approved for class III-IV PAH - Fluid retention - Oral, well-tolerated - Teratogens • Bosentan (Tracleer) • Mixed ETA/ETB antagonist • BID • LFTs • Ambrisentan (Letairis) • ETA specificity • Unique metabolism, ? lack of drug-drug interaction • Once daily Bosentan: 6-Minute Walk Test Mean change from baseline (m) Study 351 100 BREATHE-1 60 Bosentan (n=21) 80 Bosentan (n=144) 40 60 40 20 P=0.0002 20 0 0 -20 Placebo (n=11) -40 -20 -60 Baseline Placebo (n=69) -40 4 8 12 Week 20 Baseline 4 8 Week Values are mean±SEM. Channick RN et al. Lancet. 2001;358:1119-1123. Rubin LJ et al for the Bosentan Randomized Trial of Endothelin Antagonist Therapy Study Group. N Engl J Med. 2002;346;896-903. 16 PDE 5 Inhibitors • Sildenafil (Viagra, Revatio) • FDA approved for class II-IV PAH • Oral, well-tolerated • Usual PDE 5 inhibitor concerns • Tadalafil (Cialis, Adcirca) • Once daily Sildenafil: Change from Baseline in 6MW Test 80 * * 46 m 60 45 m *P<0.001 * Mean change from baseline 20 (m) 0 Week 4 Week 8 Week 12 -20 -40 Placebo (n=65) Sildenafil 20 mg tid (n=65) Sildenafil 40 mg tid (n=63) Sildenafil 80 mg tid (n=65) Galiè N et al for the Sildenafil Use in Pulmonary Arterial Hypertension (SUPER) Study Group. N Engl J Med. 2005;353:2148–2157. 50 m 40 New Directions in PAH • New treatments • New delivery strategies • Treprostinil, reformulated Iloprost • Drug combos • FREEDOM, COMPASS 2 (and many more) • New assessments • Genomics/proteomics/etc. • RV studies • New (related) disease states • Groups II, III, IV and V Pregnancy in PAH • Maternal death rate is 30-50% • Majority of deaths occur in the first week following delivery • Maternal mortality increased by hypovolemia, thromboemboli, and preeclampsia/eclampsia • Poor fetal outcome with only 25% of all pregnancies reaching term