Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
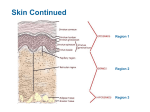
The Integumentary System – Consists of the skin and its accessory organs; hair, nails, and cutaneous glands • Inspection of the skin, hair, and nails is significant part of a physical exam • Skin is the most vulnerable organ – Exposed to radiation, trauma, infection, and injurious chemicals • Receives more medical treatment than any other organ system • Dermatology—scientific study and medical treatment of the integumentary system Functions of the Skin • Resistance to trauma and infection, protection • Other barrier functions – Waterproofing, UV radiation • Vitamin D synthesis – Skin first step, liver and kidneys complete the process • Sensation • Thermoregulation – Vasoconstriction/vasodilation • Transdermal absorption – Administration of certain drugs steadily through thin skin via adhesive patches The Skin and Subcutaneous Tissue • The body’s largest and heaviest organ – 15% of body weight – Most skin is 1 to 2 mm thick • Two layers – Epidermis: stratified squamous epithelium – Dermis: connective tissue layer – Hypodermis—another connective tissue layer below the dermis • Thick skin—on palms and sole, and corresponding surfaces on fingers and toes – Has sweat glands, but no hair follicles or sebaceous (oil) glands – Epidermis 0.5 mm thick • Thin skin covers rest of the body – Epidermis about 0.1 mm thick – Possesses hair follicles, sebaceous glands, and sweat glands The Integumentary System (Skin) The Epidermis – Dead cells at the surface packed with tough protein called keratin – Lacks blood vessels, has some verve endings for touch and pain. – Depends on the diffusion of nutrients from underlying connective tissue • Composed of stratified squamous epithelium which can be 20 40 cell layers thick depending on location – the major cell type is the keratinocyte • The cells of the epidermis are arranged into 5 structurally and functionally distinct layers called strata – each strata is made of one or more types of cells each providing a specific function for the epidermis Cells of the Epidermis 1. Stem cells • Undifferentiated cells that give rise to keratinocytes • In deepest layer of epidermis (stratum basale) 2. Keratinocytes: synthesize keratin 3. Melanocytes • Occur only in stratum basale • Synthesize pigment melanin that shields DNA from ultraviolet radiation 4. Tactile (Merkel) cells • Touch receptor cells in basal layer associated with dermal nerve fibers 5. Dendritic (Langerhans) cells • Macrophages found in stratum spinosum and granulosum • Guard against toxins, microbes, pathogens that penetrate skin Cells of the Epidermis Sweat pore Stratum corneum Stratum lucidum Stratum granulosum Exfoliating keratinocytes Dead keratinocytes Sweat duct Living keratinocytes Stratum spinosum Dendritic cell Tactile cell Melanocyte Stem cell Stratum basale Dermal papilla Tactile nerve fiber Dermis Dermal blood vessels Layers of the Epidermis • The most superficial layer of the epidermis are the cells that are subjected to the physical forces that come from the outside of the body – friction, abrasion, puncture… • As a result, these cells continuously fall off from the surface of the skin – exfoliation • The exfoliated cells are constantly replaced by cells in the deepest strata of the epidermis which are constantly dividing (mitosis) maintaining a constant epidermal thickness – the rate of mitosis equals the rate of exfoliation Stratum Corneum • Outermost strata made of keratinized cells • Resistant to abrasion, penetration, and water loss • Made of up to 30 layers of dead keratinocytes – accounts for up to 75% of the epidermal thickness • Most superficial layer of keratinocytes exfoliate from the surface of the body Stratum Lucidum • Thin translucent zone seen only in thick skin found on the palms of the hand and souls of the feet (calluses) • Cells have no nucleus or organelles Stratum Granulosum • Three to five cell layers deep made of keratinocytes • Keratinocytes accumulate vesicles (granules) filled with the protein keratin and glycolipids which are exocytosed – the exocytosed keratin wraps around the cell membrane of the keratinocyte creating a thick coat which provides protection from abrasion and puncture – the exocytosed glycolipids fills the extracellular spaces between the keratinocytes and provides a waterproofing property to skin • forms a barrier between surface cells and deeper layers of the epidermis • cuts off nutrient supply to the cells of the lucidum and corneum to die Stratum Spinosum Several cell layers deep made of: • Keratinocytes – become somewhat flattened and “spiny-shaped” • Langerhans (dendritic) cells – phagocytose foreign substances such as bacteria and viruses that attempt to enter the body through the skin – alert the immune system to the presence of foreign substances Stratum Basale (germinativum) Deepest of the epidermal strata made of a single layer of cells (consisting of 3 cell types) • Keratinocytes – undergo mitosis rapidly to replace the cells that are exfoliated from the surface – as these keratinocytes “move” up through the more superficial strata • Melanocytes – produce the brown pigment melanin to protect against UV radiation (sunlight) damage to DNA of keratinocytes • Merkel (tactile) cells – touch receptors that provide sensory perception Melanocytes • Occur only in the stratum basale • Melanin is shed from the melanocytes onto neighboring keratinocytes of the strata spinosum and basale. – 2 Forms of Melanin • Eumelanin: brownish-black pigment. • Pheomelanin: reddish-yellow, sulfur-containing pigment. • Dark skin: produces greater quantities of melanin, and breaks it down more slowly. Melanin will accumulate into several epidermal layers. • Light skin: produces less melanin, and breaks it down quickly so that it doesn’t spread beyond the stratum basale. • UV exposure increases the productivity of melanocytes. The Dermis • Dermis—connective tissue layer beneath the epidermis – Ranges from 0.2 mm (eyelids) to 4 mm (palms, soles) – Composed mainly of collagen with elastic fibers, reticular fibers, and fibroblasts – Well supplied with blood vessels, sweat glands, sebaceous glands, and nerve endings • 2 Layers: – Papillary layer – Reticular layer Dermis Papillary layer Reticular layer The Dermis • Papillary layer—superficial zone of dermis – Thin zone of areolar tissue in and near the dermal papilla – Allows for mobility of leukocytes and other defense cells should epidermis become broken – Rich in small blood vessels – 20% of the thickness of the dermis – Its superior surface contains fingerlike projections called dermal papillae which keep it firmly attached to the superficially located epidermis – Dermal papillae contain sensory receptors such as tactile corpuscles (touch receptors) and free nerve endings (sense pain) • Reticular layer – 80% of the thickness of the dermis – Elastic fibers provide stretch-recoil properties – Location of: • hair and associated follicles • pacinian corpuscles (pressure receptors) • blood vessels • glands The Hypodermis • Hypodermis – Subcutaneous tissue – Mostly adipose – Pads body – Binds skin to underlying tissues • Drugs introduced by injection – Highly vascular and absorbs them quickly • Subcutaneous fat – Energy reservoir – Thermal insulation – 8% thicker in women Skin Colors of diagnostic value • Cyanosis—blueness of the skin from deficiency of oxygen in the circulating blood (airway obstruction, lung disease, cardiac arrest, cold weather) • Erythema—abnormal redness of the skin due to dilated cutaneous vessels (exercise, hot weather, sunburn, anger, or embarrassment) • Pallor—pale or ashen color when there is so little blood flow through the skin that the white color of dermal collagen is visible (emotional stress, low blood pressure, circulatory shock, cold, anemia) • Albinism—genetic lack of melanin that results in white hair, pale skin, and pink eyes • Jaundice—yellowing of skin and sclera due to excess of bilirubin in blood (cancer, hepatitis, cirrhosis) • Hematoma (bruise)—mass of clotted blood showing through skin Hair • Filamentous strands of dead keratinized cells produced by hair follicles • Contains hard keratin which is tougher and more durable than the soft keratin of the epidermis • The long thin hair shaft is visible above epidermis • The hair root is in the dermis within a follicle • Pigmented by melanocytes at the base of the follicle Hair Function and Distribution • Hair is distributed over the entire skin surface except – palms, soles, and lips, nipples and portions of the external genitalia • Functions of hair include: – Retain body heat • The follicle of the hair is connected to piloerector muscles that contract when cold – raises hair on skin surface (goose bumps) increasing the thickness of the insulation barrier at the surface of the skin – Provide sensory perception • Limbs and trunk have 55 to 70 hairs per cm2 – Face about 10 times as many – 30,000 hairs in a man’s beard – 100,000 hairs on an average person’s scalp – Number of hairs does not differ much from person to person or even between sexes Structure of the Hair and Follicle Hair shaft Sebaceous gland Piloerector muscle Hair receptor Bulge Hair root Hair matrix Hair bulb Apocrine sweat gland Blood capillaries in dermal papilla (a) Dermal papilla • Hair is divisible into three zones along its length – Bulb: a swelling at the base where hair originates in dermis or hypodermis • Only living hair cells are in or near bulb – Root: the remainder of the hair in the follicle – Shaft: the portion above the skin surface • Dermal papilla—bud of vascular connective tissue encased by bulb – Provides the hair with its sole source of nutrition • Hair matrix—region of mitotically active cells immediately above papilla – Hair’s growth center • Three layers of the hair in cross section from inside out – Medulla • Core of loosely arranged cells and air spaces – Cortex • Constitutes bulk of the hair – Cuticle • Composed of multiple layers of very thin, scaly cells that overlap each other Connective tissue root sheath Epithelial root sheath Hair medulla Hair cortex Hair matrix Hair bulb Dermal papilla (b) 0.5 mm Hair Texture and Color • Texture—related to differences in cross-sectional shape – Straight hair is round – Wavy hair is oval – Curly hair is relatively flat • Color—due to pigment granules in the cells of the cortex – Brown and black hair is rich in eumelanin – Red hair has a slight amount of eumelanin but a high concentration of pheomelanin – Blond hair has an intermediate amount of pheomelanin and very little eumelanin – Gray and white hair results from scarcity or absence of melanin in the cortex and the presence of air in the medulla Hair Texture and Color Three layers of hair (c.s.) • Medulla – Core of cells and air spaces • Cortex – Constitutes bulk of the hair, several layers of keratinized cells • Cuticle – multiple layers of very thin, scaly cells that overlap each other Eumelanin Pheomelanin Cuticle Cortex (c) Red, wavy Air space Eumelanin Pheomelanin Medulla (b) Black, straight (a) Blond, straight (d) Gray, wavy Hair Growth • The Hair Cycle: – 3 Stages: • Anagen: 90% of hair, hair cells multiply in the follicle and push the hair deeper into the dermis. Also forms the hair root sheath. Hair root sheath cells transform into hair cells which produce keratin and then die as they are pushed away from the papilla. • Catagen: Mitosis in the sheath ceases. The base of the hair hardens and is no longer anchored in the papilla. • Telogen: Rest period. *When anagen begins anew, the new hair will push out the old. Nails • • hard derivatives of the stratum corneum. composed of very thin, dead, densely packed cells, filled with parallel fibers of hard keratin. – Nail plate: the hard part of the nail. – Free edge: end which overhangs the tip of the finger or toe. – Nail body: the visible attached portion of the nail. – Nail root: extends proximally under the overlying skin. – Nail bed: the skin underlying the nail plate. It’s epidermis is called the hyponychium. Nail matrix: A growth zone at the proximal end of the nail, composed of stratum basale. Mitosis (1mm/week). Lunule: white crescent at the proximal end of a nail. Cuticle (eponychium): a narrow zone of dead skin. Exocrine glands of the skin • Sweat glands – merocrine sweat glands • secrete water to cool of the body – apocrine sweat glands • scent glands that secrete a milky substance rich in fatty acids in response to stress or sexual stimulation • Sebaceous glands – secrete an oily substance (sebum) into a hair follicle • softens the skin • Ceruminous glands – secrete a waxy substance (cerumen) in the ear canal • keeps eardrum flexible • kills bacteria Skin Cancer • Skin cancer—induced by the UV rays of the sun – – – – – Most often on the head and neck Most common in fair-skinned people and the elderly One of the most common cancer One of the easiest to treat Has one of the highest survival rates if detected and treated early • Three types of skin cancer named for the epidermal cells in which they originate – Basal cell carcinoma, squamous cell carcinoma, and malignant melanoma Skin Cancer (a) Basal cell carcinoma • Basal cell carcinoma - Most common type - Least dangerous because it seldom metastasizes - Forms from cells in stratum basale - Lesion is small, shiny bump with central depression and beaded edges Skin Cancer (b) Squamous cell carcinoma • Squamous cell carcinoma - Arise from keratinocytes from stratum spinosum - Lesions usually appear on scalp, ears, lower lip, or back of the hand - Have raised, reddened, scaly appearance later forming a concave ulcer - Chance of recovery good with early detection and surgical removal - Tends to metastasize to lymph nodes and may become lethal Skin Cancer (c) Malignant melanoma • Malignant melanoma - Skin cancer that arises from melanocytes; often in a preexisting mole - Less than 5% of skin cancers, but most deadly form - Treated surgically if caught early - Metastasizes rapidly; unresponsive to chemotherapy; usually fatal Burns • Classified according to the depth of tissue involvement • First-degree burn: partial-thickness burn; involves only the epidermis • Marked by redness, slight edema, and pain • Heals in a few days – Most sunburns are first-degree burns • Second-degree burn: partial-thickness burn; involves the epidermis and part of the dermis • Leaves part of the dermis intact • Red, tan, or white • Two weeks to several months to heal and may leave scars • Blistered and very painful • Third-degree burn: full-thickness burn; the epidermis and all of the dermis, and often some deeper tissues (muscles or bones) are destroyed • Often requires skin grafts • Needs fluid replacement and infection control Degrees of Burn Injuries Partial-thickness burns (a) First degree Full-thickness burns (b) Second degree (c) Third degree Tissue Repair • Damaged tissues can be repaired in two ways: – Regeneration: replacement of dead or damaged cells by the same type of cell as before • Restores normal function • Skin injuries and liver regenerate – Fibrosis: replacement of damaged cells with scar tissue • Holds organs together • Does not restore normal function – Severe cuts and burns, healing of muscle injuries, scarring of lungs in tuberculosis • Healing of a cut in the skin: – Severed blood vessels bleed into cut – Mast cells and damaged cells release histamine – Dilates blood vessels – Increases blood flow to area – Makes capillaries more permeable 1 Bleeding into the wound • Blood plasma seeps into the wound carrying: – Antibodies – Clotting proteins – Blood cells • Blood clot forms in the tissue – Loosely knitting edges of cut together – Inhibits spread of pathogens from injury site to healthy tissue Scab Blood clot • Forms scab that temporarily seals wound and blocks infection • Macrophages phagocytize and digest tissue debris Macrophages Fibroblasts Leukocytes 2 Scab formation and macrophage activity • New capillaries sprout from nearby vessels and grow into wound • Deeper portions become infiltrated by capillaries and fibroblasts Scab – Macrophages remove the blood clot Blood capillary – Fibroblasts deposit new Granulation collagen tissue – Begins 3–4 days after injury and lasts up to 2 weeks Macrophages Fibroblasts 3 Formation of granulation tissue (fibroblastic phase of repair) Tissue Repair • Surface epithelial cells around wound multiply and migrate into wound area beneath scab • Epithelium regenerates • Connective tissue undergoes fibrosis • Scar tissue may or may not show Epidermal through epithelium regrowth tissue • Remodeling (maturation) phase Scar (fibrosis) begins several weeks after injury and may last up to 2 years 4 Epithelial regeneration and connective tissue fibrosis (remodeling phase of repair)