Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Electrocardiography wikipedia , lookup
Saturated fat and cardiovascular disease wikipedia , lookup
Cardiovascular disease wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Jatene procedure wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
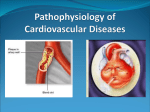
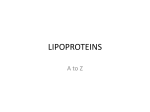
Vascular disorders are responsible for more morbidity and mortality than any other category of human disease. Although the most clinically significant lesions typically involve arteries, venous diseases also occur. Vascular pathology results in disease via two principal mechanisms: (1) Narrowing (stenosis) or complete obstruction of vessel lumens, either progressively (e.g., by atherosclerosis) or precipitously (e.g., by thrombosis or embolism). (2) weakening of vessel walls, leading to dilation or rupture. 2 3 Atherosclerosis literally means “hardening of the arteries”; it is a generic term reflecting arterial wall thickening and loss of elasticity. There are three general patterns: - Arteriolosclerosis affects small arteries and arterioles, and may cause downstream ischemic injury. - Mönckeberg medial sclerosis is characterized by calcific deposits in muscular arteries in persons typically older than age 50. - Atherosclerosis, from Greek root words for “gruel” and “hardening,” is the most frequent and clinically important pattern. 4 Atherosclerosis is characterized by intimal lesions called atheromas (also called atheromatous or atherosclerotic plaques) that protrude into vessel lumens. An atheromatous plaque consists of a raised lesion with a soft, yellow, grumous core of lipid (mainly cholesterol and cholesterol esters) covered by a white fibrous cap. Atherosclerotic plaques can: - obstruct blood flow - rupture leading to thrombosis - weaken the underlying media and thereby lead to aneurysm formation 5 The major components of a well-developed intimal atheromatous plaque overlying an intact media. 6 7 Etiology and Pathophysiology lipid-laden macrophage Chronic stable angina Relationship between atherosclerotic plaque encroachment in the coronary lumen (coronary blood flow) and the resulting influence of myocardial supply and demand Atherosclerosis Atherosclerotic plaque development Plaque rupture Platelet activation/aggregation Thrombus formation – incomplete/complete Coronary artery disease (CAD) and ischemic heart disease (IHD) are important manifestations of the atherosclerosis. The prevalence and severity of atherosclerosis and IHD are related to two groups of risk factors: 1. Constitutional (non-modifiable) 2. Acquired (modifiable) or related to behaviours that are potentially amenable to intervention 10 Constitutional risk factors in IHD: - Age - Gender - Genetics Modifiable risk factors in IHD: - hyperlipidemia - hypertension - cigarette smoking - diabetes mellitus 11 Additional risk factors: - Inflammation - Hyperhomocystinemia - Metabolic syndrome - Lipoprotein (a) levels - Factors affecting hemostasis - Other factors 12 Pathogenesis of Atherosclerosis Historically, there have been two dominant hypotheses to explain the progress of the disease: - one emphasizes intimal cellular proliferation. - the other focuses on the repetitive formation and organization of thrombi. Recently, the response-to-injury hypothesis which views atherosclerosis as a chronic inflammatory and healing response of the arterial wall to endothelial injury was adopted. 14 Atherosclerosis is produced by the following pathogenic events: - Endothelial injury, which causes (among other things) increased vascular permeability, leukocyte adhesion, and thrombosis. - Accumulation of lipoproteins (mainly LDL and its oxidized forms) in the vessel wall. - Monocyte adhesion to the endothelium, followed by migration into the intima and transformation into macrophages and foam cells. - Platelet adhesion. 15 - Factor release from activated platelets, macrophages, and vascular wall cells, inducing smooth muscle cell recruitment, either from the media or from circulating precursors. - Smooth muscle cell proliferation and ECM production. - Lipid accumulation both extracellularly and within cells (macrophages and smooth muscle cells). 16 17 18 Consequences of Atherosclerosis The aorta, carotid, and iliac arteries (large elastic arteries) and coronary and popliteal (medium-sized muscular arteries) are targets for atherosclerosis. Heart attack, stroke, aneurysm and gangrene in the legs are potential consequences of the disease. The principal outcomes depend on: - The size of the involved vessels - The relative stability of the plaque itself - The degree of degeneration of the underlying arterial wall 19 20 1. Atherosclerotic stenosis Compromised blood flow WILL lead to ischemic injury secondary to critical occlusion of a small vessel. Total circumference expansion due to outward remodelling of vessel media is an adaptive mechanism before an injury commences. At 70% fixed occlusion, clinical symptoms surface (Stable angina). The effects of vascular occlusion ultimately depend on arterial supply and the metabolic demand of the affected tissue. 21 2. Acute plaque change Plaque rupture is promptly followed by partial or complete vascular thrombosis resulting in acute tissue infarction (e.g., myocardial or cerebral infarction). Plaque changes fall into three general categories: - Rupture/fissuring, exposing highly thrombogenic plaque constituents - Erosion/ulceration, exposing the thrombogenic subendothelial basement membrane to blood - Hemorrhage into the atheroma, expanding its volume 22 The events that trigger abrupt changes in plaque configuration are complex and include: - Intrinsic factors (e.g., plaque structure and composition) - Extrinsic factors (e.g., blood pressure, platelet reactivity) 23 3. Thrombosis Thrombosis (partial/total) associated with a disrupted plaque is critical to the pathogenesis of the acute coronary syndromes. Thrombus superimposed on a disrupted partially stenotic plaque converts it to a total occlusion. In other coronary syndromes luminal obstruction by thrombosis is usually incomplete and will disappear with time. Mural thrombus in a coronary artery can also embolize 24 4. Vasoconstriction Vasoconstriction at sites of atheroma is stimulated by: (1) circulating adrenergic agonists (2) locally released platelet contents (3) impaired secretion of endothelial cell relaxing factors (nitric oxide) relative to contracting factors (endothelin) as a result of endothelial cell dysfunction (4) mediators released from perivascular inflammatory cells. 25 Hyperlipidemia Hypercholesterolemia additive to nonlipid CHD risk factors: cigarette smoking, HTN, DM, low HDL, electrocardiographic abnormalities Presence of CHD, prior MI increases MI risk 5 to 7 times LDL level: significant predictor of morbidity/mortality ~50% of MIs and > 70% of CHD deaths occur in patients with known CHD 26 Background & Pathophysiology Cholesterol: essential for cell membrane formation & hormone synthesis Lipids not present in free form in plasma; circulate as lipoproteins (complexes of lipids and proteins) 3 major classes of plasma lipoproteins: VLDL carries ~10 to 15 % of total serum cholesterol; carried in circulation as TG; VLDL = TG/5 LDL carries 60 to 70% of total serum cholesterol; IDL is also included in this group (LDL1) HDL carries 20 to 30% of total serum cholesterol; reverse transportation of cholesterol 27 Cholesterol, triglycerides, and phospholipids are the major lipids in the body. They are transported as complexes of lipid and proteins known as lipoproteins. Plasma lipoproteins are spherical particles with surfaces that consist largely of phospholipid, free cholesterol, and protein and cores composed mostly of triglyceride and cholesterol ester The figure shows a diagrammatic representation of the structure of low-density lipoprotein (LDL), the LDL receptor, and the binding of LDL to the receptor via apolipoprotein B-100. 28 29 Apoproteins These proteins have three functions: provide structure to the lipoprotein, activate enzyme systems, bind with cell receptors The five most clinically relevant apolipoproteins are A-I, A-II, B-100, C, and E the B and E proteins are ligands for LDL receptors the blood concentration of apolipoprotein B-100 is an indication of the total number of VLDL and LDL particles in the circulation. An increased number of lipoprotein particles (i.e., an increased apolipoprotein B-100 concentration) is a strong predictor of CHD risk. Apo C-II is a cofactor for lipoprotein lipase Apo C-III downregulates lipoprotein lipase activity and interferes with the hepatic uptake of VLDL remnant particles (may emerge as an important marker of atherosclerosis and provide a way for clinicians to identify patients requiring aggressive treatment.) A-I protein activates LCAT, which catalyzes the esterification of free cholesterol in HDL particles. Levels of apolipoprotein A-I have a stronger inverse correlation with CHD risk than apolipoprotein A-II levels. HDL particles that contain only A-I apolipoproteins (LpA-I) are associated with a lower CHD risk than are HDL particles containing both A-I and A-II (LpA-I, A-II). 30 31 Chylomicron VLDL LDL HDL <0.94 0.94–1.006 1.006–1.063 1.063–1.210 Protein 1–2 6–10 18–22 45–55 Triglyceride 85–95 50–65 4–8 2–7 Cholesterol 3–7 20–30 51–58 18–25 Phospholipid 3–6 15–20 18–24 26–32 Physiologic origin Intestine Intestine and liver Product of VLDL catabolism Liver and intestine Physiologic function Transport dietary CH and TG to liver Transport endogenous TG and CH Transport Transport CH endogenous CH from cells to to cells liver Plasma appearance Cream layer Turbid Clear Clear Electrophoretic mobility Origin Pre-beta Beta Alpha B-100, C-I, C-II, C-III, E B-100, A-I, A-II, A-IV Density (g/mL) Composition (%) Apolipoproteins A-IV, B-48, C-I, C-II, C-III 32 Background & Pathophysiology VLDL secreted from the liver converted to IDL then LDL Plasma LDL taken up by receptors on liver, adrenal, & peripheral cells recognize LDL apolipoprotein B-100 LDL internalized & degraded by these cells Increased intracellular cholesterol levels inhibits HMG-CoA reductase & decreases LDL receptor synthesis Decreases in LDL receptors: plasma LDL not as readily taken up & broken down by cells 33 Background & Pathophysiology LDL also excreted in bile joins enterohepatic pool eliminated in stool LDL can be oxidized in subendothelial space of arteries Oxidized LDL in artery walls provokes inflammatory response Monocytes recruited & transformed into macrophages results in cholesterol laden foam cell accumulation Foam cells: beginning of arterial fatty streak If processes continue: angina, stroke, MI, peripheral artery disease, arrhythmias, death 34 35 Biosynthetic pathway for cholesterol. The rate-limiting enzyme in this pathway is 3-hydroxy-3methylglutaryl coenzyme A reductase (HMG-CoA reductase). (CETP, cholesterol ester transfer protein; HDL, high-density lipoprotein; IDL, intermediate-density lipoprotein; LDL, low-density lipoprotein; LPL, lipoprotein lipase; VLDL, very-low-density lipoprotein.) 36 Etiology There are two major ways in which dyslipidemias are classified: Phenotype, or the presentation in the body (including the specific type of lipid that is increased) Etiology, or the reason for the condition (genetic (primary), or secondary to another condition.) This classification can be problematic, because most conditions involve the intersection of genetics and lifestyle issues. However, there are a few well defined genetic conditions that are usually easy to identify. Current laboratory values can not define underlying abnormality Secondary dyslipidemias and should be initially managed by correcting underlying abnormality when possible 38 38 Etiology Primary lipoprotein disorders: 6 categories used for phenotypical description of dyslipidemia Fredrickson-Levy-Lees Classification Type Lipoprotein Elevation Effect on lipid profile I Chylomicrons ↑↑TG, ↑cholesterol IIa LDL ↑cholesterol IIb LDL + VLDL ↑cholesterol, ↑TG III IDL (LDL1) ↑cholesterol, ↑TG IV VLDL ↑TG, moderate ↑cholesterol V VLDL + Chylomicrons ↑↑TG, ↑cholesterol 39 Lipid Phenotype Plasma Lipids [mmol/L (mg/dL)] Lipoprotein Elevated Pheno- Clinical Signs type Heterozygotes TC = 7–13 (275–500) LDL IIa Usually develop xanthomas in adulthood and vascular disease at 30–50 years (LDL receptors) Homozygotes TC >13 (>500) LDL IIa Usually develop xanthomas in adulthood and vascular disease in childhood Familial defective Apo B-100 Heterozygotes TC = 7–13 (275–500) LDL IIa Polygenic hypercholesterolemia (genetic/lifestyle) TC = 6.5–9 (250– 350) LDL IIa Usually asymptomatic until vascular disease develops; no xanthomas Isolated hypercholesterolemia Familial hypercholesterolemia Isolated hypertriglyceridemia Familial hypertriglyceridemia TG = 2.8–8.5 (250– 750) VLDL IV Asymptomatic; may be associated with increased risk of vascular disease Familial LPL deficiency TG >8.5 (>750) Chylomicrons, VLDL I, V May be asymptomatic; may be associated with pancreatitis, abdominal pain, hepatosplenomegaly Familial Apo C-II deficiency TG >8.5 (>750) Chylomicrons, VLDL I, V As above 41 Lipid Phenotype Plasma Lipid Levels [mmol/L (mg/dL)] Lipoprotein Elevated Phenotype Clinical Signs Hypertriglyceridemia and hypercholesterolemia Combined hyperlipidemia TG = 2.8–8.5 (250–750); TC = 6.5–13 (250–500) VLDL, LDL IIb Usually asymptomatic until vascular disease develops; familial form may present as isolated high TG or isolated high LDL cholesterol Dysbetalipoproteinemia TG = 2.8–8.5 (250–750); TC = 6.5–13 (250–500) VLDL, IDL; LDL normal III Usually asymptomatic until vascular disease develops; may have palmar or tuboeruptive xanthomas (Apo E) Note: Elevated cholesterol is not necessarily familial hypercholesterolemia (type IIa) *cholesterol may be elevated in other lipoprotein disorders *lipoprotein pattern does not describe underlying genetic defect 42 Main Lipid Parameter Diagnostic Features Disorder Metabolic Defect Lipid Effect Polygenic hypercholesterolemia ↓LDL clearance ↑LDL-C LDL-C: 130–250 mg/dL TG: 150–500 mg/dL None distinctive Atherogenic dyslipidemia ↑VLDL secretion, ↑C-III synthesis ↓LPL activity ↓VLDL removal ↑TG ↑Remnant VLDL ↓HDL ↑Small, dense LDL HDL-C: <40 mg/dL Frequently accompanied by central obesity or diabetes Familial hypercholesterolemia (heterozygous) Dysfunctional or absent LDL receptors ↑LDL-C LDL-C: 250–450 mg/dL Family history of CHD, tendon xanthomas Familial defective apoB-100 Defective ApoB on LDL and VLDL ↑LDL-C LDL-C: 250–450 mg/dL Family history of CHD, tendon xanthomas Dysbetalipoproteinemia (type III hyperlipidemia) ApoE2:E2 phenotype, ↓VLDL remnant clearance ↑Remnant VLDL, ↑IDL LDL-C: 300–600 mg/dL TGs: 400–800 mg/dL Palmar xanthomas, tuberoeruptive xanthomas Familial combined hyperlipidemia ↑ApoB and VLDL production ↑CH, TG, or both LDL-C: 250–350 mg/dL TGs: 200–800 mg/dL Family history, CHD Family history, Hyperlipidemia Familial hyperapobetalipoproteinemia ↑ApoB production ↑ApoB ApoB: >125 mg/dL None distinctive Hypoalphalipoproteinemia ↑HDL catabolism ↓HDL-C HDL-C: <40 mg/dL None distinctive Xanthomas Xanthomas are plaques or nodules consisting of abnormal lipid deposition and foam cells. They do not represent a disease but rather are symptoms of different lipoprotein disorders or arise without an underlying metabolic effect. Clinically, xanthomas can be classified as: eruptive, tuberoeruptive or tuberous, tendinous, or planar. Planar xanthomas include: xanthelasma palpebrarum/xanthelasma, xanthoma striatum palmare, intertriginous xanthomas. There are characteristic clinical phenotypes associated with specific metabolic defects Tuberoeruptive and tuberous xanthomata typical of familial dysbetalipoproteinemia. A. Knee B. Palm. Eruptive skin xanthomata characteristic of severe chylomicronemia. Tendon xanthomata typical of heterozygous familial hypercholesterolemia. Similar xanthomata occur in patients with familial defective apolipoprotein B100, cerebrotendinous xanthomatosis, and sitosterolemia. Xanthoma striatum palmare characteristic of familial dysbetalipoproteinemia. Forms of xanthomas and other lipid deposits frequently seen in familial hypercholesterolemia homozygotes. A. Arcus corneae. B, C, E, and F. Cutaneous planar xanthomas, which usually have a bright orange hue. D and G. Tuberous xanthomas on the elbows. H. Tendon and tuberous xanthomas. Familial hypercholesterolemia characterized by a. selective elevation in the plasma level of LDL, b. deposition of LDL-derived cholesterol in tendons (xanthomas) and arteries (atheromas), c. inheritance as an autosomal dominant trait with homozygotes more severely affected than heterozygotes. The primary defect in familial hypercholesterolemia is the inability to bind LDL to the LDL receptor or, rarely, a defect of internalizing the LDL receptor complex into the cell after normal binding. Homozygotes have essentially no functional LDL receptors. This leads to lack of LDL degradation by cells and unregulated biosynthesis of cholesterol, with total cholesterol and LDL-C inversely proportional to the deficit in LDL receptors. Heterozygotes have only about half the normal number of LDL receptors, total cholesterol levels in the range from 300 to 600 mg/dL. Familial LPL deficiency LPL is normally released from vascular endothelium or by heparin and hydrolyzes chylomicrons and VLDL Familial LPL deficiency is a rare, autosomal recessive trait Diagnosis is based on low or absent enzyme activity with normal human plasma or apolipoprotein CII, a cofactor of the enzyme. Type I lipoprotein pattern characterized by massive accumulation of chylomicrons and corresponding increase in plasma triglycerides. VLDL concentration is normal. Presenting manifestations include repeated attacks of pancreatitis and abdominal pain, eruptive cutaneous xanthomatosis, and hepatosplenomegaly beginning in childhood. Symptom severity is proportional to dietary fat intake and consequently to the elevation of chylomicrons. Accelerated atherosclerosis is not associated with the disease. type V (VLDL and chylomicrons). Abdominal pain, pancreatitis, eruptive xanthomas, and peripheral polyneuropathy Symptoms may occur in childhood, but usually the disorder is expressed at a later age. The risk of atherosclerosis is increased with the disorder. Patients commonly are obese, hyperuricemic, and diabetic, and alcohol intake, exogenous estrogens, and renal insufficiency tend to be exacerbating factors. Dysbetalipoproteinemia familial type III hyperlipoproteinemia (also called, broad-band, or β-VLDL) Patients develop the following clinical features after age 20 years: xanthoma striata palmaris (yellow discolorations of the palmar and digital creases); tuberous or tuberoeruptive xanthomas (bulbous cutaneous xanthomas); severe atherosclerosis involving the coronary arteries, internal carotids, and abdominal aorta. A defective structure of apolipoprotein E does not allow normal hepatic surface receptor binding of remnant particles derived from chylomicrons and VLDL (known as IDL). Aggravating factors such as obesity, diabetes, and pregnancy may promote overproduction of apolipoprotein B–containing lipoproteins. Although homozygosity for the defective allele (E2/E2) is common (1:100), only 1 in 10,000 express the full-blown picture, and interaction with other genetic or environmental factors, or both, is needed to produce clinical disease. Familial combined hyperlipidemia characterized by elevations in total cholesterol and triglycerides, decreased HDL, increased apolipoprotein B, and small, dense LDL. It is associated with premature CHD and may be difficult to diagnose because lipid levels do not consistently display the same pattern. Type IV hyperlipoproteinemia Two genetic patterns: familial hypertriglyceridemia, which does not carry a great risk for premature CAD, familial combined hyperlipidemia, which is associated with increased risk for cardiovascular disease. Type IV hyperlipoproteinemia is common and occurs in adults, primarily in patients who are obese, diabetic, and hyperuricemic and do not have xanthomas. It may be secondary to alcohol ingestion and can be aggravated by stress, progestins, oral contraceptives, thiazides, or β-blockers. Lipoprotein Abnormalities: 2˚ Causes Hypercholesterolemia hypothyroidism obstructive liver disease nephrotic syndrome anorexia nervosa acute intermittent porphyria Medications progestins thiazide diuretics glucocorticoids β-blockers isotretinoin protease inhibitors cyclosporine mirtazipine sirolimus Lipoprotein Abnormalities: 2˚ Causes Hypertriglyceridemia obesity DM lipodystrophy glycogen storage disease • Medications • alcohol • estrogens • isotretinoin • β-blockers • glucocorticoids ileal bypass surgery • bile acid resins sepsis • asparaginase Pregnancy monocolonal gammopathy: multiple myeloma, lymphoma acute hepatitis systemic lupus erythematous • Thiazides • interferons • azole antifungals • mirtazipine • anabolic steroids • sirolimus 54 Lipoprotein Abnormalities: 2˚ Causes Hypocholesterolemia malnutrition malabsorption myeloproliferative diseases chronic infectious diseases acquired immune deficiency syndrome tuberculosis Low high-density lipoprotein malnutrition obesity Medications non-ISA β-blockers anabolic steroids isotretinoin progestins monoclonal gammopathy chronic liver disease 55 55 Metabolic syndrome Any 3 or more of the following are needed for diagnosis 57 Total cholesterol <200 200–239 240 LDL cholesterol <100 100–129 130–159 160–189 190 HDL cholesterol <40 60 mg/dL Triglycerides <150 150–199 200–499 500 Desirable Borderline high High Optimal Near or above optimal Borderline high High Very high Low High Normal Borderline high High Very high All values are mg/dL 58 Major risk factorsa – exclusive of LDL-C – that modify the LDL goals Age Men: > 45 years Women: > 55 years or premature menopause without estrogen replacement therapy Family history of premature CHD (definite myocardial infarction or sudden death before age 55 years in father or other male first-degree relative, or before age 65 years in mother or other female first-degree relative) Cigarette smoking Within the past month Hypertension (140/90 mm Hg or taking antihypertensive medication) Low HDL cholesterol (<40 mg/dL)b aDiabetes regarded as coronary heart disease (CHD) risk equivalent. bHDL cholesterol >60 mg/dL counts as "negative" risk factor; its presence removes one risk factor from the total count. Metabolic syndrome is considered as CHD risk equivalent 59 Goals & Cutpoints Risk Category LDL Goal (mg/dL) LDL Level at Which to Initiate TLC (mg/dL) LDL Level at Which to Consider Drug Therapy High risk: CHD or CHD risk equivalents (10-year risk >20%) <100 (optional goal: <70) >100 >100 (<100 mg/dL; consider drug options)a Moderately high risk: 2+ risk factors (10-year risk >10%–20%) <130 (optional goal <100) >130 >130 (100–129: consider drug options) Moderate risk: 2+ risk factors (10-year risk <10%) <130 >130 >160 Lower risk: 0–1 risk factorb <160 >160 >190 (160–189: LDL-lowering drug optional) Risk is estimated from Framingham risk score aSome authorities recommend use of LDL-lowering drugs in this category if LDL cholesterol <100 mg/dL cannot be achieved by therapeutic lifestyle changes (TLC). Others prefer to use drugs that primarily modify triglycerides and high-density lipoprotein, e.g., nicotinic acid or fibrates. Clinical judgment also may call for deferring drug therapy in this subcategory. bAlmost all people with 0–1 risk factor have a 10-year risk <10%; thus,10-year risk assessment in people with 0–1 risk factor is not necessary. 60 Patient Assessment Lab - definitions • The ACCURACY of a measurement system is the degree of closeness of measurements of a quantity to its actual (true) value. • The PRECISION of a measurement system, also called reproducibility or repeatability, is the degree to which repeated measurements under unchanged conditions show the same results. • SENSITIVITY (also called recall rate in some fields) measures the proportion of actual positives which are correctly identified as such (e.g. the percentage of sick people who are correctly identified as having the condition). • SPECIFICITY measures the proportion of negatives which are correctly identified (e.g. the percentage of healthy people who are correctly identified as not having the condition). • VALIDITY refers to the degree to which evidence and theory support the interpretations of test scores entailed by proposed uses of tests. 61 62 Calculation of LDL-c The majority of labs, including the insurance labs, do not directly measure the LDL portion of the lipid profile. On the other hand, total cholesterol, HDL and triglycerides are directly measured with values determined for each of these three tests. LDL is usually not measured directly due to the expense and time required to perform the analysis. Therefore, to estimate LDL, labs use the “FRIEDEWALD FORMULA” which is (in mg/dl): VLDL 63 64 Hypertension Persistent elevation of arterial blood pressure (BP) National Guideline 7th Report of the Joint National Committee on the Detection, Evaluation, and Treatment of High Blood Pressure (JNC7) ~72 million Americans (31%) have BP > 140/90 mmHg Most patients asymptomatic Cardiovascular morbidity & mortality risk directly correlated with BP; antihypertensive drug therapy reduces cardiovascular & mortality risk Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003;42(6):1206–1252. 65 Target-Organ Damage Brain: stroke, transient ischemic attack, dementia Eyes: retinopathy Heart: left ventricular hypertrophy, angina Kidney: chronic kidney disease Peripheral Vasculature: peripheral arterial disease 66 67 Etiology Essential hypertension: > 90% of cases hereditary component Secondary hypertension: < 10% of cases common causes: chronic kidney disease, renovascular disease other causes: Rx drugs, street drugs, natural products, food, industrial chemicals 68 Causes of 2˚ Hypertension Diseases chronic kidney disease Cushing's syndrome coarctation of the aorta obstructive sleep apnea parathyroid disease pheochromocytoma primary aldosteronism renovascular disease thyroid disease 69 Causes of 2˚ Hypertension Prescription drugs: prednisone, fludrocortisone, triamcinolone amphetamines/anorexiants: phendimetrazine, phentermine, sibutramine antivascular endothelin growth factor agents estrogens: usually oral contraceptives calcineurin inhibitors: cyclosporine, tacrolimus decongestants: phenylpropanolamine & analogs erythropoiesis stimulating agents: erythropoietin, darbepoietin 70 Causes of 2˚ Hypertension Prescription drugs: NSAIDs, COX-2 inhibitors venlafaxine bupropion bromocriptine buspirone carbamazepine clozapine ketamine metoclopramide 71 Causes of 2˚ Hypertension Situations: β-blocker or centrally acting α-agonists when abruptly discontinued β-blocker without α-blocker first when treating pheochromocytoma Food substances: sodium ethanol licorice 72 Causes of 2˚ Hypertension Street drugs, other natural products: cocaine anabolic steroids cocaine withdrawal narcotic withdrawal ephedra alkaloids methylphenidate (e.g., ma-huang) “herbal ecstasy” phenylpropanolamine analogs nicotine withdrawal phencyclidine ketamine ergot-containing herbal products St. John's wort 73 Mechanisms of Pathogenesis Increased cardiac output (CO): increased preload: increased fluid volume excess sodium intake renal sodium retention venous constriction: excess RAAS stimulation sympathetic nervous system overactivity 74 Mechanisms of Pathogenesis Increased peripheral resistance (PR): functional vascular constriction: excess RAAS stimulation sympathetic nervous system overactivity genetic alterations of cell membranes endothelial-derived factors structural vascular hypertrophy: excess RAAS stimulation sympathetic nervous system overactivity genetic alterations of cell membranes endothelial-derived factors hyperinsulinemia due to obesity, metabolic syndrome 75 Arterial Blood Pressure Sphygmomanometry: indirect BP measurement MAP = 1/3 (SBP) + 2/3 (DBP) BP = CO x TPR MAP: Mean Arterial Pressure SBP: Systolic Blood Pressure DBP: Diastolic Blood Pressure BP: Blood Pressure CO: Cardiac Output TPR: Total Peripheral Resistance 76 Arterial Pressure Determinants 77 Adult Classification Classification Normal Systolic Blood Pressure (mmHg) Diastolic Blood Pressure (mmHg) Less than 120 and Less than 80 Prehypertension 120-139 or 80-89 Stage 1 hypertension 140-159 or 90-99 Stage 2 hypertension > 160 or > 100 Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003;42(6):1206–1252. 78 Heart Failure Progressive clinical syndrome Results from the heart’s inability to pump sufficient blood to meet the body’s metabolic needs Can occur from any disorder damaging the pericardium, heart valves, myocardium, or ventricle function Outdated term “congestive heart failure” inaccurate because patients may present without congestion 79 Epidemiology ~5.7 million Americans had HF in 2006 670,000 more cases diagnosed each year Incidence, prevalence, & hospitalization rates of heart failure are increasing Annual hospital discharges > 1 million Direct & indirect costs for 2009 ~$37.2 billion Overall 5-year survival rate ~50% Lloyd-Jones D, Adams R, Carnethon M, et al. Heart disease and stroke statistics—2009 update: A report from the American Heart 80 Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 2009;117:e21–e181. Epidemiology Factors affecting prognosis: age gender LVEF renal function blood pressure HF etiology drug or device therapy 81 Etiology Can result from any disorder that affects the hearts ability to contract &/or relax Classic familiar form: impaired systolic function (i.e. reduced LVEF) Studies suggest up to 50% heart failure patients have preserved LVEF with presumed diastolic dysfunction usually elderly, female, obese, HTN, atrial fibrillation, DM Frequently, patients have coexisting systolic & diastolic dysfunction 82 HF Causes Coronary artery disease: most common cause ~70% of cases Ischemic heart disease &/or HTN contribute to development of HF Systolic dysfunction (decreased contractility) reduction in muscle mass (e.g. myocardial infarction) dilated cardiomyopathies ventricular hypertrophy pressure overload (e.g. systemic or pulmonary hypertension, aortic or pulmonic valve stenosis) volume overload (e.g. valvular regurgitation, shunts, high output states) 83 HF Causes Diastolic dysfunction restricted ventricular filling, increased ventricular stiffness ventricular hypertrophy, hypertrophic cardiomyopathy infiltrative myocardial diseases: amyloidosis, sarcoidosis, endomyocardial fibrosis myocardial ischemia & infarction mitral or tricuspid valve stenosis pericardial disease pericarditis, pericardial tamponade 84 85 Pathophysiology CO: volume of blood ejected per unit time (L/min) CO = HR x SV MAP = CO x SVR In normal LV function, increasing SVR has little effect on SV preload: 1˚ mechanism affecting CO As LV dysfunction increases, the negative inverse relationship between SV & SVR becomes more important 86 87 88 Compensatory Mechanisms in HF The heart’s decrease in pumping capacity results in compensatory responses to maintain CO Responses are intended to be short term after acute reductions in BP or renal perfusion Persistent decline in CO in HF results in long term activation of compensatory responses leading to functional, structural, biochemical, molecular changes 89 Compensatory Responses in HF Compensatory Response Beneficial Effects of Compensation Detrimental Effects of Compensation Increased preload Optimize stroke-volume via Frank(through Na+ & Starling mechanism water retention) Pulmonary and systemic congestion and edema formation Increased MVO2 Vasoconstriction Maintain BP in face of reduced CO Shunt blood from nonessential organs to brain and heart Increased MVO2 Increased afterload decreases stroke volume and further activates the compensatory responses Tachycardia and increased contractility (because of SNS activation) Helps maintain CO Increased MVO2 Shortened diastolic filling time β1-receptor downregulation, decreased receptor sensitivity Precipitation of ventricular arrhythmias Increased risk of myocardial cell death Ventricular hypertrophy and remodeling Helps maintain CO Reduces myocardial wall stress Decreases MVO2 Diastolic dysfunction Systolic dysfunction Increased risk of myocardial cell death Increased risk of myocardial ischemia Increased arrhythmia risk Fibrosis DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy: A Pathophysiologic Approach, 7th Edition: http://www.accesspharmacy.com 90 91 Compensatory Responses in HF Tachycardia & increased contractility primarily results from NE release CO increases until diastolic filling is compromised (HR 170 to 200 bpm) Fluid retention & increased preload decreased CO leads to reduced perfusion of other organs including the kidneys activation of renal-angiotensin-aldosterone system (RAAS) Na+ & H2O retention increase preload to increase CO in chronic HF, increases in preload have smaller effects on SV than in normal hearts 92 93 94 Compensatory Responses in HF Vasoconstriction & increased afterload helps redistribute blood flow away from nonessential organs to coronary & cerebral blood vessels; increases afterload increased afterload leads to decreased CO Ventricular hypertrophy & remodeling key component of pathology progression remodeling affects the heart at molecular & cellular levels major focus for therapeutic interventions therapies that reverse modeling, decrease mortality, slow disease progression 95 96 HF Models Older paradigms cardiorenal model problem viewed as excess Na+ & H2O diuretics main therapy cardiocirculatory model problem viewed as impaired CO main therapies are positive inotropes, vasodilators 97 Neurohormonal HF Model Current paradigm: neurohormonal model initiating event leads to decreased CO becomes progressive systemic disease mediated by neurohormones & autocrine/paracrine factors not a full explanation: drug therapies that target neurohormonal imbalances slow progression but do not stop disease progression 98 Neurohormones Angiotensin II increases SVR, heightens SNS activation, promotes Na+ retention maintains perfusion pressure in severe HF impaired renal function ACE inhibitor/ARB initiation cause transient renal impairment stimulates ventricular hypertrophy, remodeling, myocyte apoptosis, oxidative stress, inflammation, extracellular matrix alterations blocking angiotensin II with ACE-inhibitors or ARBs prolongs survival 99 Neurohormones Norepinephrine effects tachycardia vasoconstriction increased contractility β1-receptor down regulation increased risk of arrhythmias myocardial cell loss contributes to hypertrophy, remodeling 100 Neurohormones Norepinephrine SNS activation through β-agonists & phosphodiesterase inhibitors increases mortality in HF patients β-blockers, ACE inhibitors, digoxin decrease SNS activation beneficial in HF β-blockers & ACE inhibitors decrease mortality digoxin does not decrease mortality but improves symptoms 101 Neurohormones Aldosterone enhances Na+ retention produces interstitial cardiac fibrosis: decreases systolic & diastolic function causes other target organ fibrosis, vascular remodeling, proinflammatory state, oxidative stress increases risk of arrhythmias aldosterone antagonists reduce mortality 102 Neurohormones Natriuretic Peptides Atrial natriuretic peptide (ANP) B-type natriuretic peptide (BNP) C-type natriuretic peptide (CNP) elevated ANP & BNP in HF natriuresis diuresis vasodilation decreased aldosterone release decreased hypertrophy SNS & RAAS inhibition 103 Neurohormones Natriuretic Peptides increased BNP increased mortality, risk of sudden death, symptoms, hospitalization BNP assays (either BNP or N-terminal pro-BNP) help with HF diagnosis controversial whether BNP should be used to guide therapy recombinant human BNP (nesiritide) short-term hemodynamic & symptom improvement in acute HF 104 Neurohormones Arginine Vasopressin AVP: pituitary peptide hormone that regulates renal H2O & solute excretion to maintain fluid homeostasis increased AVP in HF causes increased free renal H2O reabsorption volume overload hyponatremia increased arterial vasoconstriction reduced CO stimulates cardiac remodeling 105 Neurohormones Arginine Vasopressin tolvaptan blocks the V2 receptor; increases serum Na+ & urine output FDA approved for treatment of clinically significant hypervolemic & euvolemic hyponatremia including patients with HF, cirrhosis, & Syndrome of Inappropriate Antidiuretic Hormone (SIADH) no effect on HR, BP, renal function, other electrolytes AVP antagonists may be useful in volume overloaded patients with hyponatremia 106 Autocrine/Paracrine Factors Other circulating mediators proinflammatory cytokines TNF-α, IL-6, IL-1β negative inotropic effects reduced β-receptor-mediated responses increased myocardial cell apoptosis stimulate remodeling anti-TNFα agents no improvement in outcomes during clinical trials 107 Autocrine/Paracrine Factors Other circulating mediators endothelin peptides are potent vasoconstrictors endothelin-1 has direct cardiotoxic & antiarrhythmogenic effects, stimulating cardiac myocyte hypertrophy endothelin-receptor antagonists have shown no benefit inflammatory & endothelial dysfunction in HF generated interest in statins for possible pleiotriopic effects on going trials assessing mortality will clarify role of statins in HF treatment 108 HF Exacerbation Previously compensated patients may develop worsening symptoms that require hospitalization Factors that exacerbate or may precipitate HF negative inotropic effects direct cardiotoxicity increased Na+ &/or H2O retention symptoms of volume overload with hypoperfusion in severe cases 109 HF Exacerbation Causes noncompliance with medications & dietary recommendations (Na+ & H2O restrictions) cardiac events: MI & ischemia, coronary artery disease, atrial fibrillation non-cardiac events: pulmonary infection, anemia inadequate/inappropriate medications Most causes are preventable 110 Drugs That Exacerbate HF Negative inotropic effect Cardiotoxic antiarrhythmics doxorubicin β-blockers daunomycin calcium channel blockers cyclophosphamide verapamil trastuzumab diltiazem imatinib itraconazole ethanol terbenafine amphetamines cocaine methamphetamine 111 Drugs That Exacerbate HF Na+ & H2O retention nonsteroidal anti-inflammatory drugs cyclooxygenase-2 inhibitors rosiglitazone, pioglitazone glucocorticoids androgens, estrogens salicylates (high dose) Na+ containing drugs carbenicillin disodium ticarcillin disodium 112 Vascular injury and thrombosis Coagulation Cascade Traditionally, the coagulation cascade has been divided into three distinct parts: the intrinsic, the extrinsic, and the common pathways. There are numerous interactions between the three pathways. Ischemic Heart Disease Caused by epicardial vessel atherosclerosis which leads to coronary heart disease Presentation: acute coronary syndrome chronic stable exertional angina pectoris ischemia without clinical symptoms heart failure, arrhythmias cerebrovascular disease peripheral vascular disease 115 Epidemiology ~79 million American adults: > 1 type of cardiovascular disease (CVD) ~2,400 Americans die of CVD each day average of 1 death every 33 seconds In 2004, CHD was responsible for 52% of CVD deaths Common initial presentation: women: angina men: myocardial infarction Rosamond W, Flegal K, Friday G, et al. Heart disease and stroke statistics—2007 update: A report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 2007;115:69–171. 116 Angina Classified by symptom severity, disability, specific activity scale Number of vessels obstructed important determinate of outcome Risk factors for increased mortality: heart failure smoking left main or left main equivalent CAD diabetes prior MI 117 Grading of Angina Pectoris by the Canadian Cardiovascular Society Classification System Class Class I Class II Class III Class IV Description of Stage Ordinary physical activity does not cause angina, such as walking, climbing stairs. Angina occurs with strenuous, rapid, or prolonged exertion at work or recreation. Slight limitation or ordinary activity. Angina occurs on walking or climbing stairs rapidly, walking uphill, walking or stair climbing after meals, or in cold, or in wind, or under emotional stress, or only during the few hours after wakening. Walking more than 2 blocks on the level and climbing more than 1 flight of ordinary stairs at a normal pace and in normal condition. Marked limitations of ordinary physical activity. Angina occurs on walking 1 to 2 blocks on the level and climbing 1 flight of stairs in normal conditions and at a normal pace. Inability to carry on any physical activity without discomfort— anginal symptoms may be present at rest. DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy: A Pathophysiologic Approach, 7th Edition: http://www.accesspharmacy.com 118 Etiology/Pathophysiology Coronary atherosclerotic plaque formation leads to imbalance between O2 supply & demand myocardial ischemia Ischemia: lack of O2, decreased or no blood flow in myocardium Anoxia: absence of O2 to myocardium 119 Etiology/Pathophysiology Determinants of myocardial oxygen demand (MVO2) HR contractility intramyocardial wall tension during systole (most important) Determinants of ischemia: resistance in vessels delivering blood to myocardium MVO2 120 Etiology/Pathophysiology Coronary blood flow inversely related to arteriolar resistance directly related to coronary driving pressure Extent of functional obstruction important limitation of coronary blood flow severe stenosis (> 70%) ischemia & symptoms at rest 121 122 Etiology/Pathophysiology Changes in O2 balance lead to rapid changes in coronary blood flow Mediators that affect O2 balance: adenosine other nucleotides nitric oxide prostaglandins CO2 H+ 123 Etiology/Pathophysiology Extrinsic factors alterations in intramyocardial wall tension throughout the cardiac cycle phasic systolic vascular bed compression factors that favor reduction in blood flow Intrinsic factors myogenic control Bayliss effect neural components parasympathetic nervous system, sympathetic nervoussystem, coronary reflexes 124 Etiology/Pathophysiology Factors limiting coronary perfusion: coronary reserve diminished at ~85% obstruction critical stenosis occurs when obstructing lesion encroaches on the luminal diameter & exceeds 70% 125 Short-Term Risk of Death or Nonfatal Myocardial Infarction in Patients with Unstable Angina Feature High Risk (At least 1 of the following features must be present) Accelerating tempo of ischemic symptoms in preceding 48 h Intermediate Risk (No high-risk feature but must have 1 of the following) History Prior Ml, peripheral or cerebrovascular disease, or CABG, prior aspirin use Character of pain Prolonged ongoing (> 20 min), Prolonged (> 20 min), rest rest pain angina, now resolved, with moderate or high likelihood of CAD Low Risk (No high- or intermediate-risk feature but may have any of the following) New-onset CCS class III or IV angina in the past 2 weeks without prolonged (> 20 min) rest pain but with moderate or high likelihood of CAD Clinical findings Pulmonary edema, most likely caused by ischemia New or worsening MR murmur S3 or new/worsening rales Hypotension, bradycardia, tachycardia Age > 75 y ECG Angina at rest with transient ST- T-wave inversions > 0.2 mV Normal or unchanged ECG segment changes > 0.05 mV Pathologic Q waves during an episode of chest Bundle-branch block, new or discomfort presumed new Cardiac markers Markedly elevated (e.g., TnT or Slightly elevated (e.g., TnT > Normal TnI > 0.1 ng/mL) 0.01 but < 0.1 ng/mL) CABG, coronary artery bypass grafting; CAD, coronary artery disease; CCS, Canadian Cardiovascular Society; ECG, electrocardiogram; Ml, myocardial infarction; MR, mitral regurgitation; Tnl, troponin; TnT, troponin T. DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM: Pharmacotherapy: A Pathophysiologic Approach, 7th Edition: 126 http://www.accesspharmacy.com NORMAL & ABNORMAL CARDIAC CONDUCTION & ELECTROPHYSIOLOGY mechanical activity of heart (contraction of the atria & ventricles) occurs as a result of its electrical activity. Electrical depolarization of the atria results in atrial contraction, & ventricular depolarization is followed by ventricular contraction. The Cardiac Conduction System Under normal circumstances, SA node serves as pacemaker of heart (because of greater automaticity) & generates the electrical impulses → atrial ventricular depolarization if the SA node fails to generate depolarizations at rate faster than that of AV node → AV node may take over as pacemaker. if the SA node & AV node fail to generate depolarizations at a rate > 30-40/min. → ventricular tissue may take over as the pacemaker. The Ventricular Action Potential Myocyte resting membrane potential is usually –70- –90 mV, due to the action of the sodium-potassium ATPase pump (maintains high extracellular Na+ concentrations & low extracellular K+ concentrations. During each AP cycle, potential of membrane ↑ to a threshold potential, usually –60- –80 mV → fast Na+ channels open → Na+ rapidly enters the cell. → vertical upstroke of AP → potential reaches 20-30 mV. = phase 0 (ventricular depolarization) → fast Na+ channels become inactivated → ventricular repolarization begins The Ventricular Action Potential (cont’d) phases 1-4 of AP represent ventricular repolarization Phase 1 repolarization: efflux of K+ ions Phase 2 repolarization: K+ continues to exit the cell, but the membrane potential is balanced by an influx of Ca++ & Na+ ions, transported through slow Ca++ & slow Na+ channels → plateau Phase 3: efflux of K+ greatly exceeds Ca++ & Na+ influx → major component of ventricular repolarization Phase 4: Na+ ions are actively pumped out via Na+-K+ ATPase pump→ restoration of membrane potential to its resting value The ventricular AP Electrocardiogram (ECG) P wave = atrial depolarization QRS complex = phase 0 of ventricular AP (ventricular depolarization) T wave = phase 3 repolarization of ventricles Atrial repolarization is not displayed on ECG, because it occurs during ventricular depolarization & is obscured by QRS complex PR interval (N= 0.12-0.2 sec) = time of conduction of impulses from atria to ventricles through AV node QRS duration (N= 0.08-0.12) = time required for ventricular depolarization ECG (cont’d) QT interval (from beginning of Q wave to end of T wave) = time required for ventricular repolarization the faster the heart rate, the shorter the QT interval, & vice versa. → QT interval is corrected for heart rate using Bazett’s equation: QTc is the QT interval corrected for rate, RR is interval from onset of one QRS complex to onset of the next QRS complex normal QTc interval in adults is 0.36-0.44 seconds. Refractory Periods a period of time during which cells and fibers cannot be depolarized again is referred to as the absolute refractory period - corresponds to phases 1, 2, & ~half of phase 3 repolarization on AP = period from Q wave to ~ first half of T wave on ECG if there is a premature stimulus for electrical impulse, this impulse cannot be conducted, because the tissue is absolutely refractory following absolute refractory period there is relative refractory period =latter half of phase 3 repolarization on AP= latter half of T wave on ECG if new (premature) electrical stimulus is initiated during relative refractory period, it can be conducted abnormally, potentially in arrhythmia Mechanisms of Cardiac Arrhythmias (1)Abnormal impulse formation; (2)abnormal impulse conduction; or (3) both Mechanisms of Arrhythmias (cont’d) 1. Abnormal Impulse Initiation May result from abnormal ↑ automaticity of SA node →↑ rate of generation of impulses & sinus tachycardia. If rate of initiation of spontaneous impulses by other cardiac fibers becomes abnormally automatic & exceeds that of the SA node → other types of tachyarrhythmias: premature atrial contractions, precipitation of atrial tachycardia or atrial fibrillation (AF) Abnormal automaticity in the ventricles → ventricular premature depolarizations (VPDs) or may precipitate ventricular tachycardia (VT) or ventricular fibrillation (VF) Mechanisms of Arrhythmias (cont’d) ↑ activity of sympathetic nervous system →↑ automaticity of SA node or other automatic cardiac fibers ↑ activity of parasympathetic nervous system →↓ automaticity Mechanisms of Arrhythmias (cont’d) 2. Abnormal Impulse Conduction: “reentry.” is often result of abnormal automaticity → mechanism is both abnormal impulse formation (automaticity) & abnormal impulse conduction (reentry) 3 conditions must be present: (1) at least 2 pathways down which an electrical impulse may travel (2) a “unidirectional block” in one of the conduction pathways (is sometimes a result of prolonged refractoriness in this pathway) (3) slowing of the velocity of impulse conduction down the other conduction pathway Reentry (1a) 2 pathways for impulse conduction, with bidirectional block in 1 pathway (shaded area) → non-viable reentrant loop (1b) 2 pathways for impulse conduction; slowing of conduction down 1 pathway, with no change in refractory period down the other pathway → unidirectional block. The retrograde impulse may reenter the area of unidirectional block → tachyarrhythmia (2a) 2 pathways for impulse conduction; lack of unidirectional block → potential reentrant pathway is non-viable (2b) 2 pathways for impulse conduction; refractory period is prolonged down 1 pathway, with no change in conduction down the other pathway → unidirectional block. The retrograde impulse may reenter the area of unidirectional block → tachyarrhythmia Mechanisms of Arrhythmias (cont’d) Reasons for prolonged refractoriness &/or slowed impulse conduction velocity in cardiac tissues: myocardial ischemia myocardial infarction, the left atrial or LV hypertrophy HF due to LV dysfunction