Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Intracranial pressure wikipedia , lookup
Cardiac output wikipedia , lookup
Homeostasis wikipedia , lookup
Common raven physiology wikipedia , lookup
Blood pressure wikipedia , lookup
Biofluid dynamics wikipedia , lookup
Blood pressure measurement wikipedia , lookup
Circulatory system wikipedia , lookup
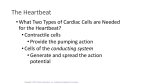
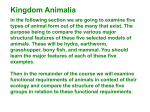
Blood Vessels Blood is carried in a closed system of vessels that begins and ends at the heart In adult, blood vessels stretch 60,000 miles! The three major types of vessels are arteries, capillaries, and veins Arteries carry blood away from the heart (O2 rich, except pulmonary) Veins carry blood toward the heart (O2 poor, except pulmonary) They branch, diverge, fork They join, merge, converge Capillaries contact tissue cells and directly serve cellular needs Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Generalized Structure of Blood Vessels Arteries and veins are composed of three tunics – tunica interna, tunica media, and tunica externa Lumen – central blood-containing space surrounded by tunics Capillaries are composed of endothelium with sparse basal lamina Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Generalized Structure of Blood Vessels Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 19.1b Tunics Tunica interna (tunica intima) Endothelial layer that lines the lumen of all vessels Continuation w/ the endocardial lining of the heart Flat cells, slick surface In vessels larger than 1 mm, a subendothelial connective tissue basement membrane is present Tunica media Circularly arranged smooth muscle and elastic fiber layer, regulated by sympathetic nervous system Controls vasoconstriction/vasodilation of vessels Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Tunics Tunica externa (tunica adventitia) Collagen fibers that protect and reinforce vessels Contains nerve fibers, lymphatic vessels, & elastin fibers Larger vessels contain vasa vasorum (capillary network) that nourish more external tissues of the blood vessel wall Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Blood Vessel Anatomy Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Table 19.1 Elastic (Conducting) Arteries Thick-walled arteries near the heart; the aorta and its major branches Large lumen allow low-resistance conduction of blood Contain elastin in all three tunics Inactive in vasoconstriction Serve as pressure reservoirs expanding and recoiling as blood is ejected from the heart Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Muscular (Distributing) Arteries and Arterioles Muscular arteries – distal to elastic arteries; deliver blood to body organs Account for most of the named structures in lab Have thickest tunica media (proportionally) of all the vessels Active in vasoconstriction Arterioles – smallest arteries; lead to capillary beds Control flow into capillary beds via vasodilation and constriction Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Capillaries Capillaries are the smallest blood vessels (microscopic) Walls consisting of a thin tunica interna, one cell thick Allow only a single RBC to pass at a time Pericytes on the outer surface stabilize their walls Tissues have a rich capillary supply Tendons, ligaments are poorly vascularized Cartilage, cornea, lens, and epithelia lack capillaries Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Vascular Components Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 19.2a, b Types of Capillaries There are three structural types of capillaries: Continuous Fenestrated Sinusoids Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Continuous Capillaries Continuous capillaries are abundant in the skin and muscles Endothelial cells provide an uninterrupted lining Adjacent cells are connected with tight junctions Intercellular clefts allow the passage of fluids & small solutes Brain capillaries do not have clefts (blood-brain barrier) Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Fenestrated Capillaries Found wherever active capillary absorption or filtrate formation occurs (e.g., small intestines, endocrine glands, and kidneys) Characterized by: An endothelium riddled with pores (fenestrations) Greater permeability than other capillaries Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Sinusoids Highly modified, leaky, fenestrated capillaries with large lumens Found in the liver, bone marrow, lymphoid tissue, and in some endocrine organs Allow large molecules (proteins and blood cells) to pass between the blood and surrounding tissues Blood flows sluggishly (e.g. in spleen) allowing for removal of unwanted debris and immunogens Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Capillary Beds A microcirculation moving from arterioles to venules Consist of two types of vessels: Vascular shunts – metarteriole–thoroughfare channel connecting an arteriole directly with a postcapillary venule True capillaries – the actual exchange vessels Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Blood Flow Through Capillary Beds True capillaries: 10-100/bed Branch from, then return to, the capillary bed Precapillary sphincter Cuff of smooth muscle that surrounds each true capillary at the metarteriole and acts as a valve to regulate flow Blood flow is regulated by vasomotor nerves and local chemical conditions True bed is open after meals, closed between meals True bed is rerouted to skeletal muscles during physical exercise Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Capillary Beds Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 19.4a Capillary Beds Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 19.4b Venous System: Venules Venules are formed when capillary beds unite Postcapillary venules – smallest venules, composed of endothelium and a few pericytes Allow fluids and WBCs to pass from the bloodstream to tissues Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Venous System: Veins Veins: Formed when venules converge Composed of three tunics, with a thin tunica media and a thick tunica externa consisting of collagen fibers and elastic networks Accommodate a large blood volume Capacitance vessels (blood reservoirs) that contain 65% of the blood supply Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Venous System: Veins Veins have much lower blood pressure and thinner walls than arteries To return blood to the heart, veins have special adaptations Large-diameter lumens, which offer little resistance to flow Valves (resembling semilunar heart valves), which prevent backflow of blood Venous sinuses – specialized, flattened veins with extremely thin walls (e.g., coronary sinus of the heart and dural sinuses of the brain) Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Vascular Anastomoses Merging blood vessels, more common in veins than arteries Arterial anastomoses provide alternate pathways (collateral channels) for blood to reach a given body region If one branch is blocked, the collateral channel can supply the area with adequate blood supply E.g. occur around joints, abdominal organs, brain, & heart E.g. poorly anastomized organs are retina, kidney, spleen Thoroughfare channels are examples of arteriovenous anastomoses Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Physiology of Circulation: Blood Flow Actual volume of blood flowing in a given period: Is measured in ml per min. Is equivalent to cardiac output (CO), considering the entire vascular system Is relatively constant when at rest Varies widely through individual organs Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Blood Pressure (BP) Force / unit area exerted on the wall of a blood vessel by its contained blood Expressed in millimeters of mercury (mm Hg) Measured in reference to systemic arterial BP in large arteries near the heart The differences in BP within the vascular system provide the driving force that keeps blood moving from higher to lower pressure areas Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Resistance Resistance – opposition to flow (friction) Measure of the amount of friction blood encounters Generally encountered in the systemic circulation away from the heart Referred to as peripheral resistance (PR) The three sources of resistance are: Blood viscosity Total blood vessel length Blood vessel diameter Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Resistance Factors: Viscosity and Vessel Length Resistance factors that remain relatively constant are: Blood viscosity: Internal resistance to flow that exist in all fluids Increased viscosity increases resistance (molecules ability to slide past one another) Blood vessel length: The longer the vessel, the greater the resistance E.g. one extra pound of fat = 1 mile of small vessels required to service it = more resistance Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Resistance Factors: Blood Vessel Diameter Changes in vessel diameter are frequent and significantly alter peripheral resistance Fluid flows slowly Fluid flows freely The smaller the tube the greater the resistance Resistance varies inversely with the fourth power of vessel radius For example, if the radius is doubled, the resistance is 1/16 as much Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Resistance Factors: Blood Vessel Diameter Small-diameter arterioles are the major determinants of peripheral resistance Fatty plaques from atherosclerosis: Cause turbulent blood flow Dramatically increase resistance due to turbulence Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Blood Flow, Blood Pressure, and Resistance Blood flow (F) is directly proportional to the difference in blood pressure (∆P) between two points in the circulation Blood flow is inversely proportional to resistance (R) If ∆P increases, blood flow speeds up; if ∆P decreases, blood flow declines If R increases, blood flow decreases R is more important than ∆P in influencing local blood pressure F = ∆P/R Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Systemic Blood Pressure Any fluid driven by a pump thru a circuit of closed channels operates under pressure The fluid closest to the pump is under the greatest pressure The heart generates blood flow. Pressure results when flow is opposed by resistance…eg. Systemic Blood Pressure Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Systemic Blood Pressure Systemic pressure: Is highest in the aorta Declines throughout the length of the pathway Is 0 mm Hg in the right atrium The steepest change in blood pressure occurs in the arterioles which offer the greatest resistance to blood flow Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Systemic Blood Pressure Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 19.5 Arterial Blood Pressure Arterial BP reflects two factors of the arteries close to the heart Their elasticity (how much they can be stretched) The volume of blood forced into them at any given time Blood pressure in elastic arteries near the heart is pulsatile (BP rises and falls) Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Arterial Blood Pressure Systolic pressure – pressure exerted on arterial walls during left ventricular contraction pushing blood into the aorta (120 mm Hg) Diastolic pressure – aortic SL valve closes preventing backflow and the walls of the aorta recoil resulting in pressure drop lowest level of arterial pressure during a ventricular cycle Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Arterial Blood Pressure Pulse pressure – the difference between systolic and diastolic pressure Felt as a pulse during systole as arteries are expanded Mean arterial pressure (MAP) – pressure that propels the blood to the tissues Because diastole is longer than systole… MAP = diastolic pressure + 1/3 pulse pressure E.g. systolic BP = 120 mm Hg E.g. diastolic BP = 80 mm Hg MAP = 93 MAP & pulse pressure decline w/ distance from the heart At the arterioles blood flow is steady Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Capillary Blood Pressure Capillary BP ranges from 40 (beginning) to 20 (end) mm Hg Low capillary pressure is desirable because high BP would rupture fragile, thin-walled capillaries Low BP is sufficient to force filtrate out into interstitial space and distribute nutrients, gases, and hormones between blood and tissues Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Venous Blood Pressure Venous BP is steady and changes little during the cardiac cycle The pressure gradient in the venous system is only about 20 mm Hg (from venules to venae cavae) vs. 60 mm Hg from the aorta to the arterioles A cut vein has even blood flow; a lacerated artery flows in spurts Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Factors Aiding Venous Return Venous BP alone is too low to promote adequate blood return and is aided by the: Respiratory “pump” – pressure changes created during breathing suck blood toward the heart by squeezing local veins Muscular “pump” – contraction of skeletal muscles surrounding deep veins “pump” blood toward the heart with valves prevent backflow during venous return Smooth muscle contraction of the tunica media by the SNS Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Factors Aiding Venous Return Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 19.6 Maintaining Blood Pressure Maintaining blood pressure requires: Cooperation of the heart, blood vessels, and kidneys Supervision of the brain Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Maintaining Blood Pressure The main factors influencing blood pressure are: Cardiac output (CO) Peripheral resistance (PR) Blood volume Blood pressure = CO x PR Blood pressure varies directly with CO, PR, and blood volume Changes in one (CO, PR, BV) are compensated by the others to maintain BP Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Cardiac Output (CO) CO = stroke volume (ml/beat) x heart rate (beats/min) Units are L/min Cardiac output is determined by venous return and neural and hormonal controls Resting heart rate is controlled by the cardioinhibitory center via the vagus nerves Stroke volume is controlled by venous return (end diastolic volume, or EDV) Under stress, the cardioacceleratory center increases heart rate and stroke volume The end systolic volume (ESV) decreases and MAP increases Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Cardiac Output (CO) Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 19.7 Controls of Blood Pressure Short-term controls: Are mediated by the nervous system and bloodborne chemicals Counteract moment-to-moment fluctuations in blood pressure by altering peripheral resistance Long-term controls regulate blood volume Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Short-Term Mechanisms: Neural Controls Neural controls of peripheral resistance: Alter blood distribution in response to demands Maintain MAP by altering blood vessel diameter Neural controls operate via reflex arcs involving: Baroreceptors & afferent fibers Vasomotor centers of the medulla Vasomotor fibers Vascular smooth muscle Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Short-Term Mechanisms: Vasomotor Center Vasomotor center – a cluster of sympathetic neurons in the medulla that oversees changes in blood vessel diameter Maintains blood vessel tone by innervating smooth muscles of blood vessels, especially arterioles Cardiovascular center – vasomotor center plus the cardiac centers that integrate blood pressure control by altering cardiac output and blood vessel diameter Vasomotor fibers (T1-L2) innervate smooth muscle of the arterioles Vasomotor state is always in a state of moderate constriction Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Short-Term Mechanisms: Vasomotor Activity Sympathetic activity causes: Vasoconstriction and a rise in BP if increased BP to decline to basal levels if decreased Vasomotor activity is modified by: Baroreceptors (pressure-sensitive), chemoreceptors (O2, CO2, and H+ sensitive), higher brain centers, bloodborne chemicals, and hormones Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Short-Term Mechanisms: BaroreceptorInitiated Reflexes When arterial blood pressure rises, it stretches baroreceptos located in the carotid sinuses, aortic arch, walls of most large arteries of the neck & thorax Baroreceptors send impulses to the vasomotor center inhibiting it resulting in vasodilation of arterioles and veins and decreasing blood pressure Venous dilation shifts blood to venous reservoirs causing a decline in venous return and cardiac output Baroreceptors stimulate parasympathetic activity and inhibit the cardioacceletory center to decrease heart rate and contractile force Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Short-Term Mechanisms: BaroreceptorInitiated Reflexes Declining blood pressure stimulates the cardioacceleratory center to: Increase cardiac output and vasoconstriction causing BP to rise Peripheral resistance & cardiac output are regulated together to minimize changes in BP Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Short-Term Mechanisms: Baroreceptor-Initiated Reflexes Baroreceptors respond to rapidly changing conditions like when you change posture They are ineffective against sustained pressure changes, e.g. chronic hypertension, where they will adapt and raise their set-point Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Impulse traveling along afferent nerves from baroreceptors: Stimulate cardioinhibitory center (and inhibit cardioacceleratory center) Baroreceptors in carotid sinuses and aortic arch stimulated Sympathetic impulses to heart ( HR and contractility) CO Inhibit vasomotor center R Rate of vasomotor impulses allows vasodilation ( vessel diameter) Arterial blood pressure rises above normal range Stimulus: Rising blood pressure Im ba la CO and R return blood pressure to Homeostatic range nc e Homeostasis: Blood pressure in normal range Im CO and R return blood pressure to homeostatic range Peripheral resistance (R) Cardiac output (CO) ba la Stimulus: Declining blood pressure nc e Impulses from baroreceptors: Stimulate cardioacceleratory center (and inhibit cardioinhibitory center) Sympathetic impulses to heart ( HR and contractility) Vasomotor fibers stimulate vasoconstriction Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Arterial blood pressure falls below normal range Baroreceptors in carotid sinuses and aortic arch inhibited Stimulate vasomotor center Figure 19.8 Short-Term Mechanisms: Chemical Controls Blood pressure is regulated by chemoreceptor reflexes sensitive to low oxygen and high carbon dioxide levels Prominent chemoreceptors are found in the carotid and aortic bodies Response is to increase cardiac output and vasoconstriction Increased BP speeds the return of blood to the heart and lungs Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Influence of Higher Brain Centers Reflexes that regulate BP are integrated in the medulla Higher brain centers (cortex and hypothalamus) can modify BP via relays to medullary centers Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Chemicals that Increase Blood Pressure Adrenal medulla hormones – norepinephrine and epinephrine increase blood pressure NE has a vasoconstrictive action E increases cardiac output and causes vasodilation in skeletal muscles Nicotine causes vasoconstriction: stimulates sympathetic neurons and the release of large amounts of NE & E Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Chemicals that Increase Blood Pressure Antidiuretic hormone (ADH, aka vasopressin) produced by the hypothalamus causes intense vasoconstriction in cases of extremely low BP stimulates the kidneys to conserve H2O Angiotensin II released when renal perfusion is inadequate The kidney’s release of renin generates angiotensin II, which causes vasoconstriction Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Chemicals that Decrease Blood Pressure Atrial natriuretic peptide (ANP) – produced by the atrium and causes blood volume and pressure to decline along with general vasodilation Nitric oxide (NO) – is a brief but potent vasodilator Inflammatory chemicals – histamine, prostacyclin, and kinins are potent vasodilators Alcohol – causes BP to drop by inhibiting antidiuretic hormone (ADH) Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Long-Term Mechanisms: Renal Regulation Long-term mechanisms control BP by altering blood volume Increased BP stimulates the kidneys to eliminate water, thus reducing BP Decreased BP stimulates the kidneys to increase blood volume and BP Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Kidney Action and Blood Pressure Kidneys act directly and indirectly to maintain long-term blood pressure Direct renal mechanism alters blood volume Indirect renal mechanism involves the reninangiotensin mechanism Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Kidney Action and Blood Pressure: Direct Renal Mechanism Increase in BV causes an increase in BP This stimulates the kidneys to release H2O which lowers BV which in turn lowers BP Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Kidney Action and Blood Pressure: Indirect Renal Mechanism Declining BP causes the release of renin, which triggers the release of angiotensin II Angiotensin II is a potent vasoconstrictor that stimulates aldosterone secretion Aldosterone enhances renal reabsorption resulting in increased BP and BP Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Kidney Action and Blood Pressure Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 19.9 Monitoring Circulatory Efficiency Efficiency of the circulation can be assessed by taking pulse and blood pressure measurements Vital signs – pulse and blood pressure, along with respiratory rate and body temperature Pulse – pressure wave caused by the expansion and recoil of elastic arteries Radial pulse (taken on the radial artery at the wrist) is routinely used Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Palpated Pulse Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 19.11 Measuring Blood Pressure Systemic arterial BP is measured indirectly with the auscultatory method A sphygmomanometer is placed on the arm superior to the elbow Pressure is increased in the cuff until it is greater than systolic pressure in the brachial artery Pressure is released slowly and the examiner listens with a stethoscope Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Measuring Blood Pressure The first sound heard is recorded as the systolic pressure The pressure when sound disappears is recorded as the diastolic pressure Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Alterations in Blood Pressure Normal BP at rest: 110-140 mm Hg (systolic) & 70-80 mm Hg (diastolic) Hypotension – low BP in which systolic pressure is below 100 mm Hg Hypertension – condition of sustained elevated arterial pressure of 140/90 or higher Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Blood Flow Through Tissues Blood flow, or tissue perfusion, is involved in: Delivery of oxygen and nutrients to, and removal of wastes from, tissue cells Gas exchange in the lungs Absorption of nutrients from the digestive tract Urine formation by the kidneys Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Velocity of Blood Flow Blood velocity: Changes as it travels through the systemic circulation Is inversely proportional to the cross-sectional area E.g. Fast in the aorta Slow in capillaries Fast again in the veins Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Velocity of Blood Flow Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 19.13 Autoregulation: Local Regulation of Blood Flow Autoregulation – automatic adjustment of blood flow to each tissue in proportion to its requirements at any given point in time Blood flow through an individual organ is intrinsically controlled by modifying the diameter of local arterioles feeding its capillaries MAP remains constant, while local demands regulate the amount of blood delivered to various areas according to need Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Blood Flow: Skeletal Muscles Capillary density & blood flow is greater in red (slow oxidative) fibers than in white (fast glycolytic) fibers When muscles become active, blood flow to them increases (hyperemia) This autoregulation occurs in response to low O2 levels SNS activity increases causing an increase in NE which causes vasoconstriction of the vessels of blood reservoirs to the skin and viscera diverting blood away to the skeletal muscles Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Blood Flow: Brain Blood flow to the brain is constant, as neurons are intolerant of ischemia Brain cannot store essential nutrients Very precise autoregulatory system, E.g. when you make a fist, blood supply shifts to those neurons in the cerobral motor cortex Metabolic controls – brain tissue is extremely sensitive to declines in pH, and increased carbon dioxide causes marked vasodilation Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Blood Flow: Brain Myogenic controls protect the brain from damaging changes in blood pressure Decreases in MAP cause cerebral vessels to dilate to ensure adequate perfusion Increases in MAP cause cerebral vessels to constrict so smaller vessels do not rupture MAP below 60mm Hg can cause syncope (fainting) Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Blood Flow: Skin Blood flow through the skin: Supplies nutrients to cells in response to oxygen need Helps maintain body temperature Provides a blood reservoir Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Blood Flow: Skin Blood flow to venous plexuses below the skin surface: Varies from 50 ml/min (cold) to 2500 ml/min (hot), depending on body temperature Is controlled by sympathetic nervous system reflexes initiated by temperature receptors and the central nervous system Does this via arteriole-venule shunts located at fingertips, palms, toes, soles of feet, ears, nose, lips Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Temperature Regulation As temperature rises (e.g., heat exposure, fever, vigorous exercise): Hypothalamic signals reduce vasomotor stimulation of the skin vessels Blood flushes into capillary beds Heat radiates from the skin Sweat also causes vasodilation via bradykinin in perspiration Bradykinin stimulates the release of NO which increases vasodilation As temperature decreases, skin vessels constrict and blood is shunted to deeper, more vital organs Rosy cheeks: blood entrapment in superficial capillary loops Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Blood Flow: Lungs (Think Reversal) Blood flow in the pulmonary circulation is unusual in that: The pathway is short Arteries/arterioles are more like veins/venules (thin-walled, with large lumens) Because of this they have a much lower arterial pressure (24/8 mm Hg versus 120/80 mm Hg) Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Blood Flow: Lungs The autoregulatory mechanism is exactly opposite of that in most tissues Low pulmonary oxygen levels cause vasoconstriction; high levels promote vasodilation As lung air sacs fill w/ air, capillary beds dilate to take it up Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Blood Flow: Heart Small vessel coronary circulation is influenced by: Aortic pressure The pumping activity of the ventricles During ventricular systole: Coronary vessels compress Myocardial blood flow ceases Stored myoglobin supplies sufficient oxygen During ventricular diastole, aortic pressure forces blood thru the coronary circulation During exercise, coronary blood vessels dilate in response to elevated CO2 levels Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Capillary Exchange of Respiratory Gases and Nutrients Oxygen, carbon dioxide, nutrients, and metabolic wastes diffuse between the blood and interstitial fluid along concentration gradients Oxygen and nutrients pass from the blood to tissues Carbon dioxide and metabolic wastes pass from tissues to the blood Water-soluble solutes pass through clefts and fenestrations Lipid-soluble molecules diffuse directly through endothelial membranes Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Capillary Exchange of Respiratory Gases and Nutrients Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 19.15.1 Four Routes Across Capillaries Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 19.15.2 Fluid Movement: Bulk Flow Fluid is forced out of capillary beds thru clefts at the arterial end, with most of it returning at the venous end of the bed This process determines relative fluid volume in blood stream and extracellular space Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Capillary Exchange: Fluid Movements Hydrostatic pressure is the force of a fluid pressed against a wall Direction and amount of fluid flow depends upon the difference between: Capillary hydrostatic pressure (HPc) Capillary colloid osmotic pressure (OPc) Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Capillary Exchange: Fluid Movements HPc – pressure of blood against the capillary walls: Tends to force fluids through the capillary walls (filtration) leaving behind cells and proteins Is greater at the arterial end of a bed than at the venule end HPc is opposed by interstitial fluid hydrostatic pressure (HPif) Net pressure is the difference between HPc and HPif Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Colloid Osmotic Pressure The force opposing hydrostatic pressure (HPc) OPc– created by nondiffusible plasma proteins, which draw water toward themselves (osmosis) E.g. serum albumin OPc does not vary from one end of the capillary bed to the other Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Net Filtration Pressure (NFP) Hydrostatic-Osmotic Pressure interactions determine if there is a net gain or loss of fluid from the blood, calculated as the Net Filtration Pressure (NFP) NFP – all the forces acting on a capillary bed Thus, fluid will leave the capillary bed if the NFP is greater than the net OP and vice versa Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Net Filtration Pressure (NFP) At the arterial end of a bed, hydrostatic forces dominate (fluids flow out) At the venous end of a bed, osmotic forces dominate (fluids flow in) More fluids enter the tissue beds than return to the blood, and the excess fluid is returned to the blood via the lymphatic system Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Net Filtration Pressure (NFP) Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 19.16 Circulatory Shock Circulatory shock – any condition in which blood vessels are inadequately filled and blood cannot circulate normally E.g. hypovolemic shock: large scale blood loss Blood volume decreases causing an increase in heart rate resulting in a weak pulse Vasoconstriction occurs enhancing venous return Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Circulatory Shock Vascular Shock: Blood volume is normal, but circulation is poor as a result of an abnormal expansion of the vascular bed caused by extreme vasodilation Results in rapid fall in blood pressure Most common cause is anaphylactic shock Body-wide vasodilation due to massive histamine release Neurogenic shock: failure of ANS regulation Septic shock (septicemia): severe systemic bacterial infection Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Copyright © 2006 Pearson Education, Inc., publishing as Benjamin Cummings Figure 19.17